


1Department of Dermatology, Sheba Medical Center, Tel HaShomer, Ramat Gan, and 2Institute of Pathology, Sheba Medical Center, Tel HaShomer, Ramat Gan, Israel affiliated to the Sackler Faculty of Medicine, Tel Aviv University, Tel Aviv, Israel
#These authors contributed equally to this work.
Rituximab targets the B-lymphocyte antigen CD20, providing pemphigus vulgaris patients with long-term remissions. However, the effects of repeated cours-es have not yet been established. This study aimed to evaluate the effect of repeated rituximab courses on remission length in pemphigus vulgaris. A total of 73 patients with pemphigus vulgaris treated with rituximab at a single centre were retrospectively analysed. Of 73 study participants (28 men, 45 women), 42 (58%) received a 2nd course of rituximab, 24 (33%) received a 3rd course, 4 (6%) received a 4th course, and one (1%) received a 5th course. Rituximab remained efficacious in each course, irrespective of previous treatments (complete remission 75–81%). Following the 2nd and 3rd courses, the results indicated longer remissions with reduced flare-ups, and the remission length increased with each subsequent course. We conclude that rituximab serves as a disease-modifying agent, notably for patients with moderate-to-severe pemphigus vulgaris.
Key words: repeated course; rituximab; pemphigus vulgaris; remission.
Accepted Sep 24, 2020; Epub ahead of print Sep 28, 2020
Acta Derm Venereol 2020; 100: adv00286.
doi: 10.2340/00015555-3649
Corr: Sharon Baum, Department of Dermatology, Sheba Medical Center, Tel HaShomer, Ramat Gan, Israel. E-mail: sharon.baum@sheba.health.gov.il
A proportion of patients with pemphigus vulgaris treated with rituximab achieve complete remission; nevertheless, relapses generally occur at 6–12 months after the first treatment. We observed that with repeated cycles of treatment with rituximab, high efficacy is maintained and remission can be induced despite failures in previous cycles. With each subsequent cycle, an improvement is observed, with a substantially longer remission time, thus we conclude that rituximab is a potent disease-modifying agent in these patients.
Pemphigus vulgaris (PV) is an autoimmune, chronic, blistering disease characterized by the formation of autoantibodies against the intercellular proteins desmogleins 1 and 3, which results in an intraepidermal split, causing blisters and erosions of the skin and mucous membranes (1). Systemic corticosteroids are the cornerstone of therapy. Adjuvant therapies, which typically focus on general immunosuppression, are used to maintain disease-free periods and act as steroid-sparing agents (2). The principal therapeutic goal is disease control with reduced corticosteroid-related toxicity (3). Relapses are treated by increasing the dose of steroid or by adding or replacing an immunosuppressant. However, adjuvant treatments occasionally lead to numerous side-effects without sufficient benefits. Extensive research has been directed at the identification of an optimal steroid-sparing agent that can also serve as a disease-modifying agent (3, 4).
Rituximab (Rituxan®; Genentech, San Francisco, CA, USA; MabThera®; Roche, Basel, Switzerland) is a monoclonal antibody targeting the B-lymphocyte antigen CD20 and is currently licensed for the treatment of moderate-to-severe PV by the US Food and Drug Administration (FDA) and the European Medicines Agency (EMA) (5–7). A review conducted by Ahmed & Shetty (8) revealed that disease control was observed in 90–95% of patients with PV within ≤ 6 weeks of treatment initiation. Complete remission (CR) was observed within 3–4 months, whereas the majority of patients remained on minimal steroid or immunosuppressive therapy (8). Despite this excellent initial response, several patients experience flares of PV within 6–24 months, and the role of rituximab in managing these flares is well described (9–20). Nevertheless, most studies included a limited number of patients and only a few cycles, thus making it difficult to evaluate the long-term efficacy of rituximab. Hence, the current study aimed to evaluate the efficacy of repeated cycles of rituximab on remission length and to determine its role in the treatment of patients with refractory PV.
A total of 73 patients diagnosed with PV and treated with rituximab (at least 42 patients with 2 rituximab courses) at the Department of Dermatology in Sheba Medical Center, Israel, between June 2009 and October 2018 were analysed retrospectively. A diagnosis of PV was dependent on the clinical appearance of mucosal and/or cutaneous lesions compatible with PV, confirmatory histopathological findings that indicated suprabasal epidermal acantholysis, and evidence of intercellular immunoglobulin G (with or without C3 binding) deposits in the epidermis/epithelium with a net-like pattern on direct immunofluorescence.
The US FDA has approved rituximab dosing regimens for non-Hodgkin’s lymphoma (NHL) and rheumatoid arthritis (RA) (21). The dosing regimens administered to our patients changed with time according to the common practice employed at that temporal point. From 2009 to 2013, the NHL regimen consisted of intra-venous infusions of 375 mg/m2 once weekly for 4 consecutive weeks. From 2014, the RA regimen consisted of 2 infusions of 1,000 mg, provided 2 weeks apart. Prior to rituximab initiation, all patients received a detailed explanation about this drug (including measures for the prevention and control of infection), underwent general clinical and laboratory examination, and were administered vaccinations/preventive treatment as indicated. All patients received infusions at the Dermatology Day Care Unit, a clinical unit in the Department of Dermatology at Sheba Medical Center (22). During follow-up, patients were examined at least once in 3 months by 2 dermatology specialists who recorded their clinical status.
The following data were collected: patients’ demographics, clinical history (skin and mucous membrane involvement, disease duration prior to rituximab treatment, and previous adjuvants administered), dates and dosing of rituximab treatment, disease severity before and after treatment, and time to relapse following each course. Response to treatment was defined as complete, partial, or absent in accordance with the consensus statement (23). Briefly, a relapse or flare-up is defined as the appearance of ≥ 3 new lesions per month that do not spontaneously heal within one week, or the extension of known lesions in a patient whose disease was previously under control. Remission is defined as partial remission (PR) or CR on or off therapy (minimal adjuvant therapy and/or ≤ 10 mg prednisone).
This study was conducted in accordance with the principles outlined in the Declaration of Helsinki and was approved by the Institutional Review Board (reference number 7172-09-SMC). The requirement for acquisition of informed consent was waived owing to the retrospective nature of the study.
Statistical analysis
Categorical variables are presented as frequencies and percentages, whereas continuous variables are expressed as mean ± standard deviation (normally distributed) or as median and interquartile range (non-normally distributed). The distribution of continuous variables was evaluated using a histogram. A reverse censoring method was employed to describe the length of follow-up. Kaplan–Meier curves were utilized to describe disease relapse during follow-up, and the log-rank test was used to determine the association between categorical variables and disease relapse. Univariate Cox regression was applied to examine the association between continuous variables and disease relapse. All statistical tests were 2-sided, and a p-value < 0.050 was considered to indicate statistical significance. Statistical analysis was performed using Predictive Analytics Software Statistics® version 24.
Patient characteristics
The patients’ demographic and clinical data are presented in Table I. A total of 73 patients (28 men, 45 women) received the 1st course of rituximab. The effect of this course, with a limited follow-up period, in 18 of these patients has been reported previously (24). All patients treated with rituximab were deemed to be recalcitrant (i.e. having a “stubborn” disease). They were previously administered multiple adjuvant agents and/or steroids that could not be tapered to a dose lower than 20 mg per day, over a period of time, while a positive clinical response was not achieved. Instead, these patients continuously deteriorated.
Table I. Patients’ demographic characteristics
Previous therapies
Prior to the 1st course, all patients were treated with prednisone. Seventeen patients received rituximab as the first-line adjuvant treatment, whereas 56 patients received at least 1 and up to 6 (mean 2.4) of the following adjuvant treatments: methotrexate (27 patients), dapsone (30 patients), azathioprine (18 patients), mycophenolate mofetil (MMF; 42 patients), cyclophosphamide (4 patients), cyclosporine (3 patients), intravenous immunoglobulin (8 patients) and plasmapheresis (5 patients).
The 17 patients who received rituximab alone did not differ from their counterparts with respect to age, sex, and prednisone doses before and after rituximab treatment. However, 12 out of these 17 patients (70%) required only one course; among those who received adjuvants prior to rituximab treatment, only 33% required a single cycle. The mean follow-up period for the latter group of patients was 87 months, compared with 35 months for the former group.
MMF was the most common adjuvant treatment and was the last to be administered prior to initiation of rituximab. No significant difference in disease duration was observed between patients who received MMF as the only adjuvant prior to rituximab treatment and those who received it as the last of their adjuvants. In most patients, treatment was terminated due to insufficient clinical response.
First rituximab cycle
The median prednisone dose prior to the 1st rituximab course was 30 mg (range 20–60 mg), which was reduced to 5 mg (range 0–5 mg) at 3 months after rituximab treat-ment. A reduction in the prednisone dose was observed with each successive rituximab cycle (Table I).
All patients discontinued adjuvant therapy during the follow-up period, and 46 flare-ups were recorded during that time (10% at 12 months, 42% at 18 months, and 55% at 24 months; Fig. 1). The median time to flare-up was 20.6 months. As shown in Fig. 1, the relapse rate following each successive rituximab cycle was lower (p = 0.027). Compared with the 1st treatment, there was a 50% chance of relapse after the 2nd treatment (hazard ratio (HR), 0.50; 95% confidence interval (95% CI) 0.30–0.84) and the risk decreased by approximately one-third after the 3rd treatment (HR 0.39; 95% CI 0.17–0.90).
Fig. 1. Survival curves showing the time to relapse after each cycle of rituximab. Number at risk=number of patients at risk for disease relapse at a given point in time. Each successive treatment was associated with a lower risk of relapse. Compared with the 1st treatment, there was a 50% chance of relapse after the 2nd treatment, and the risk decreased by approximately one-third after the 3rd treatment.
There were no statistically significant correlations among the type of disease involvement, disease duration, prednisone dose prior to treatment, treatment protocol (NHL or RA), and relapses after the 1st, 2nd, and 3rd rituximab courses. However, an increased flare-up risk was observed in elderly patients, compared with younger patients (HR 1.05; 95% CI 1.01–1.08; p = 0.010). This also applies to relapses after the 2nd and 3rd rituximab courses. Among all adjuvant treatments administered prior to rituximab initiation, only MMF was associated with reduced flares on completion of rituximab cycles (p = 0.001).
A total of 31 patients (28 who achieved complete remission and 3 who attained partial remission treated with low-dose prednisone and topical potent steroids) were not in need of a 2nd course.
Second rituximab cycle
Out of the 73 (58%) patients included in this study, 42 received at least 2 courses of rituximab treatment; the clinical data of these patients are presented in Table I. These 42 patients did not differ from the 31 patients in whom one course was sufficient with respect to age, sex, disease duration, age at disease onset, rituximab initiation, and site of involvement. However, patients who received fewer adjuvants had a better chance to remit following a single course (p < 0.05). Of the 42 patients who received a 2nd rituximab course, 25 (59%, or 33% of all patients) experienced a relapse. Flares occurred in 9%, 17%, and 32% of the subjects at 12, 18, and 24 months, respectively (Fig. 1). The median time to relapse was 37.5 months.
Third rituximab cycle
Twenty-four subjects (12 men, 12 women) received a 3rd rituximab course; of these subjects, 5 (20%, or 6% of all patients) relapsed once more and 4 received a 4th course. Only one patient received 5 courses during the follow-up period. After each cycle, fewer patients required an additional cycle of rituximab.
The mean remission length was 20 months (range 17–23.5 months), 30 months (range 23–37 months), and 31 months (range 23–38.5 months) after the 1st, 2nd, and 3rd rituximab courses, respectively. This represents a prolongation of the remission interval with each successive treatment; i.e. by 9.5 months after the 2nd course (range 2–17 months, p = 0.012) and by 10.5 months after the 3rd course (range 2–19 months, p = 0.014). The mean remission period following the 3rd course lasted one month longer than that following the 2nd course; however, this did not reach statistical significance. When the remission interval was evaluated according to sex, women experienced significantly longer remission periods between the 2nd and 3rd courses than did men (33.8 vs 38.0 months, p = 0.019).
Summary of rituximab cycles
Fig. 2 shows the flowchart describing the cohort’s clinical response to treatment. All patients achieved either PR or CR within a short period following a rituximab cycle, and such efficacy was retained during subsequent courses (CR rates of 81%, 79%, and 75% after the 1st, 2nd, and 3rd cycles, respectively). An insufficient response to a treatment cycle was not predictive of the patient’s response to the ensuing cycle.
Treatment tolerance
Rituximab was generally well tolerated. One patient developed pneumonia after the 1st course, and another experienced weakness as a side-effect of the treatment. One patient died in November 2013 due to an unexpected complication during endoscopic retrograde cholan-giopancreatography for suspected gallstones.
Fig. 2. Pemphigus vulgaris: a flow chart describing the patients’ clinical response following the administration of rituximab treatments. CR: complete response; PR: partial response; NR: no response; pat: patients.
Rituximab is a highly effective treatment for PV (5, 9–20, 25). The current study involving 73 patients with refractory PV not only further supports its efficacy, but also sheds light on issues that can be addressed only when one evaluates repeated cycles. Although the role of rituximab in managing flares of the disease is well described (9–20), most studies included a limited number of patients and only a few cycles, thus making it difficult to evaluate the long-term efficacy of rituximab. The current study included a relatively large cohort of patients with PV only who were treated with > 2 rituximab cycles and followed up for a relatively long period. Table II summarizes the findings of studies that examined the effects of repeated rituximab cycles. Due to heterogeneity in patients, rituximab protocols, and reported outcomes, a true comparison among these studies is challenging.
Table II. Publications dealing with repeated rituximab cycles
The first and most important issue emerging from the current study is that rituximab is potentially a disease-modifying agent; i.e., substantial improvement was observed with each subsequent cycle, and this was associated with fewer flare-ups, longer remissions, and a “crescendo” effect. Theoretically, after a limited number (individually determined for each patient) of courses, pemphigus can therefore be cured in several patients (Fig. 1). One can realize that by the end of all cycles, most patients achieved CR at a rate of > 90%. In this respect, our study supports the findings of Cianchini et al. (9) for a larger cohort of PV patients with a longer follow-up period, which is in line with the report by Colliou et al. (10). This finding is not surprising, considering that high efficacy is maintained with repeated cycles of rituximab and that remissions can be induced despite previous fail-ures with rituximab, as was clearly shown in the current study and by others (9, 10, 12). The “crescendo” effect of rituximab was outlined in a recent case report describing a patient with severe oral PV who received 4 cycles of rituximab over a period of 7 years. The patient’s clinical response was progressive with respect to his oral severity score and response rate (26).
Our study further supports the notion that when rituximab is administered as the first adjuvant and fewer adjuvants are, in general, administered prior to rituximab, the overall response to rituximab is superior (10, 16). Given this finding as well as the beneficial effect of rituximab on the disease course, it is preferable to administer rituximab as the first-line adjuvant treatment (along with corticosteroids). Additional support for this approach comes from Colliou et al. (10), who noted CR at the last follow-up in 100% of patients who received rituximab as the first-line adjuvant treatment, compared with 29% of patients who did not receive it. Dissimilar to the patients reported by Colliou et al. (10), our patients who received rituximab did not have a milder disease; however, they were followed up for a shorter period and, accordingly, had a shorter disease duration. We also noted that there is less of a need for a 2nd rituximab course when rituximab is used as the first-line adjuvant treatment. Hence, one can infer that the response to repeated cycles of rituximab is dependent not only on disease severity, but also on disease duration and, consequently, on other adjuvants used prior to rituximab initiation. The effect of disease duration on the response was previously suggested by Kim et al. (12). This latter finding may be accounted for by the “epitope spreading phenomenon” (27). In fact, in the current study, better outcomes were attributed to younger patients and those who were treated with MMF prior to rituximab initiation.
The reduction in prednisone dose on completion of each rituximab cycle and the lower starting dose at the beginning of each cycle served as additional verifications of treatment efficacy, which is in agreement with the literature (13). This is indicative of either the efficacy of the adjuvant administered before rituximab initiation or the efficacy of prior rituximab course (13).
Reducing the prednisone dose does not affect the success of rituximab treatment, as was confirmed by a recent prospective randomized trial. This trial showed that the combination of first-line rituximab with short-term, low-dose prednisone resulted in a higher CR rate and a lower adverse event rate when compared with a higher dose and long-term prednisone treatment alone. Thus, avoiding the adverse effects associated with long-term systemic corticosteroid use is possible (5).
The use of rituximab during relapses only or as a proactive treatment within a specific time-frame requires further evaluation. Most studies used it as needed, at different dosages, and in different schedules (Table II). Nonetheless, as shown in our study, when a full course is provided as needed or is administered as needed, but at a reduced dose of 500 mg at 6-month intervals, rituximab retains its high potency. A previous study involving 29 patients treated with rituximab, with an additional dose (500 mg) during a relapse, concluded that the need for additional courses increased at 6 months after rituximab initiation and peaked at 12 months after therapy (28). Furthermore, an additional prophylactic infusion of rituximab administered at 6 months after the 1st course has been reported to be not beneficial, as 3 out of 10 treated patients relapsed (vs 5 out of 9 patients who did not) (23). However, it was noted that treatment during relapse led to faster consolidation (3 months) compared with that following the 1st rituximab cycle (12 months) (29), supporting the notion that time to remission is reduced with repeated courses.
The effectiveness and safety of first-line rituximab therapy with proactive administration of 500 mg at 12 and 18 months were evaluated. Additional maintenance doses were administered in all patients, irrespective of their clinical status. Although 89% of patients achieved CR, most relapses were observed at 6–12 months after treatment initiation, suggesting that the 1st maintenance dose would be more beneficial if provided at 6 months (5).
In the current study, a proactive approach was adopt-ed in only one patient, who received additional rituximab courses, resulting in CR. Based on our survival curve analysis, if one chooses the proactive approach, to prevent relapses, a 2nd course is advocated at 6–12 months after the 1st (Fig. 1).
An additional issue that remains unresolved is whether one of the dosing protocols used (haematological vs rheumatological) has an advantage over the other. This could not be addressed in the current study and in others because patients received rituximab according to the accepted practice at the time gained from other medical fields and according to their insurance policies. How-ever, few studies claim that the haematological protocol is superior to the rheumatologic protocol in achieving sustained CR (Table II) (11, 12, 14).
One of the drawbacks of rituximab therapy is its association with higher rates of infection and mortality. This was not evident in this series, and even with repeated cycles, serious adverse effects were not observed. We believe that the observed safety of rituximab is related to our meticulous administration protocol, the admin-istration setting chosen, and our policy involving the cessation of additional immunosuppressive therapies following infusions.
Study limitations
The current study has several limitations, including its retrospective nature, relatively small cohort, and lengthy follow-up period. Furthermore, all patients had moderate-to-severe disease, and disease severity could not be assessed using the pemphigus severity scale. The use of 2 treatment regimens affected the cumulative dose per patient and might have manipulated the results.
Conclusion
Rituximab is a promising treatment option for severe PV. Complete remission is achieved in the majority of patients. Rituximab is an effective steroid-sparing agent and has a positive long-term clinical effect if used repeatedly during relapses. With each subsequent cycle, an improvement is observed with a substantially longer remission time, thus rendering rituximab a potent disease-modifying agent. Future prospective randomized controlled trials may benefit from correlating clinical and laboratory data on CD19+ / CD20+ B-cell counts and autoantibody titres.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize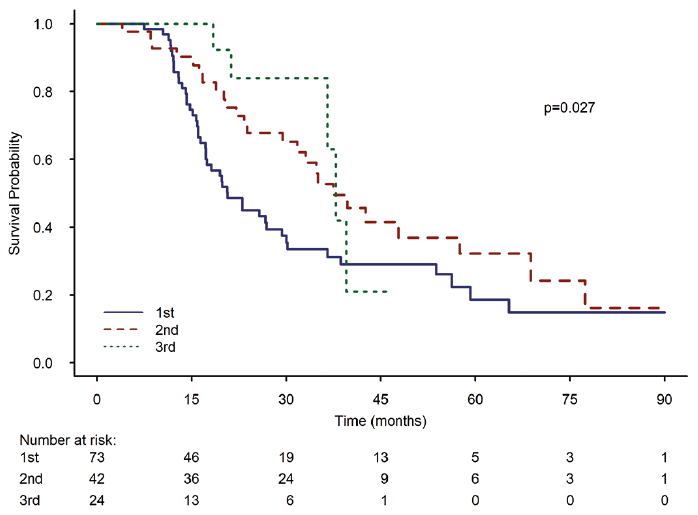 Click to show fullsize
Click to show fullsize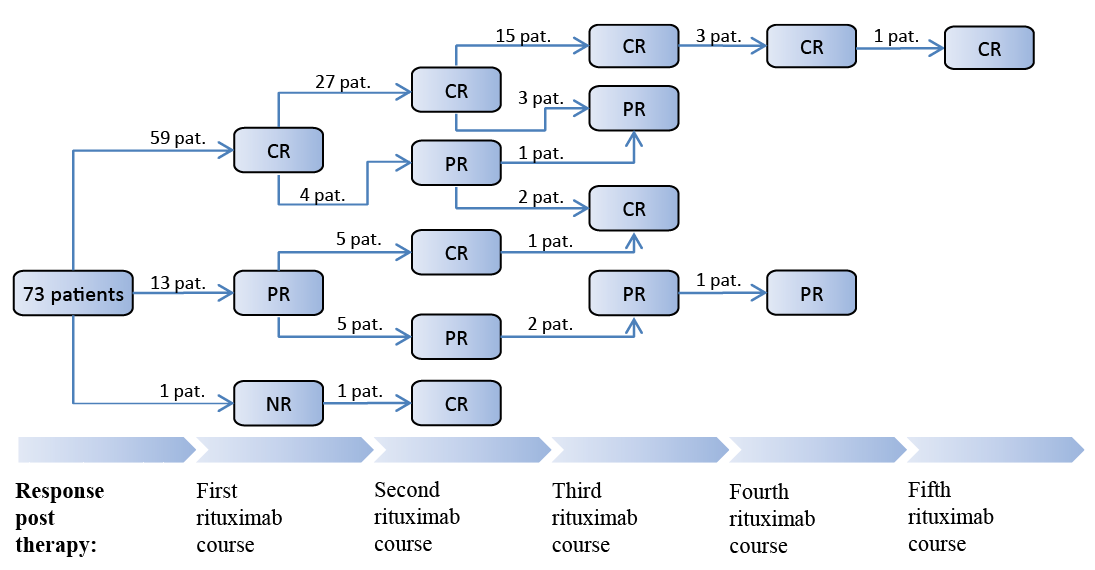 Click to show fullsize
Click to show fullsize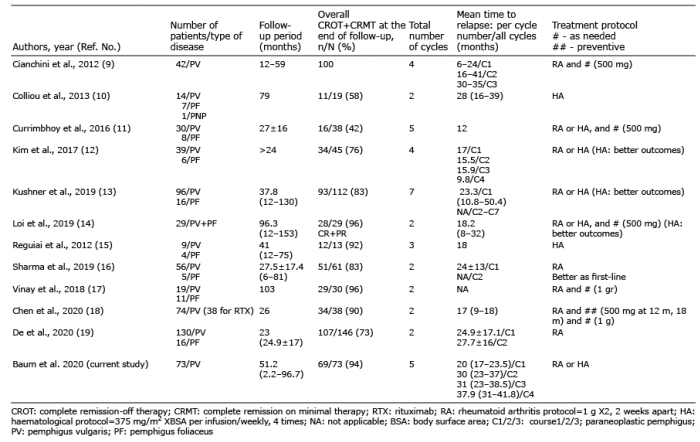 Click to show fullsize
Click to show fullsize