


1Doctorate School, Universidad Católica de Valencia San Vicente Mártir, València, Spain, 2Dermatology, Clinica San Carlo, Paderno Dugnano, Italy, 3Department of Dermatology, Instituto Valenciano de Oncología, València, 4Department of Dermatology, Hospital Carlos Haya, Málaga, 5Department of Pathology, Instituto Valenciano de Oncología, and 6School of Medicine, Universidad Católica de Valencia San Vicente Mártir, València, Spain
#These authors contributed equally to this work.
Locoregional lymph node recurrences of primary trunk melanoma can occur in basins not identified during sentinel lymph node biopsy. However, the factors associated with recurrences in non-sentinel lymph node basins are unknown. To evaluate these factors, this observational retrospective study examined the patterns of first lymph node recurrence and the factors associated with recurrence in non-sentinel lymph node basins. A total of 305 patients with primary trunk melanoma who had undergone sentinel lymph node biopsy from 2000 to 2015 were evaluated. Twenty-three patients presented locoregional lymph node recurrence; 8 of which (34.8%) were in non-sentinel lymph node basins. Non-sentinel lymph node recurrences were more frequent in patients with positive sentinel lymph nodes and in those patients whose number of tumour-involved nodes was > 3. These results suggest that clinical examination and ultrasound surveillance should be performed on all potential lymph node drain-age basins of trunk melanomas.
Key words: melanoma; lymph node; recurrence; trunk.
Accepted Sep 15, 2020; Epub ahead of print Sep 18, 2020
Acta Derm Venereol 2020; 100: adv00284.
doi: 10.2340/00015555-3635
Corr: Eduardo Nagore, Universidad Católica de Valencia San Vicente Mártir, c/ Quevedo, 2, ES-46001 València, Spain. Email: eduardo.nagore@ucv.es
Locoregional lymph node recurrences of trunk melanoma can occur in basins not identified during sentinel lymph node biopsy. In this study, 23 out of 305 trunk melanoma patients presented locoregional lymph node recurrence, with one-third of these in non-sentinel lymph node basins. This suggests that clinical examination and ultrasound surveillance should be performed on all potential lymph node drainage basins of trunk melanomas.
The trunk site of melanoma represents a negative prognostic factor in patients with melanoma although the reason remains uncertain (1–3). Even after introduction of lymphoscintigraphy and sentinel lymph node biopsy (SLNB), unpredictable drainage patterns may still occur in trunk melanoma (4–6). Indeed, lymphatic drainage to multiple basins (MLBD) is observed in approximately 20–30% of patients with primary trunk melanoma, although its prognostic impact remains controversial (7–13). Moreover, SLNB and lymphadenectomy can modify lymphatic drainage, which could indicate new drainage basins other than those detected during SLNB.
Identification and evaluation of lymph drainage basins is mandatory because the presence of lymph node (LN) metastases is the strongest prognostic factor for recurrence and survival in patients with melanoma (14).
Despite the extensive literature about SLNB, no data are available detailing the pattern of LN recurrences in non-sentinel lymph node (NSLN) basins vs sentinel lymph node (SLN) basins. However, in our clinical experience, there are patients who present locoregional LN recurrence in basins not identified during lympho-scintigraphy and SLNB.
This study retrospectively reviewed a case series of patients with trunk melanoma, with the aim of evaluating the patterns of first recurrence in locoregional LNs and identifying factors that can be associated with recurrence in NSLN basins.
Patient population
An observational retrospective study was performed, based on 305 patients with primary trunk melanoma who had undergone lymphatic mapping and SLNB from 2000 to 2015 at our institution.
The data were retrieved from the melanoma database of the Instituto Valenciano de Oncología (IVO) of València. This database contains prospectively recorded data of patients with melanoma who were diagnosed and treated at the IVO since 1 January 2000. The database meets all legal requirements and was approved by the ethics committee of the IVO. All patients gave written permission to be included in the database and to participate in this study.
Guidelines for staging procedure in our centre included SLNB for all melanomas thicker than 0.75 mm and those thinner than or equal to 0.75 mm if the tumour was ulcerated, had vascular invasion, a microscopic satellite, and/or the presence of at least one mitosis in the dermal component.
Inclusion criteria included 2 parameters: (i) diagnosed with primary trunk melanoma in clinical stage I or II; and (ii) underwent SLNB.
Patients with unidentified SLN, multiple invasive melanomas, in situ melanoma, clinically detected tumour-involved node (TIN), or radiological evidence of regional and/or distant metastases were excluded.
The main outcome of the study was the development of loco-regional LN recurrence during follow-up. Locoregional LN recurrence was defined as the appearance of LN metastasis in one or more than one of the potential LN drainage basins of trunk melanoma, confirmed by histological analysis. Only first LN recurrences, either alone or synchronous with other distant or locoregional cutaneous recurrences, were included in this study.
LN recurrences were classified based on the site: (i) SLN basin if the metastasis appeared in a basin detected during SLNB regard-less of the status (negative or positive); or (ii) NSLN basin.
Sex, age at diagnosis (< 45 vs 45–60 vs > 60 years), trunk site (superior central vs superior lateral vs inferior central vs inferior lateral and anterior vs posterior), Breslow thickness (≤ 2 mm vs > 2 mm), ulceration status, vascular invasion status, presence of microscopic satellite or not, number of LN basin drainage (1 vs 2 vs 3), number of SLNs (1 vs 2 vs 3+), SLN status, and number of TINs (0 vs 1–3 vs > 3) were included as covariates.
The study was approved by the local ethics committee, and patients provided informed consent.
Sentinel lymph node biopsy technique
SLNs were detected using a lymphoscintigraphy protocol with Tc99m and intradermal injection of blue dye around the surgical scar of melanoma.
All radiolabelled LNs and/or those that appeared blue-stained during surgery were considered SLNs and were excised. After removing the SLNs, the surgeon ensured that no radiolabelled or blue-stained tissue remained in the basin. SLNs were then classified depending on size. SLNs ≤ 5 mm were bisected, while SLNs > 5 mm were sectioned every 2–3 mm parallel to the short axis. After a 24-h fixation in buffered formalin, SLN specimens were embedded in paraffin blocks. Finally, 3 histological sections were realized every 250 µm until the whole block was gone. One section was stained with haematoxylin and eosin, one with S-100, and one with Human Melanoma Black (HMB45).
Complete lymph node dissection (CLND) was performed in all patients with positive SLN unless contraindicated or declined by the patient.
Statistical analysis
All the variables analysed were expressed categorically. Differences in the distribution of each variable between the defined groups were assessed by contingency tables, and the significance was analysed by χ2 and Fisher’s exact tests. Survival estimates were derived using the Kaplan–Meier method, in which the event was the development of locoregional LN metastases. Patients who did not develop LN recurrence or who died by the last date of follow-up were censored. Differences in survival by each variable value were evaluated using the log-rank test. Multivariate analyses were carried out using a stepwise forward Cox proportional hazard method. In these models, all covariates that were statistically significant based on the log rank test were included. A classification and regression tree (CART) analysis was used to hierarchically stratify the variables associated with NSLN basin recurrence. All tests were 2-sided, and the level of significance was set at alpha < 0.05. Statistical analyses were performed using IBM SPSS 20.0 (IBM SPSS statistics, IL, USA).
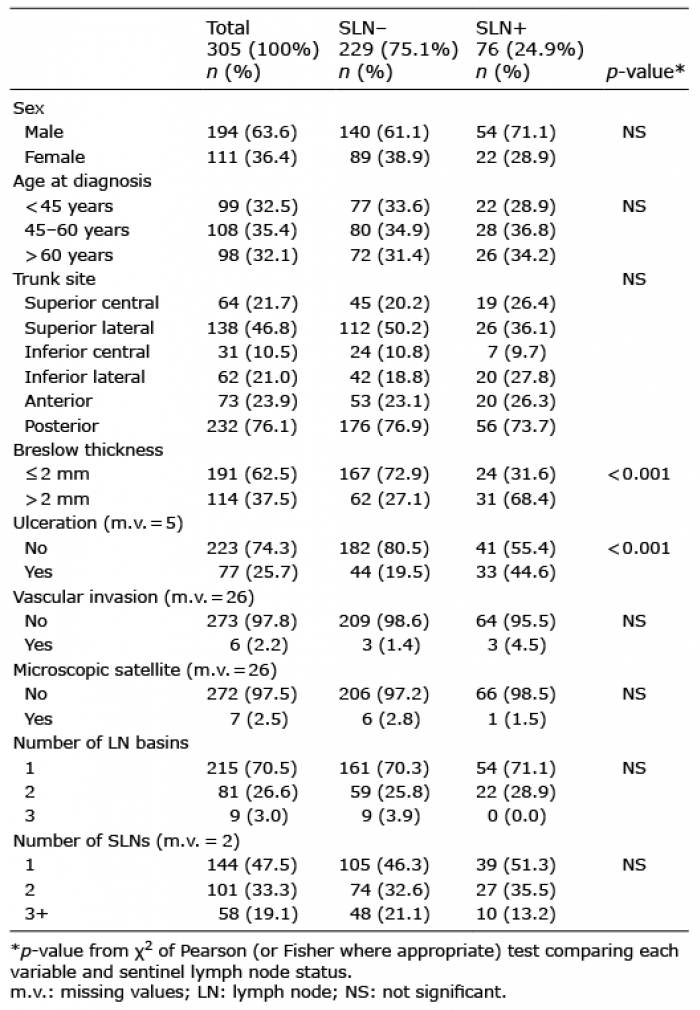
The study population consisted of 305 patients, 194 (63.6%) males and 111 (36.4%) females with a median age of 52 years (interquartile range (IQR) 40.5–64). MLBD was present in 90 (29.5%) patients; 81 had dual basin drainage, and 9 underwent triple basin drainage. Seventy-six patients out of 305 (24.9%) had a histologically positive SLNB result. Of those patients, 72 were treated with CLND. The clinical-pathological character-istics are listed in Table I.
Table I. Clinical and pathological characteristics of trunk melanomas and their correlation with sentinel lymph node (SLN) status
Factors associated with lymph node recurrence
After a median follow-up of 70 months (IQR 32–112), 23 patients presented locoregional LN recurrence, 11 of them with previous positive SLN (Fig. 1). All of the 11 SLN-positive patients underwent CLND. None of the 4 SLN-positive patients who were not treated with CLND developed LN recurrence. Factors predicting a shorter time for LN recurrence included increasing number of TINs (log rank, p < 0.001), Breslow > 2 mm (log rank, p < 0.001), ulceration (log rank, p = 0.003), positive SLN (log rank, p = 0.007), vascular invasion (log rank, p = 0.007), and male sex (log rank, p = 0.049) as indicated in Fig. 2. Multivariate Cox-regression showed that a shorter time of LN recurrence was statistically associated with number of TINs (>3 vs 0; hazard ratio (HR) 17.2; 95% confidence interval (CI) 4.4–66.6; p < 0.001) and Breslow thickness (> 2 mm vs ≤ 2 mm; HR 10.0; 95% CI 2.836–6.00; p < 0.001) as shown in Table II.
Fig. 1. Pattern of lymph node recurrence. Eight out of 23 lymph node (LN) recurrences appeared in non-sentinel lymph node (NSLN) basins. SLNB: sentinel lymph node biopsy; SLN: sentinel lymph node.
Fig. 2. Kaplan–Meier curves depicting lymph node recurrence per covariate. (A) Number of tumor-involved nodes; (B) Breslow thickness; (C) sentinel lymph node (SLN) status; (D) absence or presence of ulceration; (E) absence or presence of vascular invasion; (F) sex. No.: number of patients.
Table II. Multivariate stepwise forward Cox-regression of factors predicting a shorter time of lymph node and non-sentinel lymph node (NSLN) recurrence
Factors associated with recurrence in non-sentinel lymph node basins
Eight out of 23 LN recurrences (34.8%) occurred in NSLN basins (Fig. 1). Five of them (62.5%) occurred in ipsilateral basins, and 3 (37.5%) occurred in contralateral basins. Six out of 8 (75%) had previous positive SLNs and had undergone CLND. Kaplan–Meier curves showed that recurrences in NSLN basins developed earlier in patients who had an increase in the number of TINs (log rank, p < 0.001), positive SLN (log rank, p = 0.001), Breslow > 2 mm (log rank, p = 0.002), ulceration (log rank, p = 0.016), and vascular invasion (log rank, p = 0.019). After multivariate analysis, only an increase in the number of TINs (> 3 vs 0; HR 180.1; 95% CI 15.5–2093.0; p < 0.001; 1–3 vs 0; HR 14.0; 95% CI HR 1.6–125.1; p = 0.018) was included in the final model associated with recurrence in NSLN basins (Table II). CART analy-sis showed that NSLN basins recurrences were more frequent: (i) in patients with positive SLNs and whose number of TINs was > 3 (2 out of 4; 50%); (ii) in patients with positive SLN, whose number of TINs was 1–3 (4 out of 72; 5.6%), and (iii) in patients with negative SLN (2 out of 229; 0.9%), as shown in Fig. 3. No significant association between recurrence in a NSLN basin and number of LN basins was noted although 3 out of 8 had dual basin drainage.
Fig. 3. Classification and regression tree of covariates associated to non-sentinel lymph node (NSLN) basin recurrences. Patients with positive sentinel lymph node (SLN) and whose number of tumour-involved nodes (TINs) was >3 had the higher percentage of non-sentinel lymph node basin recurrence.
This study analysed 305 patients with trunk melanoma who underwent SLNB over a 15-year period at our institution. Of this population, 76 presented with positive SLNs, and all but 4 patients were treated with CLND. During the study period, 23 cases of locoregional LN recurrences were observed, of which 11 were in SLN-positive basins and 12 in SLN-negative. Finally, 8 of the locoregional LN recurrence occurred in a NSLN basin.
SLN positivity was observed in 24.9% of the patients. Factors associated with a positive SLN were Breslow thickness and ulceration, coherently with the published literature (9, 11, 12, 15–18).
Numerous studies have shown that trunk melanoma is an independent indicator for decreased survival and increased risk of recurrence in patients with melanoma, being part of the back and breast (Thorax), upper arm, neck, and scalp (TANS) region (1–3). The reason for this finding is unknown, but may be due to the unpredictable lymphatic drainage of trunk melanoma. Ideally, a melanoma located in the upper trunk (above the Sappey’s line) will drain into the ipsilateral axilla, but it can also drain into the ipsilateral groin and/or the contralateral axilla and/or groin. This unpredictability appears to happen in more than half of cases and is more frequent if the melanoma is located on or below Sappey’s line and on the midline. Moreover, unusual locations of SLNs have been reported in nearly 7% of trunk melanomas with the triangular intermuscular space being one of the most common sites to harbour ectopic/interval SLNs (4–6) (Fig. 4).
Fig. 4. Sappey’s line and midline (red lines), and cutaneous projections of the triangular intermuscular space (green triangles). The skin overlying Sappey’s line and 5-cm wide midline has further unpredictable lymphatic drainage and may drain to multiple lymph node basins. The triangular intermuscular space is an area that may harbour ectopic sentinel lymph nodes. It is located along the drainage of the upper back to the axillary basins, and it is bounded by the teres major inferiorly, the infraspinatus, teres minor, and subscapularis superiorly, and the long head of the triceps laterally.
MLBD occurs in approximately 20–30% of patients and, indeed, we detected 90 patients (29.5%) with more than one drainage basin. The significance of MLBD as a prognostic factor is still a matter of debate (7–13). In our series, we did not find a correlation between MLBD and SLN positivity or LN recurrence.
LN recurrences are reported to occur in both SLN-negative and SLN-positive patients at percentages between 3.2% and 4.4% and 7.4% and 19.6% of them, respectively (8, 15, 16, 18–23). We found similar results, with 5.2% and 14.5% of LN recurrences in SLN-negative and SLN-positive patients, respectively. Multivariate Cox-regression showed that a shorter time for LN recurrence was statistically associated with number of TINs and Breslow thickness (Table II). This confirms the data published in previous studies (7, 10, 13, 15, 16, 18–21).
Twelve LN recurrences in SLN-negative basins correspond to a false-negative rate (FNR) of 13.6%. Different biological reasons have been proposed to justify the high FNR after SLN identification: (i) block of the lymph flow by a massively metastatic SLN, thus redirect-ing the radiocolloid and/or the blue dye to a “new” SLN that might not yet contain metastases; (ii) tumour cells pass through the SLN and lodge in the next-echelon LN without producing metastases in the SLN (24); (iii) flaps/grafts and wide excisions alter the lymphatic drainage pattern of the primary melanoma (18); and (iv) variability and sluggishness of lymphatic systems in older people (23). Although some of these biological mechanisms could explain our 10 patients who presented LN recurrence in a SLN basin, the 2 recurrences in a NSLN basin could be simply illustrated because of technical errors. Indeed, there are numerous possible sources of professional inaccuracy that can alter the result of SLNB: (i) incorrect radiocolloid administration; (ii) too far or too deep with respect to the biopsy site/scar; (iii) relying only on planar imaging to localize the SLN(s) during the lymphoscintigraphic mapping; and (iv) inadequate histopathological analysis, such as only haematoxylin and eosin staining without immunohistochemistry and molecular biology techniques (24). However, a priori, it cannot be ruled out that biological mechanisms were at the base of these 2 NSLN basin recurrences.
On the other hand, 11 SLN-positive patients presented LN recurrences; 5 in a SLN basin and 6 in a NSLN basin. While it appears logical to explain the recurrences in a SLN basin as resulting from incomplete lymph node dissections and/or incomplete histopathological analysis, the mechanism underlying the recurrences in a NSLN basin is a matter of speculation. These recurrences can be caused by non-visualization of the additional basins during lymphoscintigraphy, but they also could be due to post-operative development of new lymphatic channels around the resected primary drainage basin. Indeed, all the patients with NSLN basin recurrence after a positive SLN were treated with CLND, and a positive SLN appeared to be the most important risk factor for NSLN basin recurrences. We used the CART analysis to describe the categories of patients who developed NSLN basin recurrence and their NSLN basin recurrence rates. The highest rate was reported in those patients with positive SLN and whose number of TINs was > 3; 4 patients were part of this category, and 2 (50%) developed NSLN basin recurrence. A lower rate was reported in patients with positive SLN and number of TINs between 1 and 3, which included 4 out of 72 (5.6%). Finally, just 0.9% of patients with negative SLN (2 out of 229) developed NSLN basin recurrence (Fig. 3). Multivariate analysis confirmed that recurrences in NSLN basins occurred earlier in patients with TINs > 3 than patients with 1–3 TINs or patients with negative SLN (Table II).
Three out of 8 NSLN basin recurrences appeared in patients with a dual basin drainage. However, as stated above, no statistical correlation was found, possibly due to the low number of cases. Interestingly, one of them was SLN negative. In this case, the patient presented 2 SLN basins, left and right axilla, but the LN recurrence appeared in the left inguinal basin. In this case with the exception of a technical error during the SLNB, we could hypothesize that the same SLNB procedure modified lymphatic flow. Using near-infrared imaging, Yokota et al. demonstrated that lymphatic flow is mainly preserved after SLNB although they collected only 11 cases of trunk melanoma. Indeed, 1 of the 3 patients with altered lymphatic flow after SNLB was affected by a melanoma of the right lumbar area (25).
Four patients with positive SLN were not treated with CLND because they refused the procedure. Nevertheless, none of them developed LN recurrence. Due to the low number of patients, it is impossible to draw some conclusion from this finding. However, it remains remarkable, considering the current recommendation to not perform CLND in SLN-positive patients based on the results of 2 recent practice-changing randomized clinical trials (21, 26). Consequently, our findings on NSLN basins recurrence should be validated in future series in which CLND is not offered routinely to patients with a positive SLN. As discussed before, harbouring a positive SLN was the most important risk factor for NSLN basins recurrence, and all the patients with positive SLN and NSLN basin recurrence were treated with CLND.
Study limitations and strengths
The main limitation of this study is data collection in a single institution, resulting in a low number of events; thus, the HR values might be overestimated. Thus, the results should require further confirmation in larger series.
The main strength of the study is that the data present-ed were prospectively collected by the same physicians at the same institution during a long follow-up period.
Conclusion
This study reported that 34.8% of LN recurrences of 305 primary trunk melanomas occurred in NSLN basins. This result suggests that, because of their anatomical characteristics, these melanomas should be checked regularly to exclude the appearance of LN metastases in basins not detected during SLNB. Consequently, it might be advisable to perform clinical examinations and ultrasound imaging on all potential lymphatic drainage basins (namely, both axillae and both groins) of patients affected by trunk melanoma. Ultrasonography is a non-invasive and accessible technique, and an excellent tool for early detection of LN recurrences. Indeed, close follow-up of SLN basin(s) with ultrasound is nowadays recom-mended instead of CLND for patients with positive SLN (21, 26). Nodal ultrasonography requires expertise from radiologists, and exploring all the 4 lymphatic drainage basins of a trunk melanoma may be time-consuming and not cost-effective. However, we consider that the clinically relevant possibility of finding an occult lymphatic metastasis should outweigh eventual health-economic consequences. Furthermore, with continuous advancement in the development of novel adjuvant treatments for melanoma, early detection of any metastatic disease could improve the prognosis of these patients.


 Click to show fullsize
Click to show fullsize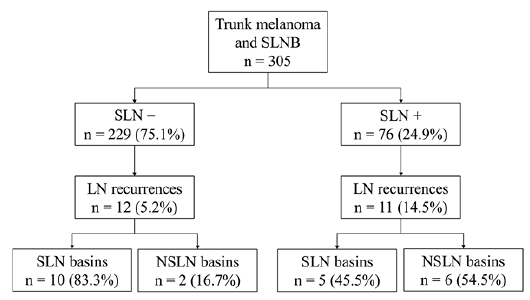 Click to show fullsize
Click to show fullsize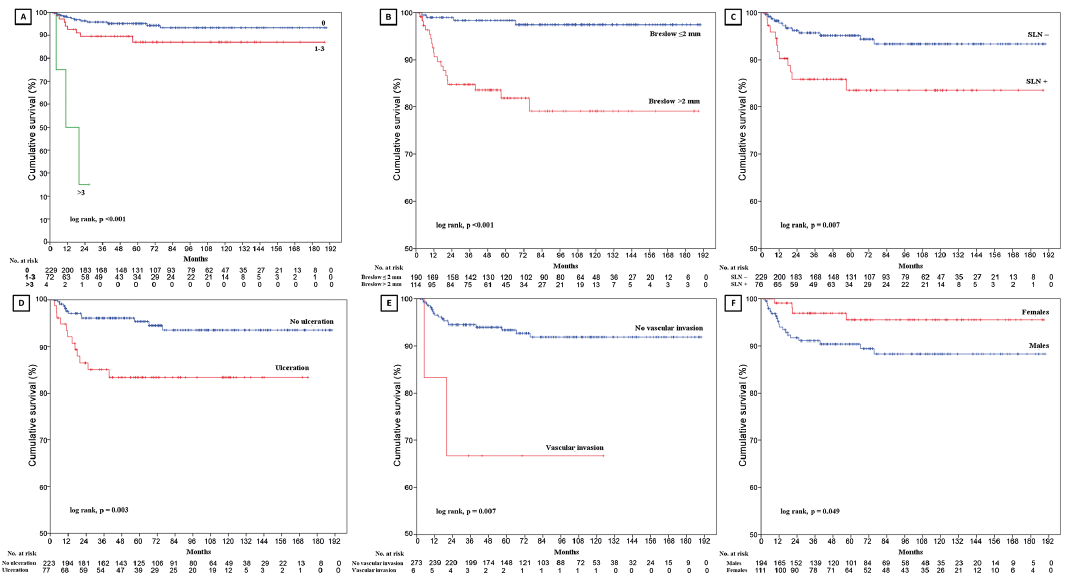 Click to show fullsize
Click to show fullsize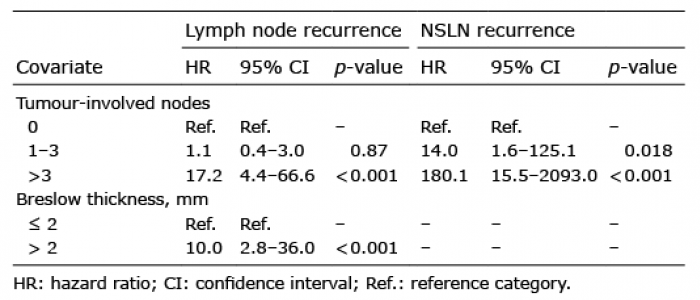 Click to show fullsize
Click to show fullsize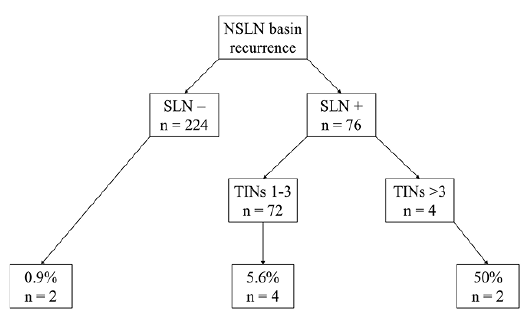 Click to show fullsize
Click to show fullsize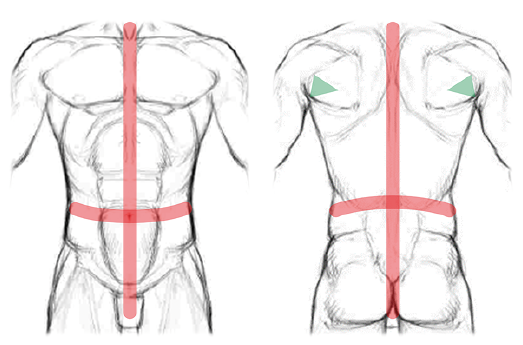 Click to show fullsize
Click to show fullsize