


1Department of Dermatology and Venerology, Peking University First Hospital, 2Beijing Key Laboratory of Molecular Diagnosis on Dermatoses, 3National Clinical Research Center for Skin and Immune Diseases, Beijing 100034, and 4Department of Dermatology, Traditional Chinese Medical Hospital of Xinjiang Uygur Autonomous Region, Xinjiang, China. *E-mail: yangwang_dr@bjmu.edu.cn
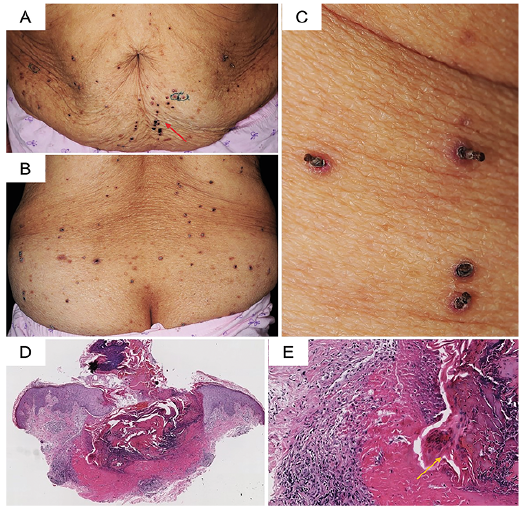
An 80-year-old woman presented with a 1-month history of generalized pruritic skin rash (Fig. 1). She also reported an aggravating bone pain in the lower back and weakness during the past 2 months. She did not report any constitution-al symptoms (weight loss, fever). Her medical and family histories were unremarkable. Physical examination revealed multiple, widespread brown-erythematous papules with a central keratotic core on the trunk and extremities (Fig. 1A–C). Koebner’s phenomenon was seen, resulting in a linear distribution of new lesions after scratching. Labora-tory tests revealed moderate anaemia (haemoglobin level 69 g/l; normal range 110–150 g/l), and an elevated serum IgG level (41.70 g/l; normal range 7.23–16.85 g/l). The renal function and serum calcium levels were within normal limits. A skin biopsy was performed on a papule (Fig. 1D, E).
What is your diagnosis? See next page for answer.
Fig. 1. (A) Abdomen. Numerous brown-erythematous papules with a central keratotic core on the abdomen. Koebner’s phenomenon can be seen (red arrow). (B) Lower back. Numerous brown-erythematous papules with a central keratotic core on the lower back. (C) Close-up. The brown-erythematous papules with a central keratotic plug. (D) Skin biopsy specimen shows a central cup-shaped invagination of the epidermis comprised of parakeratotic cells, debris, and other basophilic and eosinophilic substance (haematoxylin-eosin; H&E), original magnification ×40). (E) Higher magnification image of the cup-shaped invagination (H&E, original magnification ×400), filled with markedly degenerated collagen bundles vertically eliminated through the epidermis (yellow arrow).
Acta Derm Venereol 2020; 100: adv00278.
Diagnosis: Acquired reactive perforating collagenosis
Histopathological analysis revealed a cup-shaped invagination of the epidermis with transepidermal elimination of necrotic collagen bundles (Fig. 1D, E), which was consistent with reactive perforating collagenosis.
Acquired reactive perforating collagenosis (ARPC) is frequently associated with diabetes mellitus and chronic kidney disease (1) and, in rare conditions, association with haematological malignancies has been reported (2). In the current case, neither diabetes mellitus nor kidney dysfunction was present. Instead, lower back pain and weakness were notable in this patient. Combined with the anaemia and elevated serum IgG level, a hematopoietic malignancy was suggested. Further immunofixation electrophoresis of serum and urine revealed monoclonal IgG kappa light-chain. Bone marrow aspiration showed infiltration of plasmablasts (68% of bone marrow cells) with high nuclear/cytoplasmic ratio, binucleated and multinucleated forms, 1–2 prominent nucleoli, and basophilic cytoplasm (Fig. 2), fulfilling the diagnostic criteria of active multiple myeloma (3). Therefore, a diagnosis of acquired reactive perforating collagenosis associated with multiple myeloma was made. The patient refused treatment and died from progressive myeloma 3 months after the diagnosis.
Clinically, reactive perforating collagenosis can be divided into 2 forms: the inherited form and the acquired form (1, 4). ARPC is an uncommon skin disease characterized by pruritic, umbilicated hyperkeratotic papulonodules involving trunk and extremities, and the keratotic materials are vertically oriented perforating bundles of necrotic collagen (1, 4, 5). Koebner’s phenomenon may also occur (1). There is a close relationship between ARPC and underlying systemic diseases. Among all coexisting diseases, diabetes mellitus and complications are the most frequent condition, followed by chronic kidney disease (1). Occasionally, ARPC may be associated with malignant disorders, including solid tumour and haematological neoplasm, and represent a paraneoplastic process (6). In an analysis of 11 cases of ARPC with malignancies, 4 (36%) cases had lymphoproliferative diseases, including Hodgkin’s disease in 3 cases and myelodysplastic syndrome in one case (3). To the best of our knowledge, no previous association with multiple myeloma was reported.
The precise pathogenesis of ARPC remains unknown (7). On a pathophysiology level, ARPC is characterized by hyaline degeneration of collagen fibres (8). ARPC may involve a complex interaction between the epithelium, connective tissue, and inflammatory mediators. Superficial trauma to the epidermis may be the primary inciting factor in susceptible patients. Predisposing conditions include vasculopathy, microdeposition of exogenous materials within the dermis (including calcium salts and silicon), and epidermal or dermal change related to metabolic derangements (1, 8).
The management of ARPC involves 2 aspects: controlling pruritus and treatment of underlying extracutaneous disorders. Skin-directed therapies, including topical cortico-steroids, emollients, anti-histamines and narrowband ultraviolet B, were used for relieving the symptoms (1). Treatments on associated comorbid diseases are pivotal for the regression of skin lesions of ARPC. Kawahara et al. (2) reported 2 ARPC cases associated with haematological malignancy, which showed remarkable improvement of skin lesions after chemotherapy.
The current patient presented neither diabetes mellitus nor kidney dysfunction. Instead, lower back pain and weakness were remarkable in the course of her disease. The laboratory tests were suggestive of active multiple myeloma. Therefore, ARPC is a paraneoplastic process and a late phenomenon in the course of active myeloma in the current patient. Although extremely rare, when patients of ARPC present with cachexia, such as weight loss, weakness, or unexplained fever and bone pain, the association with internal malignancy should be considered.
In conclusion, this case highlights the importance of the recognition of the paraneoplastic skin conditions, which may lead to timely treatment of the associated aggressive malignancies.
Fig. 2. Bone marrow smear. Morphological findings in the bone marrow showed plasmablasts infiltration (Wright-Giemsa stain, original magnification ×640).


 Click to show fullsize
Click to show fullsize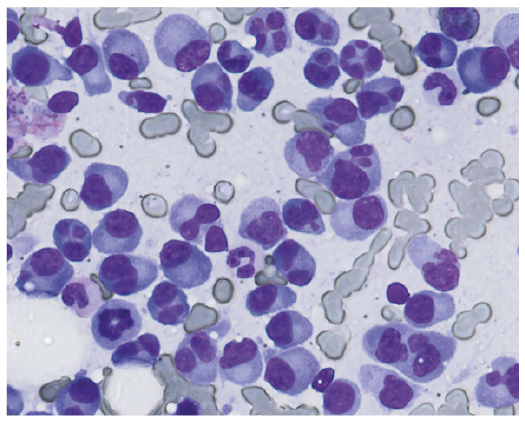 Click to show fullsize
Click to show fullsize