


1Department of Dermatology and Medical Research Center Oulu, Oulu University Hospital; PEDEGO Research Unit, University of Oulu, FIN-90220 Oulu, 2Department of Dermatology, Turku University Hospital and University of Turku and 3Department of Biostatistics, University of Turku, Turku, Finland. *E-mail: kaisa.tasanen@oulu.fi
Accepted Oct 2, 2020; Epub ahead of print Oct 7, 2020
Acta Derm Venereol 2020; 100: adv00297.
doi: 10.2340/00015555-3656
In clinical research, the use of data retrieved from health registries and biobank samples is becoming more common (1). The information contained in these data repositories is based on diagnoses entered into medical records during daily clinical practice. In general, Finnish health registries have been shown to be an accurate and reliable source of information (2), but the dermatological diagnoses contained therein have not previously been validated. This study aimed to validate the diagnostic code used to record cases of psoriasis in the databases of 2 Finnish biobanks (Oulu and Turku).
In November–December 2019, biobank personnel retrieved the recent records of 100 consecutive patients containing the diagnostic code for psoriasis (International Classification of Diseases – 10th revision (ICD-10) code L40.0) from the Borealis biobank in Oulu, and 100 from the Auria biobank in Turku (www.finbb.fi). These biobanks are based on specialized (tertiary) care. Patients treated in the University hospitals of Oulu and Turku are asked for permission to include their biological samples in the biobank. Currently, there is no data about the participation rate. The records of 196 patients, matched by sex and age, containing the diagnostic code for type II diabetes mellitus (E11) were selected as a control group. The intention of the control group was to identify any unregistered diagnoses of psoriasis. Patients with diabetes were chosen because patients with psoriasis have an elevated risk of diabetes (3), and therefore selecting such a control group may have increased the likelihood of encountering unregistered cases of psoriasis. This study was approved by FinBB, which is a consortium of Finnish biobanks, and the University Hospitals of Oulu and Turku. Study data were collected and managed using REDCap electronic data capture tools (4) hosted at the University of Turku. Counts and percentages are presented for categorical variables. An exact 95% confidence interval (CI) was calculated for the positive predictive value (PPV).
Data were extracted from the patients’ electronic medical records by a dermatologist or experienced resident. The records of the psoriasis group were checked for clinical findings that are characteristic of psoriasis (sharply demarcated and erythematous papulosquamous lesions), but not of any other dermatological condition. Age at onset, psoriasis type, and receipt of any treatment used for psoriasis were recorded, as were any symptoms or diagnosis of psoriatic joint disease. A diagnosis was defined as “uncertain” if the record contained evidence clearly supporting a diagnosis, but the diagnosis was not set by dermatologist. The medical records of the control group were reviewed carefully in order to find cases of psoriasis that were not registered with the appropriate diagnostic code. The criterion for validity of a psoriasis diagnosis was that: (i) a dermatologist or a registrar had stated typical clinical findings for psoriasis; or (ii) psoriasis-like findings and one of the following: histological findings supporting a diagnosis, a recorded score on the Psoriasis Area Severity Index (PASI), nail findings typical of psoriasis, psoriatic arthritis diagnosed by a rheumatologist, or a note in the records of a first-degree relative with diagnosed psoriasis. Plaque psoriasis, psoriasis arthritis with typical skin symptoms and guttate psoriasis were accepted as “psoriasis” in this validation study.
Based on these criteria, the diagnosis in 12 patients from the psoriasis group could not be verified by the electronic medical records, and the diagnosis was uncertain for a further 12 patients. Consequently, the study found the PPV to be 88.0% (95% CI 82.7–92.2). All the patients with an “uncertain” diagnosis seemed to be psoriasis cases, but with symptoms so mild that they did not warrant a dermatological appointment at a university hospital and therefore lacked a confirmatory diagnosis by a dermatologist. Of those with a diagnosis recorded with the code L40.0, 12 records contained clinical findings typical of dermatological conditions other than psoriasis. Among these, findings consistent with pustulosis palmoplantaris were the most frequent, being present in 6 of the records. Three patients in the control group had psoriasis based on chart review, resulting in a negative predictive value (NPV) of 1.5%.
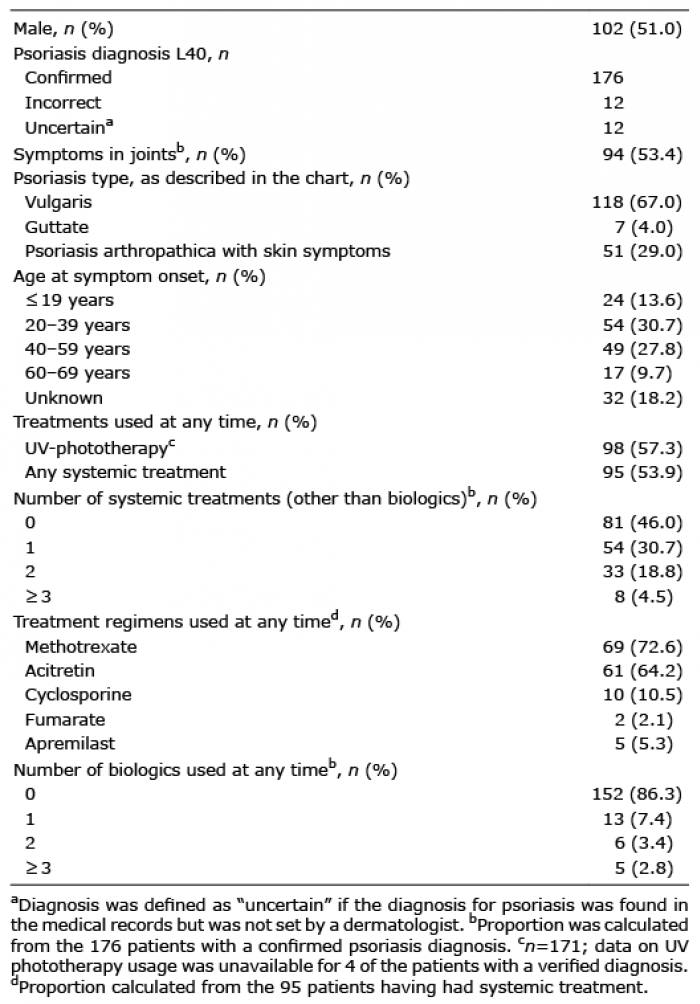
A small majority of the psoriasis group (51.0%) were males. Most cases had psoriasis vulgaris (Table I). A diagnosis of psoriasis arthropathica had been set for a quarter of cases, but almost half of patients had joint symptoms. This probably reflects the high frequency of arthrosis symptoms. We analysed the psoriasis treatments used by the 176 patients with a verified psoriasis diagnosis. More than half (57.3%) had received ultraviolet (UV) phototherapy and nearly as many (54.0%) systemic therapy other than biologics, of which methotrexate and acitretin were the most used. Biologics were used by 13.6%, with most of these having received only one biologic (Table I). There were no reports of psoriasis having been triggered by the use of biologic treatments.
Table I. Demographics and treatment usage of the psoriasis group (n = 200)
A recent Italian study reported as high as 98.9% PPV for psoriasis when using either a dermatologist’s diagnosis or psoriasis medications as search criteria (5). A recent Danish study found a PPV of 97.1% among patients treated in tertiary referral dermatology clinics (6). The lower PPV (88.0%) found in the current study may be due to the fact that it was based on diagnosis codes registered in biobank registries rather than dermatology clinics. Our findings are comparable to those of a study from the USA in which a PPV of 90% was found for psoriasis diagnoses set by dermatologists (7). However, the validity of the psoriasis diagnoses recorded in Finnish biobank registries seems to be higher than in Sweden, where a registry validation study for psoriasis covering all healthcare utilizations, i.e. primary and specialized care, found a PPV for psoriasis of 81% (8). An even lower PPV (68.7%) was found in another study from the USA, which included psoriasis diagnoses from all healthcare settings (9). Previously, a British study analysed the psoriasis diagnoses in a registry based on general practitioners’ (GP) coding. It found that as many as 91% of the codes in the GP registry had been set by dermatologists (10), but the study did not verify the accuracy of the original diagnoses. A Dutch study reported PPV for GP diagnoses psoriasis being 62%, but increasing up to 82% if anamnestic information about psoriasis lesions were considered (11). It is noteworthy that the current study enables identification of psoriasis as the exposure, not the outcome.
This study categorized as “uncertain” all psoriasis diagnoses that lacked verification by a dermatologist, although the chart review revealed these diagnoses to be reliable, but mild. This was the cases also for those 3 in control group who had psoriasis mentioned in their charts. This finding may disturb registry and biobank data-based research if the study and control populations are not large enough. It was decided not to collect the information about PASI scores because the procedure of administering the PASI differs between hospitals. However, since more than half of the current patients with psoriasis had been treated with UV-phototherapy and/or systemic treatments, their psoriasis can be defined as moderate-to-severe.
Based on these findings, we conclude that the use of the ICD-10 code L40.0 is a reasonably valid approach when selecting patients with psoriasis from biobank registries.
The FinnGen-project provided salaries for SH and AV.
Conflicts of interest: SH has received an educational grant from Celgene. AV has received educational grants from AbbVie, Jansen, Novartis, and Celgene. LK has attended advisory boards for Abbvie, Eli Lilly, Janssen, Leo Pharma, Novartis, Sanofi, UCB Pharma. KT has received educational grants from Novartis and Pfizer and honoraria from Novartis, Abbvie, Janssen-Cilag, SanofiGenzyme and Lilly for consulting and/or speaking. LH has received educational grants from Shire, Janssen-Cilag, Novartis, AbbVie and LeoPharma, honoraria from SanofiGenzyme, Novartis, Abbvie and UCB Pharma for consulting and/or speaking and is an investigator for Abbvie. EL and SP have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize