


IDI-IRCCS (Istituto Dermopatico dell’Immacolata-Istituto di Ricovero e Cura a Carattere Scientifico, Dermatological Research Hospital), Rome, Italy
Depression is frequent in patients with hidradenitis suppurativa. However, its relationship with quality of life and clinical severity needs further investigation. In this cross-sectional study, 341 adult, consecutive patients with hidradenitis suppurativa completed the 12-item General Health Questionnaire (GHQ-12), which has been shown to be able to identify cases of major depressive disorder in dermatological patients. The frequency of depression in hidradenitis suppurativa patients was 29.0%. In patients with depression, severity (International Hidradenitis Suppurativa Severity Score System (IHS4)), quality of life (Skindex-17; Dermatology Life Quality Index (DLQI)), and health status (36-item Short Form Health Survey (SF-36)) were significantly worse compared with patients with no depression. The highest linear correlation was observed between GHQ-12 and the psychosocial scale of the Skindex-17 and the SF-36 mental scale. In contrast, correlation between GHQ-12 and clinical severity was poor. Depression is an important comorbidity in hidradenitis suppurativa, which is strongly associated with impairment in quality of life, but not linearly correlated with clinical severity.
Key words: acne inversa; clinical severity; depression; 12-item General Health Questionnaire; hidradenitis suppurativa; quality of life.
Accepted Sep 24, 2020; Epub ahead of print Sep 28, 2020
Acta Derm Venereol 2020; 100: adv00319.
doi: 10.2340/00015555-3647
Corr: Francesca Sampogna, Clinical Epidemiology Unit, IDI-IRCCS, Via dei Monti di Creta, 104 IT-00167 Rome, Italy. E-mail: fg.sampogna@gmail.com
In this study of 341 patients with hidradenitis suppurativa, a prevalence of depression of 29% was observed. While there was a linear correlation between depression and quality of life or health status measures, this correlation was not observed with clinical severity. This confirms that clinical severity measures, which are based mainly on clinical signs, do not necessarily correspond to the burden that the disease has on the patient. In fact, hidradenitis suppurativa is a condition with a strong psychosocial impact even at a low level of clinical severity.
Hidradenitis suppurativa (HS) is a chronic and debilitating skin disease. Painful nodules and abscesses, purulent discharge, scarring and, often, draining tunnel formation, predominantly affecting intertriginous sites (1), have heavy psychosocial consequences on patients (2). The impact on patients’ quality of life (QoL) is considerable (3), and higher than that observed in many other chronic dermatological conditions (4), and even in non-dermatological conditions (5). Specific psychosocial aspects have been investigated, such as stigmatization, fatigue and satisfaction (6), pain (7), sexual disturbance (8), resilience (9) and alexithymia (10). However, the psychological conditions mainly investigated in patients with HS are depression and anxiety, which are known to be common in patients with chronic dermatological conditions. A recent systematic review and meta-analysis (11) concluded that depression and anxiety are frequent in patients with HS. A higher prevalence of depression was found in patients with HS compared with controls (12). However, there were large discrepancies in the estimation of the prevalence of depression, from 1.6% (13) up to 37.8% (14), depending on the methodology and the instrument used. Analysing the same population, Onderdijk et al. (15) found that using a self-report measure the prevalence of depression was higher in patients with HS compared with controls, while clinically defined depression rates according to International Classification of Diseases, 10th revision (ICD-10) criteria were not significantly higher in patients with HS than in controls.
Psychological distress in patients with HS has been found to be associated with shame (16) and physical pain (16, 17). The observations concerning the association between depression and clinical severity in HS are not homogeneous. In some studies depression correlated positively with severity, as measured by the Hurley score (15), and with clinical stage (3), while in other studies depression and clinical severity did not correlate (18, 19).
The aim of this study was to estimate the prevalence of depression in patients with HS, its association with demographic and clinical variables, and with QoL.
Study design
This is a cross-sectional, observational study, on patients with HS. The study was approved by the Institutional Ethical Committee of IDI-IRCCS (459/1, 9 November 2015).
Patients with hidradenitis suppurativa
Consecutive patients with a diagnosis of HS were recruited between August 2016 and October 2019 at the dermatological hospital IDI-IRCCS, in Rome, Italy. These patients are part of the Italian HS registry (20), but our Institutional protocol, besides the Dermatology Life Quality Index (DLQI) requested by the national registry, also includes an additional set of patient-reported outcomes (see below).
Inclusion criteria were: (i) age 16 years or over; (ii) both sexes; (iii) a new diagnosis of HS or presenting for the first time to the hospital with HS; (iv) history of at least 6 months of nodules, abscesses, draining tunnels, and secondary retracting scars, affecting intertriginous sites, including axillae, breasts, groin, buttocks, and perineum; and (v) written informed consent, signed by the patient or by a parent/guardian for patients less than 18 years of age. Exclusion criteria were: (i) inability to understand Italian; (ii) inability to understand the questionnaires; and (iii) Major psychiatric disorders.
Outcome measure: 12-item General Health Questionnaire
The 12-item General Health Questionnaire (GHQ-12) is a self-administered instrument designed to detect non-psychotic and minor psychiatric disorders. Each item assesses the presence or frequency of a possible mental problem and it is rated on a 4-point scale (less than usual, no more than usual, rather more than usual, or much more than usual). In this study, the GHQ-12 was scored with the binary scoring method, collapsing adjacent responses to obtain a dichotomous scoring (0-0-1-1). Patients with a score of 7 or more were defined as “GHQ cases” of depressive disorder. This cut-off has been shown to have good sensitivity and specificity to identify cases of major depressive disorder (MDD) in patients with skin conditions (21). Since the GHQ-12 is not a diagnostic tool, “GHQ cases” are possible cases of depression. However, to simplify, we refer to them throughout this paper as patients with depression.
Quality of life: Skindex-17 and Dermatology Life Quality Index
The Skindex-17 questionnaire (22) measures the impact of skin conditions on patients’ QoL. It consists of 17 items that constitute 2 subscales: symptoms and psychosocial. Answers are given on a 3-point scale (0: never; 1: rarely/sometimes; 2: often/always), on which higher scores indicate a higher impact on QoL. Scale scores were transformed to a linear scale, with scores ranging from 0 to 100. The DLQI (23) is a dermatology-specific health-related QoL questionnaire, which consists of 10 questions with possible answers from 0 (“not at all”) to 4 (very much”). The total score is obtained by adding the score of each item. Higher scores indicate a higher impact on QoL.
Health status: 36-item Short Form Health Survey
The 36-item Short Form Health Survey (SF-36) (24) is a generic indicator of health status. It includes 36 items intended to measure 8 dimensions: physical functioning, role limitations due to physical health problems, bodily pain, general health, vitality (energy/fatigue), social functioning, role limitations due to emotional problems, and mental health. The physical dimensions (i.e. the first 4 dimensions) can be summarized into the Physical Component Summary (PCS), while the Mental Component Summary (MCS) is obtained from the remaining dimensions. Scores for each domain range from 0 to 100, with higher scores indicating a better status. It has been shown that the MCS and the mental health (MH) scales of the SF-36 may be used as a screening instrument to detect psychological disorders, such as anxiety and depression. The presence of depression in our population was also evaluated using these scales, with scores ≤ 56 for MH and ≤ 42 for MCS, as defined in a population with rheumatoid arthritis (25).
Clinical severity: International Hidradenitis Suppurativa Severity Score System
The International Hidradenitis Suppurativa Severity Score (IHS4) (26) is a scoring system obtained by the number of nodules, plus the number of abscesses (multiplied by 2) plus the number of draining tunnels (multiplied by 4). HS is defined as mild/moderate if the score is < 11 points and severe if the score is ≥ 11 points.
Collected data and procedures
Patients were informed about the study and signed the consent in the waiting room, where, if they agreed to participate, they completed the questionnaires (GHQ-12, Skindex-17, DLQI and SF-36). Moreover, sociodemographic and clinical data were recorded. For the purpose of this study, the following variables were used: sex, age, educational level, body mass index (BMI), smoking, duration of the disease, visual analogue scale (VAS) for pain, number of fistulas, abscesses, nodules and scars.
Statistical analysis
Categorical variables were described as number and percentage, and continuous variable as mean and standard deviation (SD). The prevalence of patients with GHQ-12≥7 was compared in subgroups of patients according to sex, age, educational level, BMI, smoking, duration of the disease, VAS pain, number of fistulas, abscesses, nodules and scars, using the χ2 test. Mean values of IHS4, of the Skindex-17 symptoms and psychosocial scales, of the DLQI, and of the SF-36 PCS and MCS scales were compared between patients with possible depression (i.e. GHQ-12≥7) and without depression using Mann–Whitney U test. Also, mean SF-36 scale scores were compared between patients with or without possible depression, using Mann–Whitney U test, and were represented graphically. Correlation among instruments was calculated using Spearman’s rank correlation coefficient.
During the study period, 373 patients were considered eligible for the study and were included in the registry. There were very few refusals (approximately 2%). Data on GHQ-12 were complete for 341 patients. There were 210 (61.6%) women, and the mean (SD) age was 32.4 (11.9) years; 52.8% of patients had severe HS (i.e. IHS4 ≥ 11).
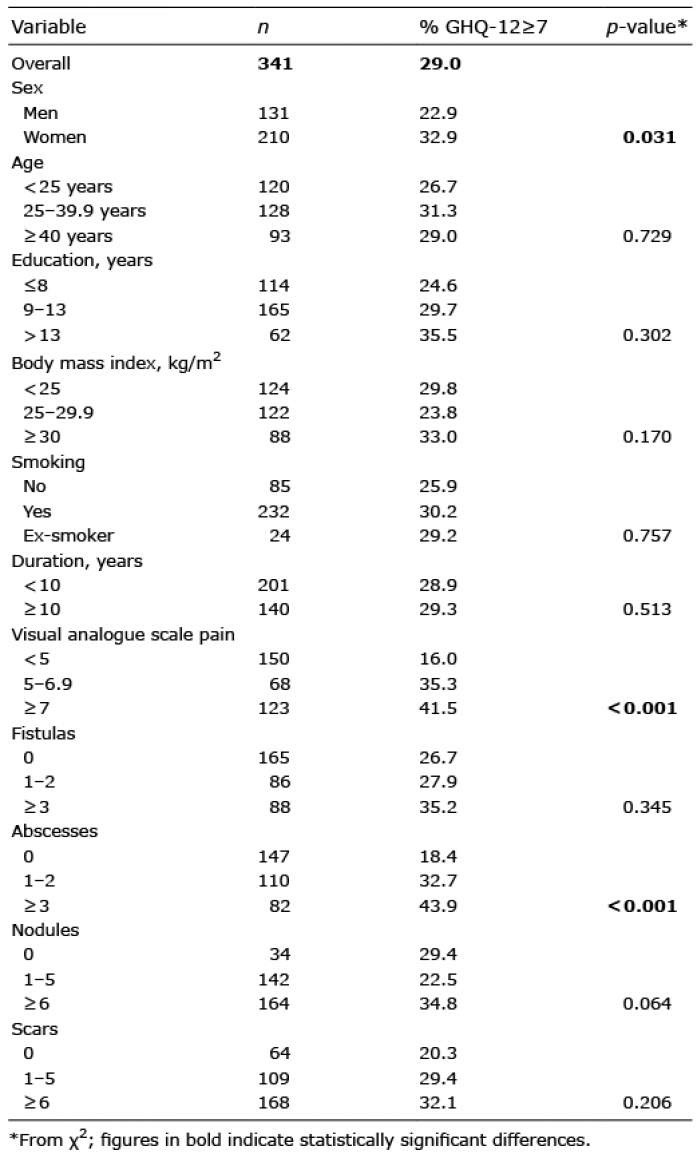
Overall, the frequency of patients with GHQ-12≥7 was 29.0%. It was higher in women than in men (32.9% vs 22.9%, p = 0.031) (Table I). No significant differences were observed according to age categories, educational level, BMI, smoking, disease duration, number of fistulas and scars. The prevalence of depression was strongly associated with VAS pain and number of abscesses. Although not significant, it was higher in underweight and overweight patients and in patients with a high number of nodules. Concerning clinical severity (Table II), mean IHS4 scores were significantly higher in patients with GHQ-12≥7. In patients with IHS4 score < 11 there were 22.4% of patients with depression vs 35.0% in patients with severe condition, i.e. IHS4 score ≥ 11. Table II also shows that QoL scores, obtained using both the Skindex-17 and the DLQI, were significantly higher in patients with depression. All single items of the Skindex-17 were significantly associated with the presence of depression. Furthermore, SF-36 mean scores were significantly lower in patients with GHQ-12≥7 compared with patients with GHQ-12<7, both for the summary scales (PCS and MCS) and for the 8 scales, as shown in Fig. 1 (p < 0.001 for all scales). According to the MCS and the MH scale of the SF-36, the proportion of patients with depression was 48.8% and 61.4%, respectively. Eighty-seven percent of patients who were classified as positive for depression with the GHQ-12 were positive also with the MCS, and 90.1% were positive also with the MH scale.
Table I. Frequency of depression (12-item General Health Questionnaire (GHQ-12)≥7) in 341 patients with hidradenitis suppurativa according to sociodemographic and clinical variables
Table II. Mean values of clinical severity, quality of life and health status scores according to the presence of depression in 341 patients with hidradenitis suppurativa
Fig. 1. 36-item Short Form Health Survey (SF-36) scales mean scores in 341 patients with hidradenitis suppurativa according to the presence of depression evaluated with the 12-item General Health Questionnaire (GHQ-12) (depression=GHQ-12≥7). PF: physical functioning; RP: role limitations due to physical health problems; BP: bodily pain; GH: general health; VT: vitality; SF: social functioning; RE: role limitations due to emotional problems; MH: mental health.
The highest correlation coefficients (close to 0.6) among instruments were observed between GHQ-12 and the psychosocial scale of the Skindex-17 and the SF-36 MCS. A moderate correlation was observed between GHQ-12 and the physical scales of both the Skindex-17 (symptoms) and the SF-36 (physical). In contrast, there was a poor correlation between GHQ-12 and clinical severity. In general, clinical severity poorly correlated with all the QoL instruments, except for the SF-36 PCS. There was poor correlation between PCS and MCS, while the correlation between symptoms and psychosocial scales of the Skindex-17 was high.
In this study, a high prevalence of depression was observed in patients with HS. A previous study (27) on psychiatric morbidity in HS reported that at least one mental disorder was diagnosed in 24.1% of patients, and that major depression was the most common of these (15.3%). In the current study, the prevalence of depression was estimated using the GHQ-12, which has been shown to be able to detect major depressive disorders in skin conditions using the cut-off score of 6/7 (21). Cut-off scores of 8 or 9 were observed to be the most effective to detect depression in a group of university students (28). However, the instrument was administered in a student psychiatric clinic, where students may tend to report more psychological symptoms. In a group of leprosy patients, the optimal cut-off for the GHQ-12 for detecting any psychiatric disorder, and not specifically depression, was 4/5 (29). In a population-based study (30), the cut-off was 3/4; however, the scales were studied against mental health service use, which is not the same as having a mental disorder. The cut-off that was used in the present study has been specifically calculated for skin disorders, in a dermatological reference centre, using as a gold standard the SCID-I standardized psychiatric interview administered by certified mental health professionals, yielding psychiatric diagnoses according to the the Fourth version of the Diagnostic and Statistical Manual of mental disorders (DSM-IV). The other cut-off for skin conditions, i.e. 3/4 (31), allows the detection of patients with minor psychiatric disorders, and is not specific for depression. The GHQ was used also in another study on HS (32) in the 28-item version, with a cut-off of 6, which resulted in a prevalence of cases of 50%. In the current study population, the prevalence of depression was 29%, which is in line with most other studies. For example, Onderdijk et al. (15) found a prevalence of 21% in 211 patients with HS using the Major Depression Inventory (MDI) questionnaire, and in the study by Vangipuram et al. (19) 24.4% of patients with HS had a diagnosis of depression according to the ICD-10. However, even a very low prevalence of 1.6% was observed (13) using the ICD-10 classification, as well as higher values, such as 37.8% (14), using the Hospital Anxiety and Depression Scale (HADS). This may, in part, be due to several combinations of different populations, study designs, and instruments used. Some studies were retrospective (19, 27), while the majority were cross-sectional. As expected, a higher prevalence was more frequently observed when a screening instrument was used, compared with a clinical-criteria based diagnosis of HS. Then, the low prevalence of 1.6% observed in the study by Thorlacius et al. (13) concerned patients with disease activity within the past 5 years.
The prevalence observed in patients with HS has been shown to be higher than that of most of other skin conditions. For example, in an analysis of the single items of the Skindex-17 (4), HS ranked first among 29 skin conditions for the item “I feel depressed”. Also, compared with non-dermatological chronic conditions (5), the mental health component of the SF-36 was significantly worse than that of several medical conditions, and very similar to mental health conditions.
In the present study, a high concordance in the identification of patients with depression was observed using the GHQ-12 and the MCS and MH scale of the SF-36. However, the SF-36 scales classified as depressed double or more the number of the patients identified by the GHQ. This could be because the cut-offs were calculated for a different condition, and the authors did not use a clinical diagnosis as the gold standard. Although the estimates obtained using the SF-36 appear to be extremely high, it should be noted that in 2 other recent studies in which the SF-36 was used in a sample of patients with HS (33, 34), we also observed unprecedented levels of poor health.
Patients with HS with depression reported a significantly worse QoL and general health status compared with patients with no depression. In particular, depression scores highly correlated with the psychosocial scale of the Skindex-17 and the mental scale of the SF-36. In contrast, correlation was moderate between GHQ and the physical components of both instruments. Also, although in the current study the mean IHS4 score was significantly higher in patients with depression compared with patients with no depression, the overall linear scores of these 2 measures scarcely correlated. In addition, Frings et al. (17) did not find a significant correlation between depression, as measured by the HADS and Hurley stage, and in another study (19) depression was not even associated with the Hurley stage. In the current study, correlation was low also between clinical severity and QoL measures, even with regard to their symptomatic component (i.e. a moderate correlation of approximately 0.3). Similarly, in previous studies, moderate coefficients were observed between DLQI and Hurley score (r = 0.28) (15), and between Skindex-29 emotion scale and Sartorius score (r = 0.31) (17). Other studies reported no significant association between clinical severity, as measured by Hurley staging, Sartorius scale, and IHS4 score, and QoL (4), and a poor correlation between physician severity scores and QoL (18).
These results also support previous findings concerning other skin conditions, such as psoriasis (35, 36), which indicate that there is not a linear correlation between clinical severity and the psychosocial impact of a disease. In fact, clinical severity measures are based mainly on clinical signs, which do not necessarily correspond with the burden that the disease places on the patient. HS is a condition with a strong psychosocial impact even at a low clinical severity level, so it is not surprising that, in the current study population, 22.4% of patients with IHS4 score < 11, i.e. mild/moderate severity, reported depression.
From a methodological point of view, it is notable that, even with moderate values, the symptomatic scales of QoL instruments correlated better with depression than did IHS4. This shows that the symptomatic component of QoL instruments include patient-centred aspects and thus measures a different construct compared with a mere clinical severity measure.
Study limitations
A limitation of this study is that it evaluated depression using the GHQ, which is a screening instrument and is not intended as a diagnostic tool. Moreover, the cross-sectional design of this study does not allow us to draw conclusions on the direction of the association between depression and the presence of HS; the association is probably bidirectional. A recent study (37) concluded that patients with major depressive disorders had an increased risk of developing autoimmune skin diseases, such as HS, compared with controls.
Conclusion
In conclusion, depression is a frequent condition in patients with HS, as reported in previous studies. Depression is an important comorbidity, since it is, in turn, associated with other aspects; for example sexual health impairment (3), and perception of pain (38) (which is the main symptom in HS). Also, the current study observed a strong association between depression in patients with HS, and pain, as well as with a high number of abscesses (which are some of the most impairing manifestations of the disease, and are also associated with pain). In addition, the study found an association between depression in the study population and being either obese or overweight, which confirmed findings concerning the general population (39).
It is important for dermatologists to take into account the presence of depression in patients with HS and consider the need for psychiatric consultation in order to improve patients’ QoL.
This study was supported in part by the “Progetto Ricerca Corrente 2019” of the Italian Ministry of Health, Rome, Italy.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize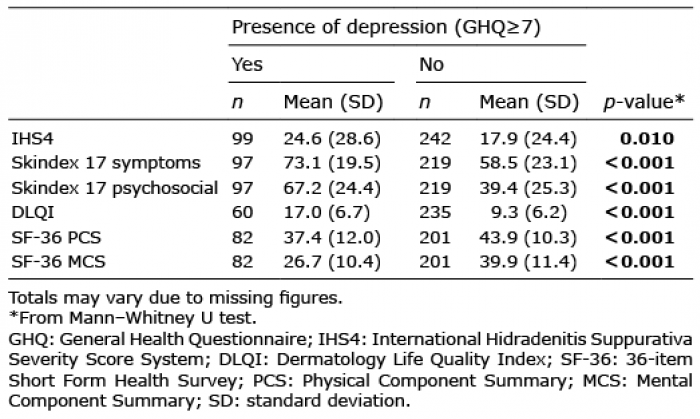 Click to show fullsize
Click to show fullsize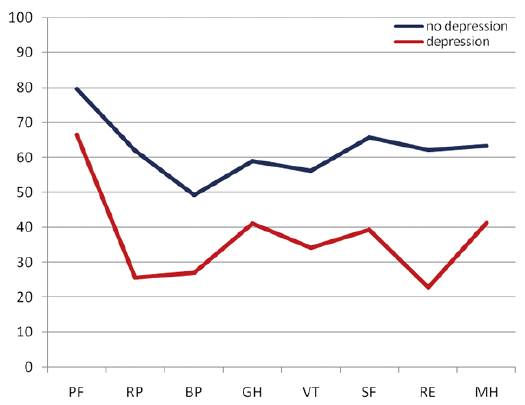 Click to show fullsize
Click to show fullsize