


1Sorbonne Université, INSERM, Institut Pierre Louis d’Épidémiologie et de Santé Publique (IPLESP), Paris, 2Department of Dermatology, CHU Pontchaillou, Rennes, 3Fédération Française de Formation Continue et d’Evaluation en Dermatologie-Vénéréologie, Pontoise, 4Department of Dermatology, AP–HP, Hôpital Henri-Mondor, Créteil, France, UPEC Université Paris Est–Créteil Val-de-Marne, and 5EA 7380 DYNAMYC, UPEC Université Paris Est–Créteil Val-de-Marne, France
#These authors contributed equally to the study.
Patients with flares of seborrhoeic dermatitis were compared with control outpatients seen during the same time-period in a case-control study, and with themselves while in remission in a case-crossover study. All patients consulted the same office-based dermatologist. During the study period, 189 cases and 189 controls were included in the case-control study, and 81 cases in the case-crossover study. Multivariate analysis was performed. Case-control study results were the following: past history of tobacco consumption (odds ratio (OR) 2.2 (95% confidence interval (CI) 1.1–4.6)), conflict as a dispute during the past month (OR 10.6 (95% CI 1.0–114.3)), alcohol consumption on a regular basis (OR 10.2 (95% CI 2.0–52.6)), and higher level of stress during the past month (OR 8.2 (95% CI 3.4–19.9)). Case-crossover study results were the following: higher level of stress during the past month (OR 4.5 (1.7–12.2)), association borderline significant for higher level of alcohol consumption (OR 5.4 (0.8–34.9)). These risk factors for flares of seborrhoeic dermatitis should be taken into account carefully in the daily management of seborrhoeic dermatitis.
Key words: seborrhoeic dermatitis; stress; alcohol.
Accepted Oct 7, 2020; Epub ahead of print Oct 13, 2020
Acta Derm Venereol 2020; 100: adv00292.
doi: 10.2340/00015555-3661
Corr: Olivier Chosidow, Department of Dermatology, AP-HP, Hôpital Henri Mondor, FR-94010 Créteil, France. E-mail: olivier.chosidow@aphp.fr
Seborrhoeic dermatitis is a chronic, inflammatory skin condition, with alternating flares and remission periods. The aim of this study was to evaluate risk factors for flares of seborrhoeic dermatitis in a population of French patients consulting the same office-based dermatologist. During the study period, 189 cases and 189 controls (without seborrhoeic dermatitis) were included in a case-control study, and 81 cases (to be compared with themselves while in remission) were included in a case-crossover study. Higher levels of stress during the past month and, probably, higher levels of consumption of alcohol were found to be associated with seborrhoeic dermatitis. These risk factors should be taken into account carefully in the management of flares.
Seborrhoeic dermatitis (SD) is a chronic, inflammatory skin condition with alternating flares and remission periods. It has a predilection for areas rich in sebaceous glands, such as the scalp, medial part of the eyebrows, glabella, nasolabial fold and, less frequently, the trunk or genitalia (1). SD is characterized by poorly defined erythematous patches covered with large greasy scales that detach easily. SD affects 2–14% of the general population in Japan, China, Australia, the Netherlands (2–5), and is potentially more prevalent in men and older people (6), with a prevalence of up to 20–30% of some selected populations (7–10). SD may have a psycho-social impact on patients, particularly due to scaling scalp and facial localization (1).
SD has been reported to be associated with several conditions, including HIV infection, Parkinson’s disease, alcoholism, depression, cancers of the upper respiratory and digestive tracts and Down syndrome, but, except for HIV infection and cancers, those associations have not been sufficiently documented (7, 10–15). SD has also been reported to be triggered by stress (16). Regarding sun exposure, SD is thought to worsen during less sunny seasons, and improve after exposure to sunlight (17, 18), although the prevalence of SD is high in people exposed to a high level of ultraviolet (UV) radiation, such as mountain guides or those exposed to UVA therapy for psoriasis (8, 19).
Although SD is a very common skin condition, a prospective quantification of risk factors of flares has not been frequently undertaken in large populations. While a cross-sectional study has been performed in the Netherlands (5), the evaluation of risk factors using a different methodology, such as simultaneous case-control and case cross-over design, is not available to date.
The aim of the current study was to evaluate risk factors for seborrhoeic dermatitis flares in a population of French patients consulting the same office-based dermatologist.
Patients and setting
The study took place in outpatient settings between September 2005 and December 2011. A total of 119 dermatologists, from all regions of France except oversea territories, participated in the study. The dermatologists were recruited via mailings, communications at congresses, or through professional associations of dermatologists. They were asked to prospectively include adult patients with “active” or “inactive” SD, as well as unaffected patients as controls (see below).
Case-control study
Patients with either a past history of, or an active form of, SD could be included as cases and were compared with control patients. Active SD was clinically defined as erythema or scaling of one or more of the following areas: hair-line, scalp, eyebrows, medial part of the eyebrows, glabella, nasolabial or chin folds. Control patients were outpatients seen by the investigators during the same period. Controls could be recruited if their medical history was free of SD, psoriasis and eczema, and if their reasons for consultation were a dermatological disease other than one of these 3 conditions. Cases and control patients were matched on age (± 5 years) and sex. After written consent was obtained, an included patient was asked to complete a questionnaire including socio-demographic and clinical data (age, sex, profession, weight, height, number of SD flare-ups during the past 2 years, tobacco and alcohol consumption during the past month, perceived stress assessed using the Cohen scale (20), quality of life assessed using the validated French version of the Skindex (21)). For each included patient, dermatologists also completed a questionnaire regarding the skin condition motivating the consultation, the past medical history, and the characteristics of SD for patients included as cases.
Case-crossover study
Patients included as cases were assessed as potential participants for a case-crossover study. After the first visit and their inclusion in the case-control study, all patients who visited the same dermatologist for a second time were asked to be included in the case-crossover study if they had presented with an active SD during the first visit and an inactive SD during the second visit or vice versa. Using this approach, each patient was considered as her/his own control. Potential risk factors for SD flares (e.g. stress level, alcohol or tobacco consumption, calendar season) were compared between flare and quiescent periods. The second visit questionnaire was distributed by dermatologists, if applicable, or sent by post.
Statistical analysis
Continuous variables are presented as median, first quartile (Q1) and third quartile (Q3), and categorical variables as proportions. For the case-control study, groups were compared by univariable conditional logistic regression. For the case-crossover study, groups were compared using Wilcoxon signed-rank test for continuous variables and McNemar’s test for categorical variables. Univariable and multivariable conditional logistic regression analyses were performed to assess the risk factors for SD in both case-control and case-crossover studies). Parameters with a p-value ≤ 0.10 in univariable analyses were included in the multivariable model. The final multivariable models were obtained by using a backward stepwise procedure based on log likelihood ratio to eliminate non-significant (p-value > 0.05) variables from the initial model. No interaction terms were included in the models. A Markov Chain Monte Carlo Method was used to impute the missing data. All analyses were performed using SAS software 9.3 (SAS Institute Inc, Cary, NC, USA).
The study was approved by the French Advisory Committee on Information Processing in Material Research in the Field of Health (Comité Consultatif sur le Traitement de l’Information en Matière de Recherche dans le Domaine de la Santé, CCTIRS (number 05.193) and by the National Commission of Informatics and Liberty (CNIL), according to French law (number 905239)).
Study population
During the study period, 189 cases and 189 controls were included in the case-control study, and 81 cases in the case-crossover study. The characteristics of cases and controls are shown in Table I. The 189 controls visited their dermatologists mainly for follow-up of naevi (n = 41, 21.7%), acne (n = 26, 13.8%), cutaneous warts (n = 19, 10.1%), or rosaceiform eruption (n = 10, 5.3%). Description of SD in cases is shown in Table II. During the first visit, SD was active for 163 participants (86.2%) included as cases, and inactive for 25 (13.2%) out of the 189 patients (data missing for one patient). Patients reported that SD started at approximately 25 years of age. Almost half of the patients (47.3%) reported that SD was permanent, while it evolved following a flare/remission scheme for 52.7% of patients. At examination, the most frequent localization of SD was the nasolabial folds (n = 132), followed by the medial part of the eyebrows (n = 106) and the hairline (n = 95); at least 3 areas were affected for 69 (36.5%) patients.
Table I. Characteristics of patients included in the case-control study
Table II. Patients’ description of seborrhoeic dermatitis (SD)
Case-control study
In univariable conditional logistic regression models, 5 parameters were associated with manifestations of SD, i.e. past history of tobacco consumption, usual consumption of alcohol, higher consumption of alcohol during the past month, higher level of stress during the past month, and professional or personal conflict during the past month. After applying a backward stepwise procedure, 3 variables were independently associated with SD, i.e. past history of tobacco consumption, alcohol consumption, and higher level of stress during the past month (Table III).
Table III. Parameters associated with the risk of seborrhoeic dermatitis: multivariate analyses
Case-crossover study
A total of 81 (42.9%) out of the 189 patients included as cases were included in the case-crossover study. Of these, 47 (58.0%) were male and their median age was 49 years (41.5–58.0) . The median time between first and second visit at the dermatologist’s office was 24 months (11–44). During the first visit, SD was active for 64 (79.0%) and inactive for 17 (21.0%) of the 81 patients. Compared with the remission period, flares of SD were associated with a significantly higher score on the Skindex scale (17.8 (10.3–27.7) vs 10.3 (5.2–15.5), p < 0.0001), but there was no significant difference regarding the Cohen stress scale (1.36 (1.07–1.86) vs 1.39 (0.93–1.79), p = 0.21). In univariable analysis (Table IV), 2 parameters were associated with flares, i.e. higher consumption of alcohol and higher level of stress during the past month. In multivariable analysis, higher level of stress during the past month was still strongly associated with the risk of SD flares (OR 4.5 (1.7–12.2), p = 0.003) while the association was borderline significant for higher consumption of alcohol (OR 5.4 (0.8–34.9), p = 0.08). No seasonality was found for risk of flares, which was not increased during winter compared with other seasons.
Table IV. Factors associated with seborrhoeic dermatitis flare-up
Although SD may be confined to the scalp (dandruff), these results suggest that SD seen by dermatologists is generally most severe, and more frequently has a facial localization.
The case-control study of 189 patients with SD supported the view that tobacco and alcohol consumption and level of stress were factors significantly associated with SD motivating a dermatological consultation. Moreover, the case-crossover study showed that more recent alcohol consumption and higher levels of stress during the past month were associated with SD flares in patients known to have documented SD, as is strongly suggested by both doctors’ and patients’ experience. Several risk factors associated with SD have been advocated, with controversial results, such as male sex, age, obesity, skin phototype, education, hypertension, depression, stress, and diet (5, 22). In a cross-sectional study performed in military personnel in South Korea (23), SD was associated with impaired Skindex (as well as in atopic dermatitis and tinea cruris) with a documented correlation with the amount of stress. In a cross-sectional study performed in the Netherlands, men and older people with a light and dry skin were at higher risk of SD (5). Moreover, a diet with a high fruit intake was associated with a lower risk of SD (22). In the current study, neither tobacco consumption nor seasonality was associated with risk of SD flares. As cases and controls were enrolled by the same dermatologist, and therefore were living in the same geographical area, it was not possible to study the impact of sun exposure. The impact of facial SD, which is a chronic skin condition with potential numerous flare-ups, on quality of life has already been proposed, and the current study showed that the Skindex score was much higher in people with flares than in the SD population without flare-ups. SD evidently has a measurable psycho-social burden in real-life.
Study strengths and limitations
The current study has several strengths. It has a large population of patients and controls of both sexes. Patients were examined and interviewed by dermatologists, and the collected information is therefore reliable. Some patients had SD flares; other patients were in remission, suggesting good external validity. The study took into account most of the factors strongly suspected to be associated with SD flares, such as alcohol and tobacco consumption, and stress level. Moreover, the study used 2 methodological approaches, i.e. case-control and case-crossover designs, allowing different questions in a population of SD with and without flare-ups, and the converging results provide strong confidence in the findings. Finally, since the onset of this research, other studies confirmed the current results (23, 24).
The study also has some limitations. First, it would have been of interest to study the relationship with a potential underlying disease (e.g. HIV, cancer, neurological disease, arterial hypertension) on the risk of having SD. Some of these associations have been poorly documented and rely almost exclusively on case reports or small series (7, 10–15). However, this was not possible in the current study because of the low number of cases and controls with these underlying diseases. In fact, the current study was not designed for those endpoints, while a cross-sectional study showed an association of SD with hypertension (24). As controls were matched according age and sex, it was therefore not possible to detect a difference between sexes. However, the influence of sex differences on SD is controversial, as shown in 2 cross-sectional studies (5, 25). Secondly, the study period was 6 years, during which 378 patients were recruited. This figure may be considered as not reflective of the number of patients with SD seen by dermatologists. However, during this study period, new health policies were adopted in France, including the implantation of the referent general practitioner reform (law of the 13 August 2004: https://www.legifrance.gouv.fr). As a consequence, the patients had to visit their general practitioner to access any specialist (including the dermatologist) and it is likely that most of the patients with SD were therefore treated directly by their GP without being referred to a dermatologist or even self-medicated. Nevertheless, it is likely that all consecutives cases seen by dermatologists were not included in the study and the most severe cases may have been more likely to be included. Thirdly, a certain degree of residual confounding cannot be ruled out, since we could not control for ethnic background, socioeconomic status, or lifestyle factors, such as sun exposure, profession, or nutrition. Potential confounding conditions, such as psoriasis, obesity, and hypertension, were not collected, and various comorbidities, such as psoriasis, acne, rosacea, and contact dermatitis, were not taken into account (6). Finally, the current study showed that it was difficult to set up clinical research in the office-based dermatologist setting, although this should be the standard for common diseases, in order to increase applicability to daily care.
Conclusion
In conclusion, this study confirms the risk factors for SD flares in a large sample of patients, presenting to a dermatology clinic; mainly, recent level of consumption of alcohol and high level of stress during the past month before the SD flare-up. Those risk factors should be taken into account carefully in the daily management of SD flares, although a formal intervention study is needed for definitive confirmation of such a therapeutic strategy.
The authors thank S. Consoli, for help in determination of quality of life scales, and M. Bayle-Lenglet, A. Bellut, J. P. Claudel, C. Courtieu, A. Lorent, J. Martel, I. Mironneau, J. C. Ortoli, S. Reberga, M. Schollhammer, J. F. Sei, E. Tisserand, and P. Zukervar, for their help in recruiting investigators.
This study is dedicated to J. C. Guillaume, MD, deceased in December 2018. He was a mentor in French dermatology clinical research in general, and helped in designing this study in particular.
Funding sources: Fujisawa, Galderma, Glaxo-Smith-Kline, Labcatal, Merck-Lipha-Santé, Novartis, Pierre Fabre Dermatologie Companies*. (*Names of the pharmaceutical companies at the time of the study).
Role of funding sources. The funding sources had no role in the design and conduct of the study; collection, management, analysis, or interpretation of the data; preparation, review, or approval of the manuscript; or decision to submit the manuscript for publication.
Conflicts of interest. DC reports grants from Janssen (2017 to 2018), and MSD France (2015 to 2017), personal fees from Janssen (2016, 2018), MSD France (2017) and Gilead France (2018) for lectures, personal fees from Innavirvax (2016) and Merck Switzerland (2017) for consultancy, outside the submitted work. PB: Consultant for Galderma, Cosmétique active France, Celgene, Naos, Lilly. OC is PI of the PsoBioTeq cohort supported by unrestricted research grants from the French Ministry of Health (PHRC AOM 09 195), the French agency for drugs (ANSM), Abbvie, Janssen, Pfizer, and MSD France. AD is member of the Scientific committee of the PsoBioTeq cohort supported by unrestricted research grants from the French Ministry of Health (PHRC AOM 09 195), the French agency for drugs (ANSM), Abbvie, Janssen, Pfizer, and MSD France. The other authors have no conflicts of interest to declare.
Investigators: Hill-Sylvestre MP, Peyron E, Bouilly-Auvray D, Gougne-Mahoudeau B, Guihard W, Heudes AM, Payenneville JM, Berthod F, Charleux D, Colcombet-Navarranne A, Corgibet F, Courtois JM, Illy G, Khallouf R, Leveque L, Loche F, Penso-Assathiany D, Pillette-Delarue M, Auffranc JC, Biard B, Bourseau-Quetier C, Cartier H, Catala S, Chastenet M, Collas-Cailleux H, Forestier JF, Gaboriaux-Pegaz MC, Gallay I, Laumaillé-Cadiou C, Lepeytre P, Meyer M, Meyer-Muller A, Pariente E, Perrin-Nicolet C, Rabouille I, Recanati G, Rey R, Royer-Chaze E, Sales D, Thiebot B, Truche C, Valembois C, Van Landuyt H, Zabarino P, Aguilaniu-Dupuy F, Antoni-Bach N, Ardisson C, Assouly P, Bamberger T, Beaulieu I, Beer F, Bieder C, Bochaton-Michaud H, Bombert S, Bouissou FX, Boulanger A, Bourdet D, Bourrel M, Bousquet-Sage C, Cabarrot A, Carmi E, Charpentier A, Charrier B, Cohen B, Colomb M, Cordier N, Delbarre M, Delhalle E, Dournon AM, Dufour C, Favre E, Ferry P, Fourcade-Lasnier C, Gand-Gavanou J, Gaudard S, Génolier-Weiller A, Gscheidel D, Guetrot D, Guichard C, Guillot M, Gutmann-Heller A, Hoang-Xuan D, Kouri N, Labourdette V, Labrousse-Pommellet V, Largier R, Le Goaer C, Le Ru Y, Legoff-Levan S, Levet R, Libert P, Ly S, Maghia R, Magne F, Maillet M, Mazgaj C, Monsarrat C, Moraillon I, Morin C, Motreff C, Papillon S, Peu Duvallon P, Pincemaille V, Quelen B, Renaut JJ, Rivollier C, Roby J, Romieux F, Schenck F, Schollhammer M, Sirieix P, Sirieix-Sorhouet M, Tiscornia C, Toussaint H, Treffandier O, Valet O, Vigan M, Waeytens D, Walther S.


 Click to show fullsize
Click to show fullsize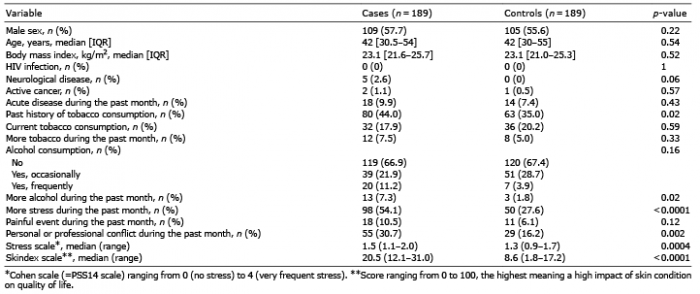 Click to show fullsize
Click to show fullsize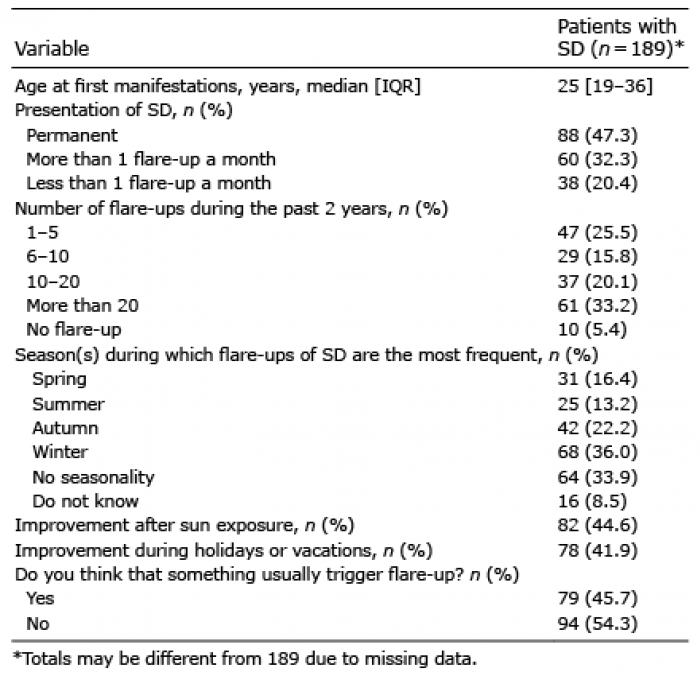 Click to show fullsize
Click to show fullsize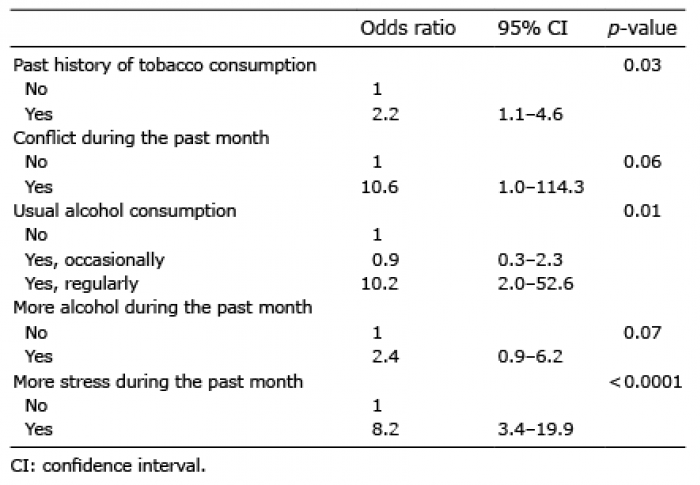 Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize