


1Division of Dermatology, Department of Medicine of Sensory and Motor Organs, Faculty of Medicine, 3Laboratory of Electron Microscopy, Tottori University, 2Division of Clinical Genetics, Tottori University Hospital, Yonago, and 4Department of Dermatology, Hirosaki University Graduate School of Medicine, Hirosaki, Japan. E-mail: taninaomi@tottori-u.ac.jp
Accepted Sep 18, 2020; Epub ahead of print Sep 23, 2020
Acta Derm Venereol 2020; 100: adv00285.
doi: 10.2340/00015555-3643
Bathing suit ichthyosis is a minor variant of autosomal recessive congenital ichthyosis (ARCI) (1). This phenotype shows a unique distribution of lesions with brownish scaling, involving the scalp, neck and trunk, but sparing the central face and extremities (2). Oji et al. (3) reported that there was a marked decrease in enzyme activity on in situ transglutaminase (TGase) testing in the skin of patients with bathing suit ichthyosis when the temperature was increased from 25°C to 37°C. They suggested that bathing suit ichthyosis was caused by the temperature sensitivity of specific transglutaminase-1 gene (TGM1) mutations (3). We report here a case of bathing suit ichthy-osis with a novel TGM1 mutation. In addition, this is the second Japanese case reported as “bathing suit ichthyosis’’.
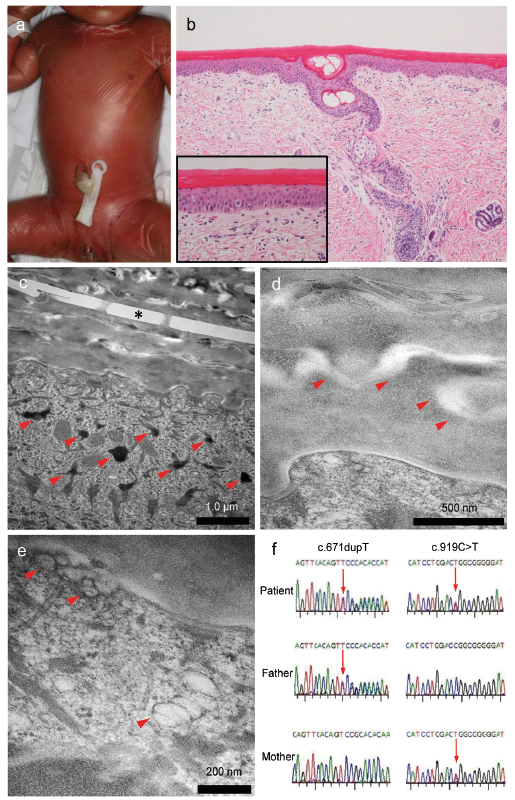
A 0-day-old, first-born girl presented a collodion membrane on her skin surface immediately after delivery and was referred to the outpatient dermatology clinic, Tottori University Hospital, Tottori, Japan. There was no family history of ichthyosis or any other relevant history. Her parents were not consanguineous. Physical examination showed that the patient’s entire body was cov-ered with a semi-transparent shiny cellophane-like membrane and the inguinal skin had notable fissures (Fig. 1a). She had ectropion of the bilateral eyelids. Other congenital malformations were not detected. Histopathology of a biopsied specimen taken from the abdomen at 7 days of age showed compact ortho-hyperkeratosis and a normal granular layer at the light microscopic level. The dermis showed minimum superficial perivascular infiltration of inflammatory cells (Fig. 1b). Transmission electron microscopy (TEM) revealed bamboo-shaped crystalloid structures, so-called cholesterol clefts, inside some of the corneocytes (Fig. 1c). A hypoplastic marginal band of corneocytes was seen (Fig. 1d). In keratinocytes of the granular layer, keratohyalin granules were decreased in number and were small (Fig. 1c), and vacuolated lamellar granules were seen occasionally (Fig. 1e). After obtaining informed consent, direct sequencing analysis of the TGM1 gene was conducted. Compound heterozygous mutations were detected in the TGM1 gene (c.671dupT [p.R225Pfs*14] and c.919C>T [p.R307W]). These variants were inherited from the patient’s father and mother, respectively (Fig. 1f). After birth, humidifying, via a closed-type infant incubator and topical application of a moistu-rizing agent, were started. The collodion membrane gradually peeled off and ectropion was improved in a few weeks. However, multiple brown scales remained over the forehead, trunk and extremities at 3 months of age (Fig. 2a). At the age of 7 months, her face except for the forehead, extensor side of the upper extremities and both lower extremities showed a normal appearance. Brown-ish scaling remained on her forehead, trunk, flexor side of the upper extremities, popliteal region, feet and hands. Fig. 2b shows brownish scales mainly on the trunk indicating a “bathing suit appearance” at 8 months of age (Fig. 2b). Based on the clinical course and results of ultrastructural and genetic examinations, a diagnosis of bathing suit ichthyosis was made.
To evaluate the association between body temperature and distribution of skin symptoms, thermography was performed at the age of 8 months (Fig. 2c). The areas of higher temperature in thermography images corresponded to the distribution of ichthy-osiform skin lesions.
Fig. 1. (a) Clinical findings at initial visit at 0 days of age. The patient’s entire body was covered with a semi-transparent shiny cellophane-like membrane and the inguinal skin showed notable fissures. (b) Histopathology of a biopsied specimen taken from the abdomen at 7 days of age. Histopathology showed compact hyperkeratosis, a normal granular layer and minimum inflammatory infiltration in the superficial dermis (haematoxylin-eosin stain, original magnification ×100). (c–e) Transmission electron microscopy (SU6600 field emission scanning electron microscope (Hitachi, Tokyo, Japan)). (c) Crystalloid structures, so-called cholesterol clefts (*), inside some of the corneocytes. Keratohyalin granules that were small in number and in size (arrows). (d) Hypoplasia of a marginal band of corneocytes (arrows). (e) Vacuolated lamellar granules (arrows). (f) The compound heterozygous TGM1 mutations p. R307W (c. 919C>T) and p. R225Pfs*14 (c. 671dupT) were detected in the patient. P. R225Pfs*14 was present in the father and p. R307W was shown to be maternal.
Fig. 2. (a) Clinical findings at 3 months of age. Multiple brown scales remained over the patient’s forehead, trunk and extremities. (b) Clinical findings at 8 months of age. Brownish scaling remained on her forehead, trunk, flexor of the upper extremities, popliteal region, feet and hands. Other regions of her face and outside of the superior limb and both lower extremities showed a normal appearance. (c) Thermography image which were taken using a INF-3000 thermograph (Nihon Kohden, Tokyo, Japan) at 8 months of age. The areas of higher temperature in the thermography image correspond to the distribution of ichthyosiform skin lesions.
Bathing suit ichthyosis is a rare variant of ARCI due to the temperature sensitivity of certain TGM1 mutations. Affected individuals are born as collodion babies. After shedding the membrane during the first weeks of life, the patient develops a characteristic distribution of brownish scaling involving the “bathing suit” areas. In the current case, the patient was born with a collodion membrane that exfoliated in a few weeks, and developed multiple brown scales on the whole body. The restriction of brown scales to the “bathing suit” areas became apparent at the age of 7 months.
The correlation between the ichthyosiform skin lesions in this case and areas of higher temperature in thermogra-phy images were in agreement with the results of a previous study (3). This suggests that a high body surface temperature might contribute to the formation of ichthyosiform skin lesions in bathing suit ichthyosis.
In a previous study, more than 20 missense mutations of TGM1 were reported in patients with bathing suit ichthyosis (4). Some missense mutations were reported only in patients with this disease, and other mutations were reported in both patients with bathing suit ichthyosis and patients with generalized ARCI. The same TGM1 mutation could result in bathing suit ichthyosis or ARCI.
This case had the compound heterozygous TGM1 mutations p. R307W (c. 919C>T) and p. R225Pfs*14 (c. 671dupT). The TGM1 mutation p. R307W has been reported in Japanese patients with lamellar ichthyosis and with bathing suit ichthyosis (5, 6), while R225Pfs*14 is a novel mutation. Clear genotype-phenotype correlations have not been established. Both mutations in present patient were arginine substitutions. Interestingly, a previous report delineated that mutation related to arginine substitutions may be common in this disorder (4, 7). The reason for the high frequency of arginine substitution mutations in this disorder is unknown, but it would be related to the pathophysiology.
The TGM1 gene encodes TGase-1, an enzyme involved in the formation of a cornified envelope. The lipid synthesized in keratinocytes is stored in lamellar granules and is released between the stratum corneum and granular layers as lipid lamellae stacks. In TGase 1-/- mouse skin, formation of these stacks was incomplete in the extracellular spaces of the stratum corneum and retention of lamellar granules was evident (8). TEM of bathing suit ichthyosis has shown the presence of cholesterol crystals (3, 9) and a hypoplastic cornified envelope and delay of the degradation of corneodesmosomes (6) in the horny layer. TEM of lamellar ichthyosis has demonstrated cholesterol crystals in the horny layer, absence or thinning of the cornified envelope, and small keratohyalin granules and lipid droplets in corneocytes (10). Our TEM findings showed, for the first time, vacuolated lamellar granules besides previously known ultrastructural findings of bathing suit ichthyosis and/or lamellar ichthyosis.


 Click to show fullsize
Click to show fullsize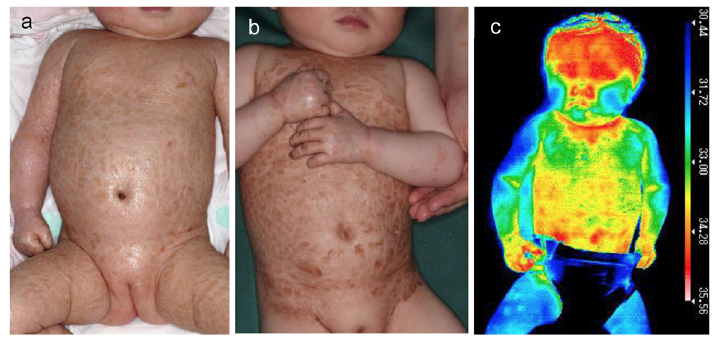 Click to show fullsize
Click to show fullsize