


Departments of Dermatology, 1Virgen de la Victoria University Hospital, Málaga, 2Virgen de las Nieves University Hospital, Granada, Spain, 3Ninewells Hospital, Dundee, UK, and 4School of Medicine, University of Granada, Granada, Spain
The aim of this study was to analyse the levels of anxiety, depression, and quality of life of individuals living with acne patients (cohabitants). The study included patients, cohabitants, and controls; a total of 204 participants. Patients’ health-related quality of life was measured with the Dermatology Life Quality Index (DLQI), while cohabitants’ quality of life was measured with the Family Dermatology Life Quality Index (FDLQI). The psychological state of all participants was measured with the Hospital Anxiety and Depression Scale (HADS). Presence of acne impaired the quality of life of 89.4% of the cohabitants. The FDLQI scores of cohabitants were significantly associated with the DLQI scores of the patients (rp = 0.294; p = 0.044). Anxiety and depression levels in cohabitants were significantly higher than in controls (p < 0.01). In conclusion, acne may have a negative impact on quality of life and psychological well-being of patients and their cohabitants.
Key words: quality of life; anxiety; depression; acne; family.
Accepted Sep 15, 2020; Epub ahead of print Sep 18, 2020
Acta Derm Venereol 2020; 100: adv00290.
doi: 10.2340/00015555-3636
Corr: Salvador Arias-Santiago, Department of Dermatology, Virgen de las Nieves University Hospital, ES-18014 Granada, Spain. E-mail: salvadorarias@ugr.es
Acne is a prevalent condition, which may impact on patients’ quality of life and psychological health. This study investigated whether acne also affects the well-being of persons living with these patients. The results showed that the quality of life and depression level of patients are closely associated with those of their cohabitants. Most cohabitants (87.1%) declared some impairment in their quality of life. Therefore, in the management of patients with acne, dermatologists should take into consideration not only the clinical severity of the skin condition, but the impact of this disease on the well-being of the patients and their cohabitants.
Acne vulgaris is a prevalent condition (85% of adolescents and 6–10% of the general population are affected (1)) that typically affects important cosmetic areas (such as the face, neck and chest), with a risk of permanent scarring. The high aesthetic impact of this condition, along with the pain often associated with inflammatory acne lesions, can make living with acne unbearable for many patients (2). People who have acne are more prone to have social phobia and develop social avoidance behaviours (3), and have a higher risk of developing anxiety and depression disorders (4, 5).
Particular attention should be given to the fact that most people with acne have the condition during adolescence; a sensitive developmental period during which biological, psychological and social changes facilitate the individual to become fully independent from the family (6, 7). A chronic illness during this period can have negative long-term consequences, including compromised educational attainment and failure to sustain close personal relationships (8, 9).
The impact of acne on patients’ quality of life (QoL) is frequently underestimated; however, studies have shown that acne may impact on patients’ mental health and social functioning, similar to other diseases, such asthma, epilepsy or diabetes (10).
Some researchers are beginning to explore how living with an affected individual might affect the cohabitant’s QoL. Studies have recently shown that some diseases (i.e. advanced cancer (11), obsessive-compulsive disorder (12) or amyotrophic lateral sclerosis (13)) can have a major impact on the cohabitants of patients. In dermatology, new studies have highlighted the potential burden of living with patients with atopic dermatitis (14) or psoriasis (15). However, no study has yet addressed how living with acne patients might affect cohabitants’ QoL. Considering the heavy burden of acne on patients, attention should be paid to whether part of this burden might be transferring from patients to their family unit.
The objective of this study is to analyse the QoL and the levels of anxiety and depression of individuals living with acne patients (cohabitants).
Subject selection
Three groups were analysed: patients consecutively selected from the dermatology outpatient clinic at Virgen de las Nieves University Hospital (Granada, Spain); their cohabitants; and healthy controls. Patients with acne were eligible for the study if they met the following criteria: age ≥ 16 years and score ≥ 3 according to the Leeds Revised Acne Grading system (LRAG) (16). Study exclusion criteria for all participants were: age < 16 years; the presence of a severe disease (e.g. inflammatory or metabolic disease, cancer, etc.); another dermatological disease, or a psychiatric diagnosis.
The following clinical data were gathered for each patient: LRAG score (a validated scale that asses the severity of acne on 3 locations (face, chest and back) and gives a score ranging from 0 to 28) (16), previous treatments, and years since onset of acne.
The impact of acne on the QoL of patients was determined using the Dermatology Life Quality Index (DLQI) (17). This widely used questionnaire is a validated dermatology-specific instrument that measures health-related QoL in skin patients. It contains 10 items assessing the patient’s skin status and problems associated with skin disease. A series of validated band descriptors have been validated to give meaning to the total scores of the DLQI (18): 0–1: no effect on patient’s life, 2–5: small effect, 6–10: moderate effect, 11–20: very large effect, and 21–30: extremely large effect.
The impact of acne on the QoL of cohabitants was measured with the Family Dermatology Life Quality Index (FDLQI) (19). The FDLQI is a validated dermatology-specific QoL instrument for the family members/partners of patients having any skin disease. Each question asks about the family member’s perception of a specific impact on his/her QoL. The scores of individual items are added to generate a total score with a range of 0–30; higher total FDLQI scores indicate greater impairment of the cohabitant’s QoL.
The Hospital Anxiety and Depression Scale (HADS) was chosen to evaluate the state of anxiety/depression, because it is widely accepted, validated for use in general populations, and easy to apply (20). The HADS is divided into an anxiety subscale (HADS-A) and a depression subscale (HADS-D), both containing 7 items. Each subscale is scored from 0 to 21, with higher scores pointing towards a higher psychological discomfort. Scores of 8 or higher in each subscale suggest significant distress and possible clinical anxiety ± depression or another mental illness, and so further assessment is desirable (21).
Finally, a questionnaire was completed by all patients to gather data on their sex, age, years since acne onset, marital status, education level, and occupation. The DLQI/FDLQI, HADS, and demographic questionnaires were given to patients/cohabitants at a follow-up visit and could be completed in the office or at home (in 1–3 days), as preferred. The relationship of the cohabitants with the patients (i.e. parent, sibling, partner, son/daughter, grandson/daughter, or other) was recorded.
For comparative purposes, the HADS and demographic questionnaires were also completed by a control group of 47 relatives (not necessarily cohabitants) of physicians in training at Virgen de las Nieves Hospital (Granada).
Ethical aspects. All patients gave their informed consent, and the anonymity of the cohabitants was strictly preserved.
Statistical analysis
The Student’s t-test was applied to compare mean values of quantitative variables and, when not normal, the Mann-Whitney U test was used. For ≥ 2 groups, an analysis of variance test was performed. Qualitative variables were analysed with the χ2 or Fisher exact tests if at least 1 cell had an expected count < 5. Associations between continuous variables were analysed using the Pearson coefficient of rank correlation (rp). A multivariate analysis was carried out using multiple linear regression to determine the independent associated factors of FDLQI. p < 0.05 was considered statistically significant in all tests. SPSS software (version 20.0.0; IBM Corp, Somers, NY) was used for statistical analyses.
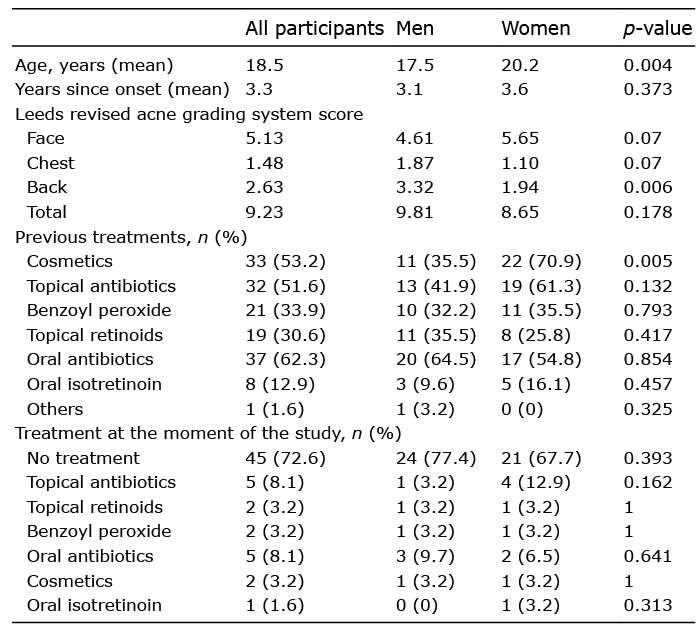
The study included 204 individuals: 62 patients with acne, 66 patient cohabitants, and 76 healthy controls. The patient group included 31 men and 31 women, with a mean age of 18.52 years (range 16–36 years). Their mean LRAG score was 9.23 (range 4–19), with a mean time since onset of 3.3 years (range 0.5–11 years) (Table I). Most patients had tried topical treatments (40 (64.5%)) and/or systemic antibiotics (38 (61.29%)), while a minority had previously been treated with oral isotretinoin (8 (12.9%)).
Table I. Clinical features of patients
Demographic characteristics
There were no significant differences among the cohabitants and the healthy controls group with regard to sex (18:48 vs 22:54; p = 0.825), occupation (44.2% vs 48.7% of active workers; p = 0.723), marital status (74.2% vs 68.5%; p = 0.445), or the proportion of group members with higher professional or university education (29.4 % vs 53.9%; p = 0.083) (Table II).
Table II. Demographic and study variables (Dermatology Life Quality Index, Family Dermatology Life Quality Index, anxiety, and depression) in the 3 groups
Dermatology Life Quality Index and Family Dermatology Life Quality Index
The mean DLQI score of the patient group (7.56; range 0–29) was higher than the mean FDLQI score of the cohabitant group (6.46; range 0–26) (Table II). DLQI scores showed a severe impact on QoL (DLQI>10) in 24.2% of patients. For the cohabitants, 19.7% had a total FDLQI score>10. The FDLQI score of cohabitants revealed a statistical association with the DLQI score of patients (rp = 0.294; p = 0.044) (Fig. 1a).
Fig. 1. Correlation analysis. (a) Family Dermatology Quality Index (FDLQI)/Dermatology Life Quality Index (DLQI) (rp = 0.294, p = 0.044). (b) Cohabitants- depression/Patients- depression (rp = 0.384, p = 0.001).
The multivariate linear regression showed a statistically significant association between the FDLQI of cohabitants and the DLQI of patients, regardless of age, sex, family relationship with the patient, anxiety and depression levels (of the patients and cohabitants), educational level LRAG score (of the patient) (standardized β = 0.231 (p = 0.048); R2 of adjusted model = 0.461 (p < 0.001)) (Table III).
Table III. Multiple linear regression analysis of independent predictors associated with Family Dermatology Life Quality Index (FDLQI) score
Hospital Anxiety and Depression Scale results
Anxiety. The mean HADS anxiety score (HADS-A) was 6.29 (range 0–15) for patients, 6.91 (range 1–19) for cohabitants, and 5.24 (range 0–17) for controls. The ratio of individuals in each group with HADS-A ≥ 8 (indicative of anxiety disorder) was 32.25% for patients, 43.3% for cohabitants, and 17.1% for controls (Table II). The different prevalence of anxiety (HADS-A ≥8) between cohabitants and controls was statistically significant (p = 0.003). The analysis did not find a statistically significant correlation between the anxiety of patients and their cohabitants.
The HADS anxiety score for patients revealed a strong statistical association with the DLQI score (rp = 0.549, p < 0.001). Among cohabitants, the anxiety level was also related to the FDLQI score (rp = 0.635, p < 0.001), and the presence of anxiety (HADS-A ≥8) was associated with a poorer QoL (FDLQI = 9.93 vs 5.20; p < 0.001) (Fig. 2a).
Patients who had previously been treated with oral isotretinoin showed a higher mean anxiety level (5.96 vs 2.39, p = 0.06), although the severity of their acne (measured by the LRAG score) was not higher compared with the rest of patients (8 vs 9.25; p = 0.717).
Depression. The mean HADS depression score was 2.47 (range 0–11) for patients, 4.23 (range 0–16) for cohabitants, and 2.75 (range 0–15) for controls (Table II). The ratio of individuals in each group with HADS-D ≥ 8 (indicative of depression disorder) was 9.7% for patients, 16.7% for cohabitants and 5.3% for controls (Table II). The different prevalence of depression (HADS-D ≥ 8) between cohabitants and controls was statistically significant (p = 0.027).
The depression level of patients was statistically associated with the depression level of their cohabitants (rp = 0.384; p = 0.001) (Fig. 1b). The patient group had a strong association between depression and DLQI score (rp = 0.615; p < 0.001). The cohabitant group also showed a statistical association between their depression and FDLQI score (rp = 0.505; p < 0.001). Furthermore, depression among cohabitants (HADS-D ≥8) was associated with higher FDLQI scores (FDLQI=9.93 vs 5.20; p = 0.001) (Fig. 2b).
Fig. 2. Mean Family Dermatology Quality Index (FDLQI) score in cohabitants with anxiety or depression. (a) Anxiety (Hospital Anxiety and Depression Scale (HADS)-A ≥8) and (b) depression (HADS-A ≥8) were associated with a higher FDLQI score in cohabitants (p < 0.001).
Studies have begun to emerge on the impact of dermatological diseases on the QoL of relatives, most frequently in relation to atopic dermatitis (22) and psoriasis (23). However, there has been no research on the effect of acne on the QoL of patients’ relatives. The results of the current study show that only a small percentage (10.6%) of people living with patients with acne reported no impairment in their QoL, while most cohabitants (51.5%) reported a high impact on their QoL (FDLQI>10) (17). These results corroborate the hypothesis of the negative impact of acne on the QoL of patients and their cohabitants.
In the current study patients older than 20 years showed a higher impact on their QoL. Various factors might contribute to these results. Feelings such as embarrassment, frustration, demoralization and discontent might be more pronounced in older patients because they continue to have to cope with a condition that is not found in most people of their age. Feelings of stigmatization can be present. Furthermore, as has been hypothesized for psoriasis (24), acne could have a cumulative deleterious impact on patients’ QoL. Living with acne for years could prevent patients from achieving their personal, social and professional goals, affecting their lives at a more profound level compared with patients who have acne for a shorter period of time.
Men and women showed similar LRAG scores and similar time of evolution. However, DLQI scores were higher in women with acne, trending to statistical significance, as has been reported previously (25). The reasons why acne could be less tolerable for women are not completely understood. It should be considered that approximately 70% of women with acne experience premenstrual flares (26), this could lead to an underestimate of the severity of acne if the patient attends clinic during another phase of her menstrual cycle (27). Another explanation for the higher impact of acne on women might be related to the unrealistic beauty expectations (particularly for women) established in modern society.
This study found that cohabitants had a statistically significantly higher anxiety level than healthy controls. Previous studies have found high anxiety levels in individuals with acne (28), but the current study is the first to analyse cohabitants’ anxiety. Further studies are necessary to determine how different factors associated with acne (clinical severity, affected area, time since onset, treatment, etc.) might influence cohabitants’ psychological health.
Patients who had previously been treated with oral isotretinoin had a significantly higher level of anxiety compared with the rest of patients, even though the clinical severity of their acne was similar at the time of the study. The effect of isotretinoin on mental health has been controversial. Until recently, some studies pointed that oral isotretinoin might increase the risk of anxiety and depression in some patients (29). In 2005 the US Food and Drug Administration (FDA) issued a warning in which close observation for symptoms of depression or suicidal thought was recommended for patients taking oral isotretinoin (30). However, recent studies have provided evidence that anxiety and depression in acne patients is more likely to be induced by the skin condition itself, while oral isotretinoin (being the most effective treatment for severe forms of acne) would instead improve psychological distress (31, 32). We consider that our results are unlikely to be caused by oral isotretinoin, but rather to the discontent associated with a skin condition that persists despite treatment.
We found that the mean depression level of our patients was low. It is recognized that it can be difficult to establish the prevalence of clinical depression in teenagers. Available data suggest that depression is less prevalent among adolescents and young adults (33). However, other authors suggest that depressive disorder may be under-diagnosed in adolescents, as available screening questionnaires may be not sensitive enough to detect depression in this younger population (34). In our study cohabitants showed significantly higher depression levels compared with the control group. One plausible explanation could be that the empathic relationship between patients and cohabitants could induce depressive symptoms in the cohabitants who witness distress and impact on daily life associated with acne on the affected individuals. Furthermore, it is noteworthy that the depression level of the cohabitants was significantly associated with the depression level of the patients.
An interesting finding of the current study is the significant association between QoL (of patients and cohabitants) and their anxiety and depression levels. This ratifies the internal consistency of the study, since it was expected that a worse QoL would be associated with higher psychological discomfort.
Our findings show the importance of treating acne patients from a holistic standpoint rather than being limited to their physical signs and symptoms. It should be taken into account that acne, although it is generally not a threat to the patient’s general health, has a great impact on the body image and self-esteem at a sensitive age, when patients are young, developing their personalities, and taking decisions that will have a great impact on their future. The high cosmetic impact of acne, the pain associated with inflammatory lesions, or the side-effects of treatments, represent a burden for patients that may be transferred to the rest of the family members. The complex psycho-social dimensions of acne are best explored during clinic in order to assess QoL impact and quantify distress of acne patients and their cohabitants. For patients with mild psychological distress, reassurance, empathy and emotional support and optimum acne treatment is usually enough, while severe cases with high distress may require the specialized care of a psychologist or psychiatrist.
Study limitations
Study limitations include sample size; additional studies with larger numbers of patients and cohabitants would be required to analyse differences between subgroups of patients and cohabitants. The questionnaires used have been validated for patients ≥ 16 years old; therefore new specifically designed studies will be necessary to analyse how acne affects younger patients and cohabitants. In addition, because the controls were relatives of junior physicians, their mean health level might have been higher than that of the general population.
Conclusion
In summary, we found that the DLQI and depression levels in patients with acne are associated with the FDLQI and depressions levels in their cohabitants. In addition, cohabitants showed higher anxiety and depression levels than healthy controls. Dermatologists should consider the QoL and psychological health of their patients, who will sometimes require multidisciplinary management alongside psychologists and psychiatrists. We also recommend that the cohabitants of patients are offered information on acne and its potential negative impact on QoL and associated psychological distress. Support and guidance for the affected individual and their cohabitants is desirable to facilitate both parties to use existing resilience strategies, with advice to seek further help if needed.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize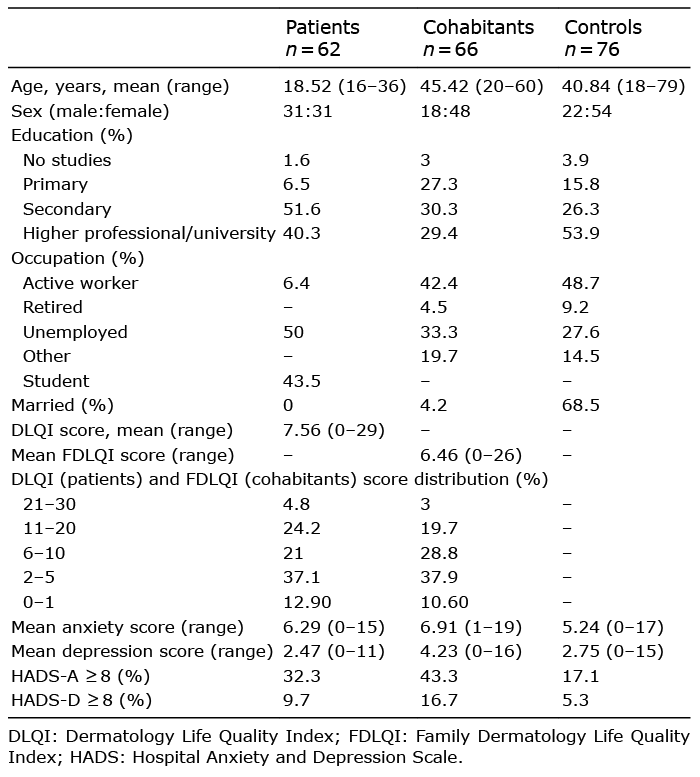 Click to show fullsize
Click to show fullsize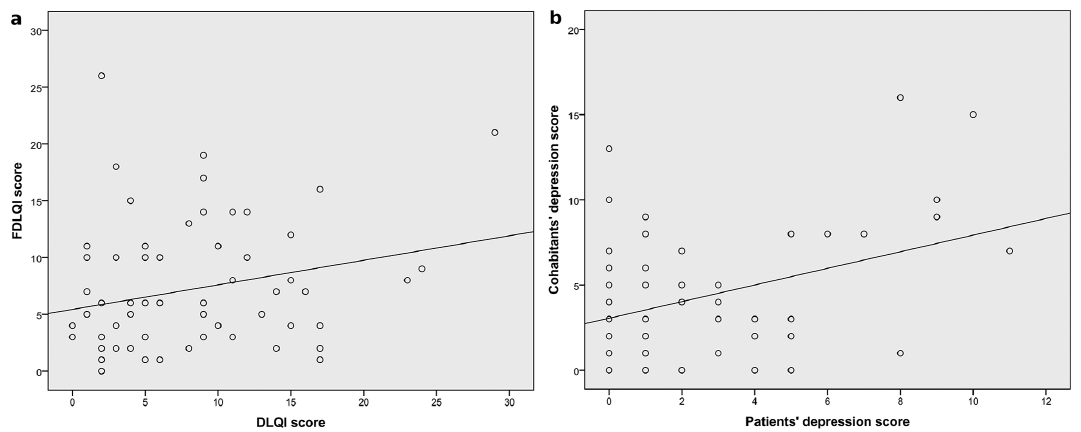 Click to show fullsize
Click to show fullsize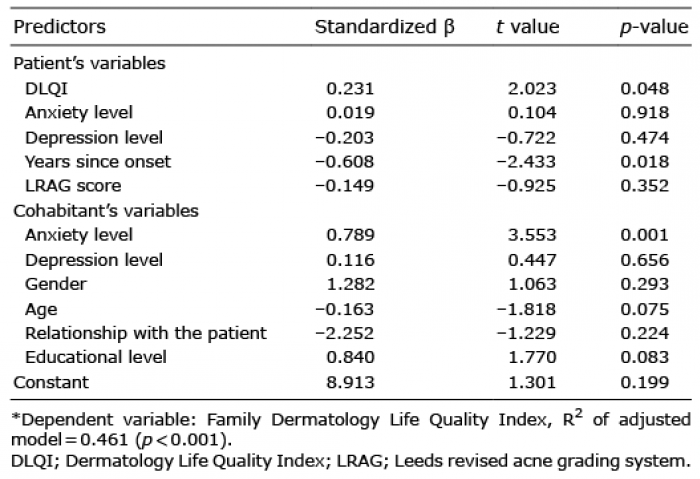 Click to show fullsize
Click to show fullsize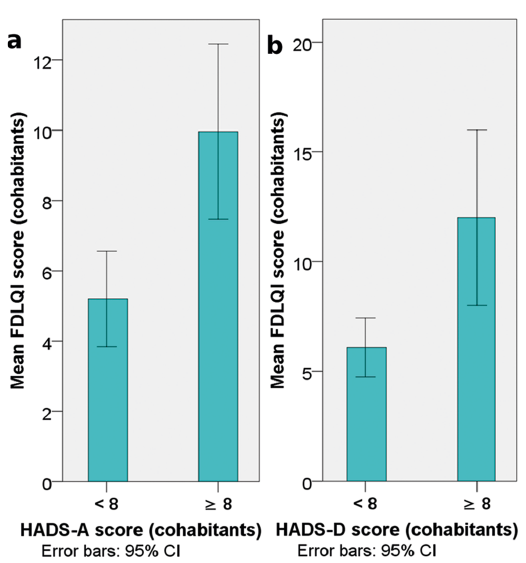 Click to show fullsize
Click to show fullsize