


1Oaro Dermatology Institute, Seoul, Republic of Korea, 2Guam Dermatology Institute, Guam, USA, 3Department of Dermatology, Dankook University, College of Medicine, Cheonan, 4Department of Dermatology, Chung-Ang University, College of Medicine, Seoul, and 5Department of Dermatology, Dongtan Sacred Heart Hospital, Hallym University College of Medicine, Hwaseong, Republic of Korea
A variety of applications of human adipose tissue stem cell-derived exosomes have been suggested as novel cell-free therapeutic strategies in the regenerative and aesthetic medical fields. This study evaluated the clinical efficacy and safety of adipose tissue stem cell- derived exosomes as an adjuvant therapy after application of fractional CO2 laser for acne scars. A 12-week prospective, double-blind, randomized, split-face trial was performed. A total of 25 patients received three consecutive treatment sessions of fractional CO2 laser to the whole face, with a follow-up evaluation. Post-laser treatment regimens were applied; for each patient, one side of the face was treated with adipose tissue stem cell-derived exosomes gel and the other side was treated with control gel. Adipose tissue stem cell-derived exosomes-treated sides had achieved a significantly greater improvement than the control sides at the final follow-up visit (percentage reduction in échelle d’évaluation clinique des cicatrices d’acné scores: 32.5 vs 19.9%, p < 0.01). Treatment-related erythema was milder, and post-treatment downtime was shorter on the human adipose tissue stem cell-derived exosomes-treated side. In conclusion, the combined use of this novel material with resurfacing devices would provide synergistic effects on both the efficacy and safety of atrophic acne scar treatments.
Key words: adipose tissue stem cell-derived exosomes; acne scar; fractional laser.
Accepted Oct 15, 2020; Epub ahead of print Oct 19, 2020
Acta Derm Venereol 2020; 100: adv00310.
doi: 10.2340/00015555-3666
Corr: Gyeong-Hun Park, Department of Dermatology, Dongtan Sacred Heart Hospital, Hallym University College of Medicine, 7, Keunjaebong-gil, Hwaseong-si, Gyeonggi-do 18450, Republic of Korea. E-mail: borelalgebra@gmail.com
Adipose tissue stem cell-derived exosomes possess the critical properties of mesenchymal stem cells in the repair of organ injuries. Furthermore, adipose tissue stem cell-derived exosomes can avoid the risks of stem cell therapy because they are cell-free. A double-blind, randomized, first-in- human, clinical trial was conducted to evaluate the efficacy and safety of highly purified adipose tissue stem cell-derived exosomes as an adjuvant therapy after fractional CO2 laser application for acne scars. Application of adipose tissue stem cell-derived exosomes treatment yielded more favourable responses, a shorter recovery time, and fewer side- effects. The combined use of adipose tissue stem cell-derived exosomes with resurfacing devices could provide synergistic effects on the efficacy and safety of atrophic acne scar treatments.
Facial atrophic acne scarring is a psychologically damaging condition that can cause social disability. Fractional laser resurfacing has widened therapeutic options and has become the current standard of care (1–3). While ablative fractional carbon dioxide laser (FCL) resurfacing has demonstrated clinical efficacy in acne scar treatment, patients still need better improvement of scars and sustain side-effects during post-procedural wound healing (4). Therefore, an adjuvant application of adipose-derived stem cell (ASC)-conditioned medium (CM) has been tried, with synergistic effects in augmenting treatment responses and reducing adverse effects through its potential to accelerate tissue regeneration and wound healing (5).
Because mesenchymal stem cells (MSCs) can differentiate into various cell types as multipotent stem cells, their unique self-renewal capacities have made them a promising cell-based therapy to treat several human diseases (6). However, there have been several drawbacks in the use of MSCs, such as poor engraftment efficiency, potential tumour formation, and difficulty in quality control (7). Furthermore, paracrine signalling of MSCs is reported to be essential for their beneficial effects on tissue regeneration and anti-inflammation.
Exosomes are lipid bilayer-enclosed extracellular vesicles, 30–200 nm in diameter, produced by almost all cells and present in all body fluids (8–10). They are regarded as an essential mediator of intercellular communication by transferring proteins and genetic material between cells (9). Several studies have shown that MSC-derived exosomes carry the essential properties of MSCs (11–13), suggesting that exosomes may be a compelling alternative to MSCs in regenerative and aesthetic medicine, as they would avoid most of the problems associated with live MSC-based therapy (14). Interestingly, recent studies have shown that human adipose tissue stem cell-derived exosomes (ASCE) possess the critical properties of stem cells and are as potent as MSCs in the repair of various organ injuries (15, 16). In fact, a variety of applications for ASCE have been suggested as novel cell-free therapeutic strategies in regenerative and aesthetic medicine. These data strongly suggest the suitability of ASCE as an adjuvant treatment modality in combination with FCL for the treatment of acne scars.
Since most single treatment modalities for acne scars yield less than ideal results with regard to efficacy and safety, customized combination treatments with various therapeutic methods are needed for optimal outcomes. Therefore, the aim of this study was to evaluate the clinical efficacy and safety of ASCE as an adjuvant therapy after application of FCL for acne scars.
Study design and patient enrollment
A 12-week prospective, double-blind, randomized, split-face, comparative study was conducted to evaluate the clinical efficacy of application of ASCE after FCL in the treatment of facial acne scars. The study was carried out in accordance with the Declaration of Helsinki and approved by our institutional review board. Informed consent was obtained from all subjects prior to enrollment. In this study, patients received 3 consecutive treatments of FCL on their whole face at an interval of 3 weeks, with a follow-up evaluation 6 weeks after their final treatment session. An independent researcher created the random allocation sequence by a computer-based random number generator, using block randomization with a block size of 4 to assign the post-laser treatment modality of each half of the face between ASCE and control gel. The allocation was concealed from subjects and investigators, and was preserved by using sequentially numbered, sealed envelopes.
Twenty-five Korean subjects (18 men and 7 women, age range 19–54 years, 12 with Fitzpatrick skin type III and 13 with type IV) with atrophic acne scars were enrolled between October and November 2019. The sample size was determined based on feasibility, because previous data for power analysis were not available. Patients whose échelle d’évaluation clinique des cicatrices d’acné (ECCA) scores were 50 or higher were eligible for inclusion (17). Patients were excluded from the study if they had active acne under treatment or if they had received any other treatments for acne scars during the 12 months prior to the first treatment. Other treatments, including chemical, mechanical, or laser resurfacing, were not permitted during the study period.
Exosome purification and preparation of adipose tissue stem cell-derived exosomes gel for clinical application
Exosomes in this study were acquired from human ASC-CM by ExoSCRT™ technology (ExoCoBio Inc., Seoul, Republic of Korea) as described previously (18). Briefly, CM was collected from ASCs cultured with serum-free Dulbecco’s Modified Eagle’s Medium (Thermo Fisher Scientific, Waltham, MA, USA) in a 5% CO2 atmosphere at 37°C. Collected CM was filtered through a 0.2-μm filter to remove non-exosomal particles. Exosomes were further concentrated and purified by tangential-flow filtration with a 500-kDa molecular weight cut-off filter membrane cartridge. Quantification of exosomes was performed by nanoparticle tracking analysis (NTA).
ASCE were prepared as gel solutions at 2 different doses for clinical application. To prepare the ASCE gel, ASCE were prepared at 9.78×1010 particles/ml (for the day of FCL treatment) or 1.63×1010 particles/ml (for days subsequent to FCL treatment) in a gel solution containing 30% ASCE. Detailed information on the ASCE and control gel solution is described in Appendix S1. To maintain blinding of investigators and subjects, the ASCE and control gel solutions were prepared with identical syringes, labelled left and right.
Treatment protocol
The entire face of each patient was treated with 10,600-nm FCL (Fraxis, Ilooda, Suwon, Korea). The face was cleansed with mild soap and topical anaesthesia was applied using EMLA® cream (Astrazeneca, Södertälje, Sweden) to the entire face under occlusion for 30 min prior to laser therapy. The treatment parameters were determined based on each patient’s condition and availability as follows: 7.2–9.0 mJ, 240–300 μs duration, and 0.8–1.0 mm density in FCL (coverage=20–25%, each pixel size=100 μm, and approximate depth=1,100–1,400 μm, treatment density 120–160 microthermal zones/cm2). Each treatment session encompassed the entire face for two passes.
Post-laser treatment regimens were applied as follows: all patients were treated with 1 ml of either ASCE gel or control gel on each half of the face according to random assignment just after finishing the laser treatment. For the next two consecutive days after each treatment, patients were instructed to apply each solution to the designated half of the face twice a day as described.
Clinical outcome assessment
All patients were photographed using a standardized digital camera (EOS 600D, Canon, Tokyo, Japan) under identical lighting conditions at each visit. Efficacy of scar improvement was assessed by the ECCA score at each visit, as well as the Investigator’s Global Assessment (IGA) at the final follow-up visit (17). IGA was evaluated using a 5-point scale associated with the degree of improvement (grade 0=no improvement, 1=1–25% improvement, 2=26–50% improvement, 3=51–75% improvement, and 4=76–100% improvement) (19, 20). For ECCA scoring, atrophic acne scars were classified into specific subtypes including icepick (V-shaped), boxcar (U-shaped), and rolling scar (M-shaped) according to their shape and size (17, 21), and the ECCA score was determined according to the number of each subtype of scar, as previously described (17). Two experienced dermatologists rated ECCA scores and IGA on the basis of the photographs in a fully blinded manner. The primary efficacy outcome was the percentage change in total ECCA score at the final follow-up visit. Secondary outcomes were the percentage change in total ECCA at weeks 3 and 6, the change in ECCA score for each subtype of atrophic scar at weeks 3, 6, and 12, and IGA at week 12.
Meanwhile, patients recorded the post-treatment responses, including erythema, oedema, and dryness with a 0–3 severity scale (0=none, 1=mild, 2=moderate, and 3=severe), daily for 7 days after each treatment session. Daily pain scores for the first post-treatment week were also recorded with a 0–10 severity scale (0 for no pain, 10 for the worst imaginable pain) during each post-treatment period. Other post-procedural complaints, including hyperpigmentation and secondary scarring, were documented at the final follow-up visit. The overall duration of subjective downtime, defined as the time during which the patient felt that treatment meaningfully affected their quality of life, was also recorded after each treatment session.
Three-dimensional (3D) image analysis
To provide supportive data for the objective evaluation of treatment efficacy, a 3D camera and software (Antera 3D® CS, Miravex, Dublin, Ireland) were used for 4 patients. Antera 3D® captures high-resolution images and provides images in 3 dimensions using optical methods and complex mathematical algorithms, which makes it possible to extract and quantify data on the 3-dimensional shape of the skin. The depressed volume of atrophic scars, mean volume of skin pores, and skin surface roughness at the selected area were objectively measured at each visit.
Statistical analysis
Baseline characteristics were presented as the mean ± standard deviation (SD) and range for continuous variables, and as number and percentage for categorical variables. Baseline data and IGA were analysed using the Wilcoxon signed-rank test to compare between treatment sides. Linear mixed effect models were used to analyse ECCA scores, atrophic scar volume, mean pore volume, and skin surface roughness. The duration of downtime was evaluated using a generalized linear mixed model with generalized Poisson family. Post-treatment pain, erythema, oedema, and dryness were assessed using cumulative link mixed models. The McNemar test was used to compare the occurrence of post-treatment hyperpigmentation and scar formation between treatment sides. A p-value less than 0.05 was considered statistically significant. All statistical analyses were performed using R version 3.6.2 (R Foundation for Statistical Computing, Vienna, Austria). Further details are provided in Appendix S1.
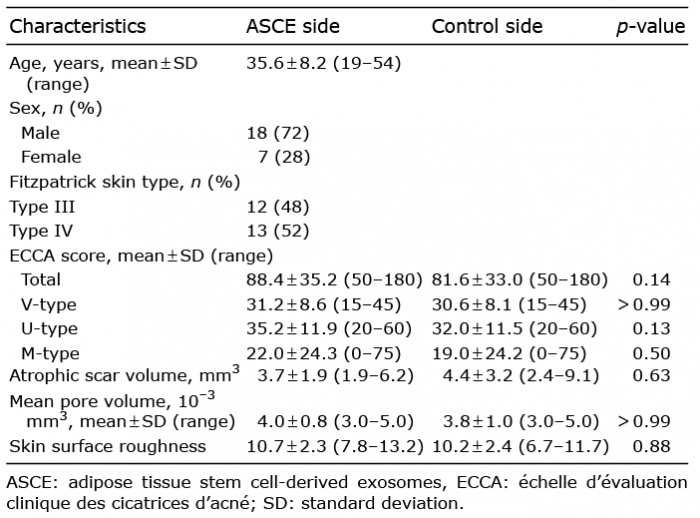
A total of 25 enrolled patients completed the study. Baseline patient characteristics are summarized in Table I. There were no significant differences in total ECCA score or scores of the 3 major subtypes (V-, U-, and M-shaped) of atrophic scars at baseline between the ASCE-treated and control sides.
Table I. Baseline characteristics of participants
Characterization of exosomes applied in clinical trial
ASCE were analysed with an NTA instrument to measure particle size distribution and concentration. As shown in Fig. 1A, the mode size was approximately 117.4 nm, and the concentration was 3.26×1011 particles/ml. Cryo-transmission electron microscopy analysis revealed ASCE that were spheres of 30–200 nm diameter and exhibited a clear lipid bilayer structure (Fig. 1B). Next, ASCE were stained with antibodies against well-established exosome surface markers (CD9, CD63, and CD81) and were analysed using bead-based flow cytometry. As shown in Fig. 1C, ASCE were positively stained with all 3 markers. The purity of the ASCE was determined by the absence of calnexin and cytochrome C, negative markers of exosomes. In line with the literature, ASCE exhibited low levels of calnexin and cytochrome C (Fig. 1D). To evaluate biological functions of ASCE in target cells, 4 in vitro potency assays were performed. As shown in Appendix S1; SFig. 1, ASCE increased collagen synthesis, cell migration and proliferation in human dermal fibroblast and decreased inflammatory cytokine level in murine macrophage. These results indicate that ASCE isolated by ExoSCRT™ technology exhibit typical characteristics of exosomes. Purified ASCE were used in ASCE solutions, and in vitro data were described in Appendix S1.
Fig. 1. Characterization of adipose tissue stem cell-derived exosomes (ASCE). (A) Representative plot of particle concentration and size distribution of ASCE, as measured by nanoparticle tracking analysis (NTA). (B) Cryo-transmission electron microscopy image of ASCE. Scale bar: 200 nm. (C) Signal intensities of exosome surface markers. ASCE were analysed using flow cytometry after staining with anti-CD9, -CD63, and -CD81 antibodies. (D) Levels of exosome exclusionary markers, calnexin and cytochrome C, in ASCE compared with cell lysate. Data are presented as the mean ± standard deviation (SD) of 3 independent experiments.
Evaluation of scar improvement
A significant reduction in ECCA score from baseline was observed on the ASCE side beginning at the first post-treatment visit and on the control side from the second post-treatment visit (Fig. 2A). The difference in percent reduction of ECCA score between the two regimens was not significant at the first post-treatment visit, but became significant at the second post-treatment visit. At the final follow-up visit, the ECCA score was reduced by 32.5% (95% confidence interval [CI]: 24.8–40.2%) from baseline on the side treated with ASCE, which was significantly greater than the reduction of 19.9% (95% CI: 12.2–27.6%) on the control side (p < 0.01).
Mean reductions in ECCA score were also analysed for each subtype (V-, U-, and M-shaped) of atrophic scar (Fig. 2B–D). For both V- and U-shaped scars, significant decreases in ECCA score from baseline were observed on both sides, but the differences in the reduction of ECCA score between the two regimens were not statistically significant at the final follow-up visit. For M-shaped scars, the ECCA score was significantly decreased compared with baseline on both sides, and ASCE-treated sides showed a significantly greater improvement than the control side at the final follow-up visit.
Fig. 2. Evaluation of scar improvement based on échelle d’évaluation clinique des cicatrices d’acné (ECCA) scores. (A) Mean percentage changes in total ECCA scores and mean changes in ECCA scores for (B) V-shaped (icepick), (C) U-shaped (boxcar), and (D) M-shaped (rolling) atrophic scars on the adipose tissue stem cell-derived exosomes (ASCE) and control sides. *p < 0.05 compared with baseline; ?p < 0.05 between the 2 sides. Error bars indicate standard errors. PT: post-treatment.
The IGA scores demonstrated comparable patterns to the ECCA evaluations. The grades 0, 1, 2, 3, and 4 were observed in 1, 8, 10, 5, and 1 facial sides treated with ASCE, respectively, and in 2, 11, 11, 1, and 0 facial sides with control, respectively. The ASCE-treated facial side demonstrated superior improvement based on IGA score compared with the control side after 3 sessions of each treatment (p = 0.02). Sixteen out of 25 facial sides achieved grade 2 or more improvements on the ASCE side, compared with 12 of the control-treated sides. Fig. 3 shows a representative case before and after each application.
Fig. 3. Clinical photographs of the adipose tissue stem cell-derived exosomes (ASCE) and control sides at baseline and 6 weeks after 3 treatment sessions in a 30-year-old male.
Three-dimensional image analysis
The depressed volume of atrophic scars, mean volume of skin pores, and skin surface roughness were objectively measured using an Antera 3D® CS at baseline and post-treatment visits (Fig. 4). At the final follow-up visit, all of atrophic scar volume, mean pore volume, and skin surface roughness were significantly decreased from baseline on the ASCE side. In contrast, no significant decreases were observed on the control side.
Fig. 4. Three-dimensional image analyses for atrophic scar, enlarged skin pore, and skin surface roughness using Antera 3D® CS. (A–D) Clinical photographs and analysed images of the adipose tissue stem cell-derived exosomes (ASCE) and control sides at baseline and at the final follow-up visit. (B) The depths of atrophic scars are shown as colours (white<yellow<green<blue<purple). (C) The depths of enlarged skin pores are shown as colours (white<yellow<orange<green<blue). (D) The vertical deviations of the skin surface are shown as colours: [downward] purple<blue<green<white <yellow<red [upward]. Mean percent changes in (E) atrophic scar volume, (F) mean pore volume, and (G) skin surface roughness on the ASCE and control sides. *p < 0.05 compared with baseline. Error bars indicate standard errors. PT: post-treatment.
Adverse effects
Various treatment-related side-effects, including post-treatment pain, erythema, oedema, and dryness, were experienced on both ASCE and control sides (Figs 5 and 6), but they were nearly resolved within 5 days. The severity of erythema during the first post-treatment week was significantly lower on the exosome side than on the control side (p = 0.03). Post-treatment pain, oedema, and dryness also tended to be milder on the exosome side, although not statistically significant. The mean duration of downtime was shorter on the ASCE side compared with the control side (4.1 (95% CI 3.5–4.8) days vs 4.3 (95% CI 3.7–5.1) days, p = 0.03). Two patients reported mild hyperpigmentation on the control side; one patient reported mild hyperpigmentation on the ASCE side (p = 0.32). No patient healed with scar formation or other permanent events.
Fig. 5. Evaluation of: (A) pain, (B) erythema, (C) oedema, and (D) dryness on both adipose tissue stem cell-derived exosomes (ASCE) and control sides for post-treatment 7 days.
Fig. 6. Clinical photographs of the adipose tissue stem cell-derived exosomes (ASCE) and control sides for post-treatment 4 days in a 31-year-old male.
Atrophic acne scars are associated with an incomplete recovery of the dermal matrix damaged by chronic inflammation (22, 23). Therefore, most fractional resurfacing devices work by depositing a pixilated pattern of microscopic wounds surrounded by healthy tissue, which are then repaired by the natural recovery process (24). However, the regenerative capability of these controlled wounds may be limited in many cases, frequently leading to delayed healing with unsatisfactory results. This specific period is also associated with various treatment-related complications, necessitating a clinical adjuvant application of soothing biological materials (25–27).
This split-face study demonstrates the clinical benefits of the postoperative application of ASCE for acne scars. To the best of our knowledge, this is the first study to use ASCE for human skin wound repair. The ASCE-treated side experienced significantly better improvement. Although both sides demonstrated steady improvement during treatment sessions, a significant difference between them was observed after completing the second session. Compared with other available adjuvant biological materials, the degree of additional improvement and relatively earlier onset time of ASCE were satisfactory (2, 4). The relative lack of efficacy of V- and U-subtypes suggests that the co-application of physical treatments including dot peeling or subcision is still needed with ASCE. From a safety perspective, ASCE-treated sides exhibited reduced post-procedural erythema and a shorter downtime.
When FCL is administered to the skin, the epidermis penetrated by the beams is instantly vaporized in microcolumns reaching down into the dermis; these columns are called microablative columns (MACs) (28). MACs begin regeneration within several hours and complete re-epithelization is usually achieved within 2–3 days. During recovery, there is an accumulation of materials involved in wound remodelling, such as heat shock protein, procollagen, and dermal elastin (29). During this process, the temporarily formed vertical channel bypassing epidermal skin barriers allows an effective passage of microparticles, such as exosomes utilized in this study, into dermal tissues (30).
A mechanistic rationale for combining FCL and ASCE in acne scar treatment is the ability of ASCE to induce rapid healing after FCL ablation by supplying multiple anti-inflammatory and regenerative growth factors (31–35). Like ASCs, ASCE are also considered to optimize characteristics of fibroblasts, such as promoting the migration, proliferation, and collagen synthesis of fibroblasts (36–38), thereby accelerating wound healing of soft tissue with extracellular matrix remodelling (39, 40). ASCE also promote scarless cutaneous wound repair by regulating the ratios of collagen type III:type I, transforming growth factor (TGF)-β3:TGF-β1 and matrix metalloproteinase 3:tissue inhibitor of metalloproteinases-1, and by regulating fibroblast differentiation to mitigate scar formation (38). There is accumulating evidence that several signalling pathways related to skin regeneration and wound healing are stimulated by ASCE (34). A recent paper also demonstrates that ASCE can increase the de novo synthesis of ceramides to rebuild skin barrier (35). Compared with other biological materials, including platelet-rich plasma and stem cell-conditioned medium, ASCE have potential advantages as they are mass-produced, sterilized by filtration, and have a longer shelf-life.
As the exosomes used in this study were isolated from CM of ASCs from a healthy donor, there may be consideration of possible inter-individual variation. To make consistent functionality of exosomes, standardized quality control (QC) for cells and exosomes was applied. Various tests such as phenotype (surface markers, differentiation potential, etc.) and growth kinetics, for stem cell itself were performed to ensure the quality of cells as the source of exosomes (41), as previously recommended (42–44). More importantly, QC for exosomes were also performed to compare the functional activities of ASCE according to the recommendation of the Korean Ministry of Food and Drug Safety (45) and the International Society for Extracellular Vesicles (46). Through the QC, in vitro potency assays have shown consistent results with low variations.
Furthermore, no specific immunity concerns have been raised regarding MSC-derived exosomes. Like their cellular source, MSC exosomes are hypo-immunogenic (47). They are negative for major histocompatibility complex (MHC) class I and II, and co-stimulatory molecules, such as B7-1 (CD80), B7-2 (CD86) and CD40 (48, 49). ASCE, used in the present study, were also negative for the human leukocyte antigens (HLA), the human MHCs, such as HLA-ABC and HLA-DRDPDQ (35, 41). In addition, the immunologic safety of MSC exosomes has been confirmed through various in vitro and in vivo studies (50–54).
There were some limitations to this study. First, all enrolled patients had a similar ethnic background. Secondly, further studies pursuing optimal ASCE application regimens are necessary.
In conclusion, treatment with ASCE afforded more favourable responses, a shorter recovery time, and fewer side-effects when utilized in combination with FCL for acne scarring. Therefore, co-treatment with this novel material with resurfacing devices may provide synergistic effects on both efficacy and safety for atrophic scar treatments.
Exosome and control solutions used in this study were manufactured, purified and provided by ExoCoBio Inc. (Seoul, Korea).
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize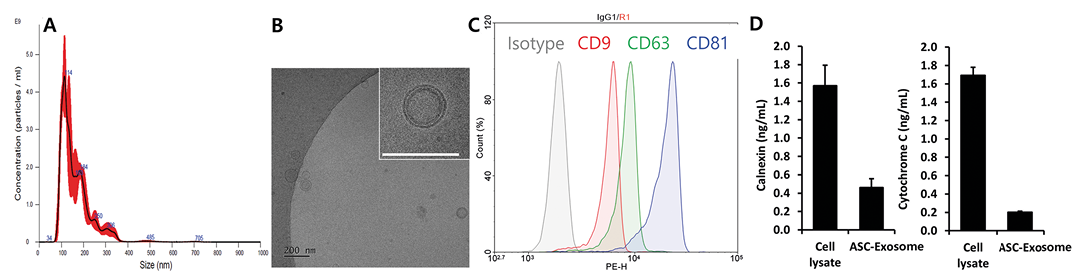 Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize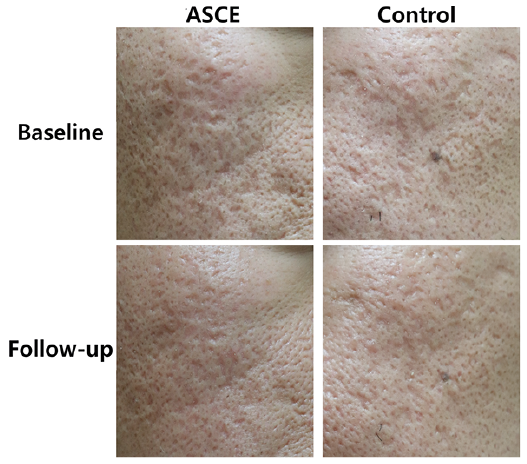 Click to show fullsize
Click to show fullsize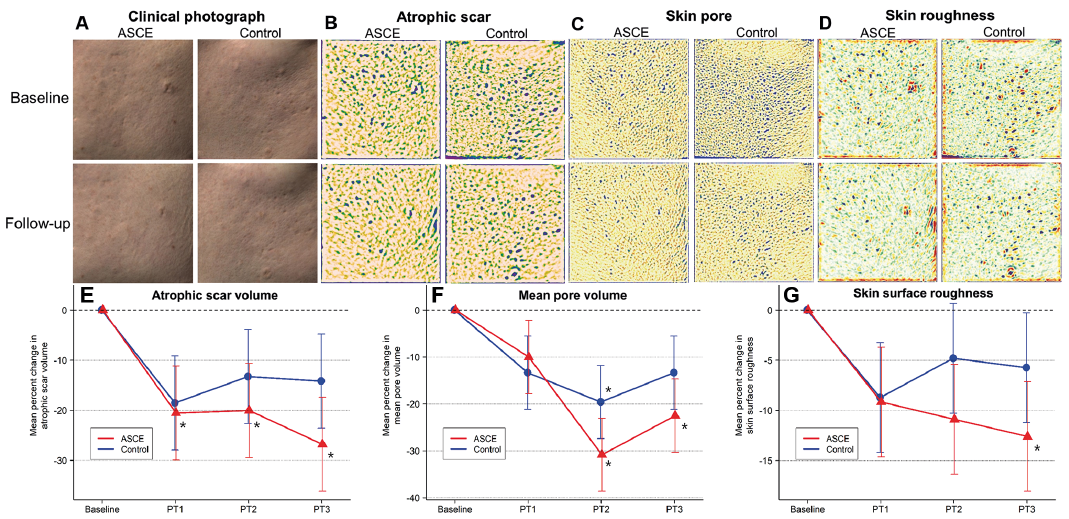 Click to show fullsize
Click to show fullsize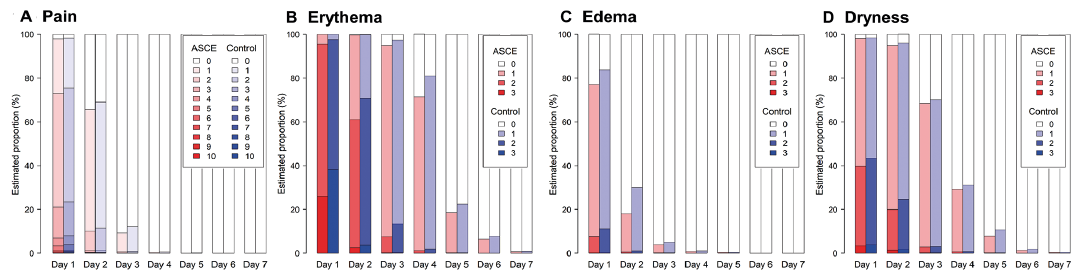 Click to show fullsize
Click to show fullsize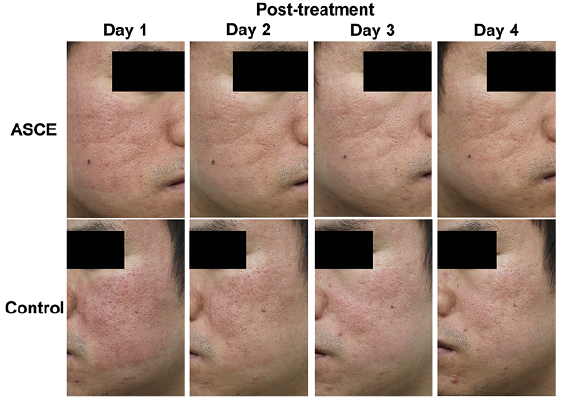 Click to show fullsize
Click to show fullsize