


Department of Dermatology and Venereal Diseases, University Medical Centre Maribor, Ljubljanska ulica 5, SI-2000 Maribor, Slovenia.*E-mail: katarina.trcko@gmail.com
A 55-year-old man presented to our department with a 5-month history of skin lesions on his trunk and extremities that were asymptomatic. His past medical history was unremarkable. Clinical examination revealed multiple erythematous papules, nodules and plaques with ulcerations and haemorrhagic crusts symmetrically distributed on extensor surfaces of the extremities, trunk, soles and lips (Fig. 1). He denied any sexual contact. The patient was afebrile. No enlarged lymph nodes were found. Swab cultures showed no growth and routine blood tests were normal. Histopathology revealed necrotic epidermis with crust rich in neutrophils and a diffuse dense infiltrate of lymphocytes, histiocytes, many epithelioid granulomas, some giant cells, rare plasma cells and neutrophils extending throughout the entire dermis (Fig. 2).
What is your diagnosis? See next page for answer.
Fig. 1. Clinical features. (a) Symmetrically distributed lesions on extensor surfaces of upper extremities and scarcely any on the anterior part of the trunk. (b) Close-up photograph of the left forearm shows erythematous-violaceous papules, nodules and plaques, some of which are covered by brownish yellow and haemorrhagic crusts, surrounded by an erythematous halo.
Fig. 2. Histopathology of biopsy specimen from nodular lesion on the upper extremity shows necrotic epidermis with crust rich in neutrophils and a diffuse dense infiltrate of lymphocytes, histiocytes, many epithelioid granulomas, some giant cells, rare plasma cells and neutrophils extending throughout the entire dermis. (a) Haematoxylin and eosin (H&E), 100×; (b) H&E, 200×.
Acta Derm Venereol 2020; 100: adv00304.
Diagnosis: Ulceronodular syphilis
Since the pathology indicated a possible diagnosis of secondary syphilis, serological tests for sexually transmitted diseases were performed and showed markedly elevated Venereal Diseases Research Laboratory (VDRL) test with a titre of 1:512 and a positive Treponema pallidum haemogglutination test (TPHA). Screening for human immunodeficiency virus (HIV) was negative. These results were sufficient to confirm a diagnosis of ulceronodular secondary syphilis. The patient was treated with 2.4 million units of benzathine penicillin, given intramuscularly, with dramatic improvement. Follow-up after 6 months showed no recurrence of syphilis, with non-reactive VDRL and positive TPHA.
Ulceronodular syphilis is a rare and atypical variant of secondary syphilis. It is also known as malignant syphilis (MS) or lues maligna because of its exuberant clinical appearance and concomitant systemic symptoms (1, 2). It usually develops 6 weeks to one year after primary infection. MS occurs mainly in immunocompromised, especially HIV-infected, patients (2). Our patient was otherwise healthy and HIV-uninfected. Several cases of MS have already been described in immunocompetent, HIV-negative individuals (2–4). The pathogenesis of MS is unknown. Theories indicate that it can be the result of immunosuppression, exaggerated immune response in the otherwise normal host, or infection by more virulent strains of Treponema pallidum (3, 4).
MS clinically presents as symmetrically distributed erythematous-violaceous papules, nodules and plaques that can evolve into ulcers, occasionally with rupioid crusts (1, 2). Lesions are mostly asymptomatic, particularly located on the upper parts of the trunk and extremities, rarely on palms and soles. Sometimes patients experience prodromal constitutional symptoms, which were absent in the case described here (2, 3).
The differential diagnosis of MS includes cutaneous lymphoma, sarcoidosis, tuberculosis, deep mycoses, leprosy, Kaposi’s sarcoma, pyoderma gangrenosum, vasculitis and tertiary syphilis. Fisher’s diagnostic criteria for MS are: compatible morphology of the lesions and histology, high serology titres for syphilis, Jarisch-Herxheimer reaction (JHR) following treatment, and excellent response to therapy (2). MS shares histological features with other forms of secondary syphilis, typically characterized by endarteritis, a superficial and deep perivascular plasma cell infiltrate, interface dermatitis, and epidermal necrosis. Histiocytes, giant cells, neutrophils and granulomas may also be seen (1, 3, 5).
The current patient met all of the above criteria, except for the development of JHR, the absence of which has been mentioned in some other case reports (6). According to a study by Lee et al., the incidence of JHR after penicillin therapy is higher in HIV-infected patients than HIV-negative ones; 34.6% vs 25.2%. However, the difference was not statistically significant (7).
Secondary syphilis is known as “the great imitator” because of diverse cutaneous manifestations. MS is its rare variant, especially in healthy, immunocompetent patients, and it should be considered in differential diagnosis of ulceronodular lesions even in the absence of systemic symptoms. Treatment with a single dose of intramuscular penicillin is sufficient and results in a rapid clinical improvement.


 Click to show fullsize
Click to show fullsize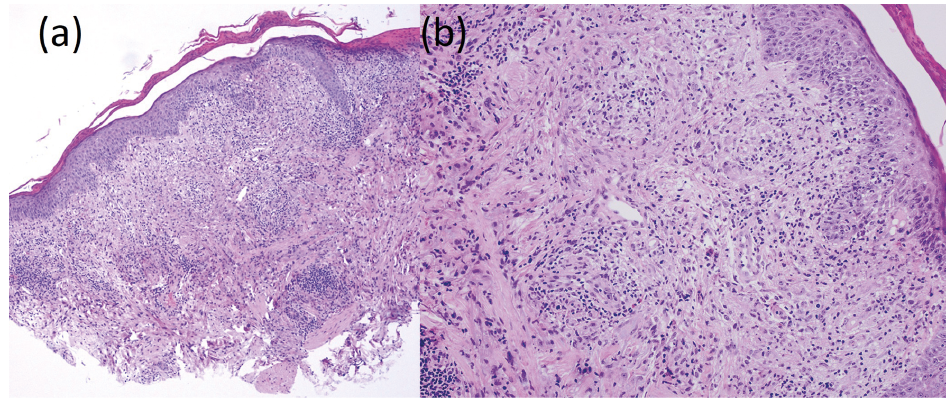 Click to show fullsize
Click to show fullsize