


1Department of Dermatology, 2Research Center of Big Data and Meta-analysis, Wan Fang Hospital, Taipei Medical University, and 3Department of Dermatology, School of Medicine, College of Medicine, Taipei Medical University, Taipei, Taiwan
#These authors contributed equally to the study as first authors.
The association between rosacea and cardiovascular disease remains controversial. A systematic review and meta-analysis of the literature, from inception to 15 February 2020, was performed to compare cardiovascular risk and comorbidities in individuals with and without rosacea. Twelve studies, involving 40,752 patients with rosacea, were included. Compared with controls, patients with rosacea had higher systolic blood pressure (standardized mean difference (SMD) 0.293, 95% confidence interval (CI) 0.054–0.532), diastolic blood pressure (SMD 0.309, 95% CI 0.003–0.615), total cholesterol (SMD 1.147, 95% CI 0.309–1.984), low-density lipoprotein (SMD 0.792, 95% CI 0.174–1.409), C-reactive protein (SMD 0.26, 95% CI 0.099–0.421), greater epicardial fat thickness (SMD 1.945, 95% CI 1.595–2.296), and higher incidence of hypertension (odds ratio (OR) 1.204, 95% CI 1.097–1.332) and insulin resistance (OR 2.338, 95% CI 1.187–4.605). This study reveals that patients with rosacea are predisposed to increased subclinical cardiovascular risk.
Key words: cardiovascular disease; dyslipidaemia; hypertension; meta-analysis; risk factor; rosacea; systematic review.
Accepted Oct 15, 2020; Epub ahead of print Oct 19, 2020
Acta Derm Venereol 2020; 100: adv00300.
doi: 10.2340/00015555-3668
Corr: Yu-Chen Huang, Department of Dermatology, Wan Fang Hospital, Taipei Medical University, 111, Hsing-Long Road Sec. 3, Wenshan District, Taipei City 116, Taiwan. E-mail: dhist2002@yahoo.com.tw
This study reveals that patients with rosacea are predisposed to increased subclinical cardiovascular risk, but there is insufficient evidence to demonstrate a higher incidence of overt cardiovascular comorbidities. Clinicians are advised to examine patients with rosacea for cardiovascular risk and comorbidities and to offer advice on lifestyle modifications.
Rosacea is a chronic disease that occurs frequently in women and individuals with fair skin (1). The clinical features of rosacea include centrofacial erythema, flushing, telangiectasia, papules, pustules, and phymatous changes (1). Ocular involvement may also occur, characterized by burning, stinging sensation, conjunctival injection, and lid margin telangiectasia (1). The exact pathophysiology of rosacea remains unclear, but it is believed that chronic inflammation and vascular hyper-reactivity are the major contributing factors (2–4). Chronic inflammation also plays a pivotal role in the pathogenesis of atherosclerosis, which reflects the increased risk of cardiovascular (CV) diseases in various chronic inflammatory disorders, such as psoriasis (5–7). Since rosacea is also a chronic inflammatory disease, an important question is whether rosacea is a localized cutaneous disease or a disease with systemic ramifications. This question is important because, if systemic inflammation does occur in patients with rosacea, more aggressive monitoring and interventions for systemic comorbidities in patients with rosacea may be warranted.
Several observational studies have investigated the association between rosacea and various CV diseases, such as coronary artery disease (CAD), diabetes mellitus (DM), dyslipidaemia, and hypertension (HTN) (8, 9). However, to date, the results of these studies are inconclusive. The aim of this study was to examine the CV risk and comorbidities in patients with rosacea in an evidence-based manner, by conducting a systematic review and meta-analysis.
The methodology of this study complied with the recommendations of the Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) statement.
The study sought to examine CV risk in patients with rosacea in comparison with controls. The primary outcomes were risk factors for CV diseases and incidence of CV comorbidities in patients with rosacea compared with controls.
Data sources and search strategy
Databases (PubMed, Cochrane Library, and Embase) were searched from inception to 15 February 2020. The final date of searching was 10 March 2020. The search focused exclusively on clinical studies involving humans, and the results were reported without any language limit. The literature search was initially performed with more general terms. After that, based on the search results, more specific terms (e.g. epicardial fat thickness) were used to search the databases again. Keywords used in the literature searches were: “rosacea” combined with “cardiovascular disease”, “cardiovascular risk”, “coronary artery disease”, “myocardial infarction”, “heart failure”, “peripheral arterial occlusive disease”, “hypertension”, “diabetes mellitus”, “dyslipidemia”, “stroke”, “obesity”, “insulin resistance”, “metabolic syndrome”, “epicardial fat thickness” and “carotid intima media thickness”. Reference lists from the screened articles were reviewed in order to avoid missing any studies.
Eligibility criteria and study selection
Studies comparing (i) the risk factors for CV diseases and (ii) the incidence of CV comorbidities between patients with rosacea and controls were included in the analysis. Eligible case-control and cohort studies (both prospective and retrospective, population-based and institution-based) were included. Review articles, case reports, case series, and conference abstracts were excluded. Case-control and cohort studies were included and case reports and case series excluded because we aimed to include studies with a higher level of evidence. Duplicated studies were excluded, but partially overlapping studies were included in the systematic review. Two investigators (TYT and YYC) independently screened the titles and the abstract of the articles. The full texts of articles reporting relevant data were assessed to determine eligibility. Any disagreement was resolved through discussion with a third investigator (YCH).
Quality assessment
The methodological quality of the included articles was evaluated based on an adapted version of the Newcastle–Ottawa Scale for cohort studies and the adapted version for cross-sectional studies, with a maximum score of 9 points for cohort studies and 7 points for cross-sectional studies. Quality assessment was performed independently (TYT and YYC) and any disagreement was resolved by the third investigator (YCH).
Data extraction
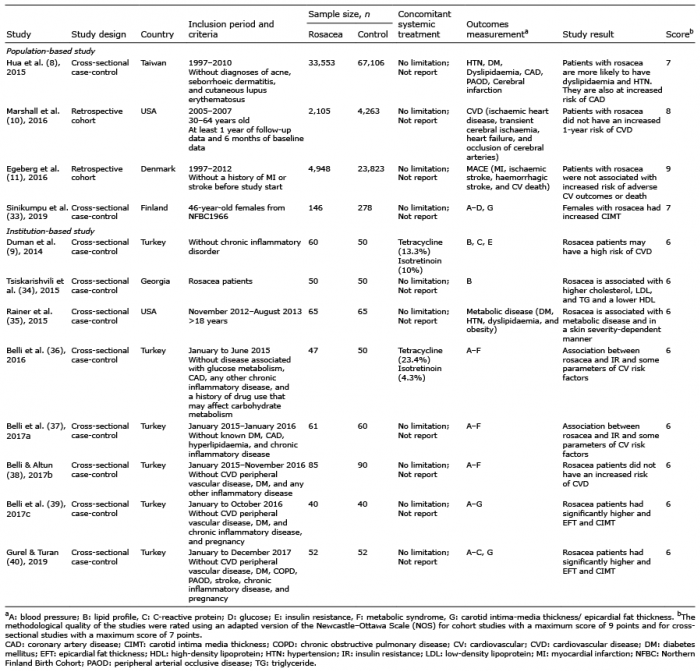
Two reviewers independently extracted and collected the data in a tabular form. The extracted data included: country, study type, inclusion criteria, sample size, study results, and quality scores (Table I). The age, sex, and laboratory data for patients with rosacea and the controls were also extracted. Detailed data for the studies regarding the association with CV comorbidities are shown in Table II, which included the crude and adjusted odds ratio (OR)/incidence rate ratio (IRR) and the adjusted variables.
Table I. Summary of included studies
Table II. Detailed data and results of studies with incidence of cardiovascular comorbidities
Data analysis
A pooled estimate of the laboratory and image examinations regarding the risk of CV diseases was performed for patients with rosacea and compared with that of controls. In addition, a pooled estimation was performed, comparing the incidence of CV comorbidities between patients with rosacea and controls. Pooled analyses were only performed for at least 2 studies, reporting the results in a similar form. Analyses of continuous data were performed using standardized mean difference (SMD) with 95% confidence interval (CI), while those of dichotomous data were conducted using OR with 95% CI. Adjusted estimates were chosen instead of raw ones, if they were provided in included studies. Heterogeneity testing was conducted by using the I square test. A random effects model was used for all analyses because of potential heterogeneity. Funnel plots and tests for publication bias (Egger’s test and Begg and Mazumdar test) were performed. The software used for statistical analyses was Comprehensive Meta-Analysis Version 3 software (Biostat Inc., Englewood, NJ, USA).
Search results and trial characteristics
Of the 232 studies screened, 12 studies involving 40,752 patients with rosacea met the inclusion criteria (Fig. 1). Two of the 12 studies were cohort studies (both population- based studies) and the remaining 10 studies were cross-sectional case-control studies (2 population-based studies and 8 institution-based studies). Four of the 12 studies reported the incidence of CV comorbidities in patients with rosacea, and the other 8 studies described the laboratory and image data related to CV risk factors in patients with rosacea. Four cross-sectional studies were performed at the same medical centre and the study periods showed an overlap. Only 2 of the 4 studies were considered for the meta-analysis. Table I summarizes the characteristics of the studies, with quality scores ranging from 6 to 9. Most cross-sectional studies lost one point of score from the selection part owing to lack of description for the non-respondents.
Fig. 1. Flow diagram for study identification.
Risk factors for cardiovascular diseases
The common risk factors for CV diseases measured in the included studies were blood pressure, lipid profile, fasting blood glucose levels, C-reactive protein (CRP) levels, carotid intima media thickness (CIMT), and epicardial fat thickness (EFT). Dyslipidaemia, HTN, insulin resistance (IR), metabolic syndrome, and DM were also defined as risk factors for CV diseases. All these data were summarized in Table III and aggregated to compare the risk factors for CV diseases in patients with rosacea with those in controls.
Table III. Detailed data and results of studies with outcomes of physical examination and laboratory data
Cardiovascular comorbidities
The CV comorbidities included CAD, heart failure, stroke, peripheral arterial occlusive disease, and CV death (Table II). One cohort study showed that the one-year CV risk in patients with rosacea was similar to that in the controls after adjustment for age, sex, and comorbidities (DM and Charlson Comorbidity Index) (OR 0.894, 95% CI 0.732–1.091) (10). Another cohort study with a long-term follow-up also showed no difference in the incidence of major adverse CV events after adjustment for comorbidities, medication, and socioeconomic status (IRR 0.99, 95% CI 0.86–1.15) (11). However, one cross-sectional study showed that the risk of CAD in patients with rosacea was significantly higher than that in controls, even after adjustment for DM, HTN, and dyslipidaemia (OR 1.20, 95% CI 1.14–1.26) (8). No pooled analysis was performed, owing to differences in study designs and the heterogeneous definition of CV outcomes.
Statistical analysis
The results of the meta-analyses are shown in Figs 2 and 3. Patients with rosacea had higher systolic blood pressure (SMD 0.293, 95% CI 0.054–0.532), diastolic blood pressure (SMD 0.309, 95% CI 0.003–0.615), total cholesterol levels (SMD 1.147, 95% CI 0.309–1.984), low-density lipoprotein levels (SMD 0.792, 95% CI 0.174–1.409), and CRP levels (SMD 0.26, 95% CI 0.099–0.421) in comparison with controls. The CIMT was similar between patients with rosacea and controls (SMD 1.058, 95% CI −0.044–2.161), but the EFT in patients with rosacea was higher than that in controls (SMD 1.945, 95% CI 1.595–2.296). Pooled analyses showed that the incidence of HTN (OR 1.204, 95% CI 1.097–1.332) and IR (OR 2.338, 95% CI 1.187–4.605) in patients with rosacea was significantly higher than that in controls, but the incidence of metabolic syndrome and DM was similar in the 2 groups. Tests for publication bias were not performed because only a limited number of studies were included in the meta-analysis.
Fig. 2. Forest plots. The forest plots showed the pooled estimates of cardiovascular risk factors in patients with rosacea in comparison with controls. Compared with controls, patients with rosacea had higher systolic blood pressure, diastolic blood pressure, total cholesterol, low-density lipoprotein, and C-reactive protein. Carotid intima media thickness was similar between patients with rosacea and controls, but epicardial fat thickness was greater in rosacea patients than in controls. CI: confidence interval.
Fig. 3. Forest plots. Pooled analyses showed the incidence of hypertension and insulin resistance was significantly higher in patients with rosacea than in controls, but the incidence of metabolic syndrome and diabetes mellitus was similar in the 2 groups. CI: confidence interval.
This meta-analysis reveals that patients with rosacea have significant risk factors for CV diseases, including higher systolic blood pressure, diastolic blood pressure, total cholesterol levels, low-density lipoprotein levels, CRP levels, and EFT. Moreover, this study showed that the incidence of IR in patients with rosacea was significantly higher than in controls, but the incidence of DM and metabolic syndrome was not increased in patients with rosacea compared with that in controls, thereby suggesting a subclinical derangement in patients with rosacea.
No meta-analysis of CV comorbidities was performed, due to substantial study heterogeneity and a limited number of eligible studies. The population-based cross-sectional study conducted by Hua et al. (8) showed that patients with rosacea had a higher risk of CAD than controls; in contrast, the cohort study conducted by Egeberg et al. (11) revealed that patients with rosacea had a similar risk of myocardial infarction as controls. However, in the cross-sectional study, the definition of CAD did not include the International Classification of Disease-9 (ICD-9) code 410 (acute myocardial infarction), which is the most severe form of CAD (8). This might explain the different results between the 2 studies. Both studies concluded that patients with rosacea did not have a higher risk of ischaemic stroke than controls (8, 11). The current evidence is not sufficient to demonstrate that patients with rosacea have higher incidence of CV comorbidities, such as myocardial infarction and stroke.
The mechanisms underlying the susceptibility of patients with rosacea to increased CV risk may be attributable to the common pathological pathways in these diseases. Patients with rosacea have an increased level of cathelicidin, an antimicrobial peptide, in their skin (2, 3). Besides the levels of cathelicidin, the forms of cathelicidin in patients with rosacea are different from those in healthy individuals (2). Cathelicidin enhances angiogenesis, leukocyte chemotaxis, and the expression of extracellular matrix components (2). Cathelicidin is processed by serine protease kallikrein 5, which is expressed extensively in the epidermis of patients with rosacea (3, 12). Recent studies have shown increased levels of cathelicidin in atherosclerotic plaques and correlations between the genetic expression of cathelicidin and CV risk factors (13–15). Cathelicidin has also been reported to promote IR in obese individuals (16). Furthermore, serine proteases are also involved in the pathogenesis of atherosclerosis (17). In addition, patients with rosacea are reported to have a decreased activity of paraoxone-1 (PON1), an antioxidant enzyme, and increased oxidative stress (18). Decreased activity of PON1 has also been shown in patients with dyslipidaemia, HTN, and DM (19, 20). Increased oxidative stress is widely believed to be a pivotal mechanism in atherosclerosis (21)
Tetracyclines, which are commonly used for treating rosacea, have not only antimicrobial effects, but also anti-inflammatory properties, and they could potentially be used to treat both cutaneous and systemic inflammation (22, 23). Tetracyclines inhibit matrix metalloproteinases (MMPs), which are important enzymes in the vascular pathophysiology of both rosacea and atherosclerosis (22, 24). A large cohort study showed that patients with rosacea receiving tetracyclines (with variable dosage and duration) had a decreased risk of developing vascular diseases (25). Axisa et al. (26) showed, in a randomized controlled trial (RCT), that doxycycline (200 mg daily for 2–8 weeks) decreased the expression of MMP-1 in atherosclerotic carotid plaques In multiple RCTs, sub-antimicrobial doses of doxycycline therapy (20 mg twice daily for 3 months in Koppikar et al. (27), 6 months in Brown et al. (28) and 2 years in Payne et al. (29)) have also been shown to reduce the levels of CRP and MMP-9. The beneficial effects of treatment with tetracyclines on both cutaneous and systemic inflammation corroborate the hypothesis that rosacea and CV diseases share common pathophysiological pathways, and these effects may serve to explain the relatively subclinical CV derangements in patients with rosacea, as shown in the current study.
Study limitations
A major limitation of the current study is that only a few eligible studies were included. However, some analyses included population-based studies, which had large sample sizes of study subjects, thereby compensating more or less the paucity of existing eligible studies. Of note, many of the included studies were conducted in Turkey, which may lead to bias when the research findings are generalized to a broader population. Ethnicity and genetics may play critical roles in the risk of rosacea and cardiovascular diseases. Rosacea is found to be more prevalent in people of Celtic and Northern European origin and is less commonly seen in people with darker skin, possibly due to masking of symptoms by darker skin pigmentation or genetic differences (30). In addition, ethnic differences in cardiovascular risk could lead to potential bias. For example, Chaturvedi revealed that South Asians have higher risk of insulin resistance and heart diseases compared with Europeans. (31). Onat (32) reported that mortality from coronary heart disease in Turkey was among the highest in selected European countries. Therefore, inclusion of a high proportion of Turkish studies could potentially be a major source of bias. However, the sample sizes of these Turkish studies are relatively small compared with the large sample sizes of other population-based studies conducted in other regions of the world. Another limitation is that the use of systemic medications, such as tetracycline and isotretinoin, could not be adjusted in our analysis, because most included studies did not provide such details (Table I). The use of tetracycline may lead to underestimation, while the use of isotretinoin may lead to overestimation, of some parameters in the current analysis. However, the duration of tetracycline treatment for rosacea is often short, and isotretinoin is infrequently used to treat rosacea. Therefore, the potential biases caused by the use of these medications might not be marked. Future studies are encouraged to take this factor into consideration. Lastly, some of the analyses were limited by substantial heterogeneity, which might result from differences in age, ethnicity, types and severity of rosacea among included studies. Unfortunately, subgroup and meta-regression analysis could not be performed because of insufficient data reported in the included studies.
Conclusion
The current study revealed that patients with rosacea are predisposed to increased CV risk, such as HTN, dyslipidaemia, IR, and high EFT. However, patients with rosacea do not have a higher incidence of overt CV comorbidities, such as myocardial infarction and stroke, although this incidence may have been underestimated due to the common use of tetracyclines. Clinicians are advised to examine patients with rosacea for CV risk and comorbidities. Patients should also be given advice regarding lifestyle modifications. Future studies should investigate the link between cutaneous and internal inflammation and examine the potential benefits of sub-antimicrobial doses of tetracyclines as primary prevention for CV diseases in patients with rosacea.
The authors thank Taipei Medical University and Wan Fang Hospital, Taipei Medical University for financial support under grant number 108TMU-WFH-02, which made this study possible.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize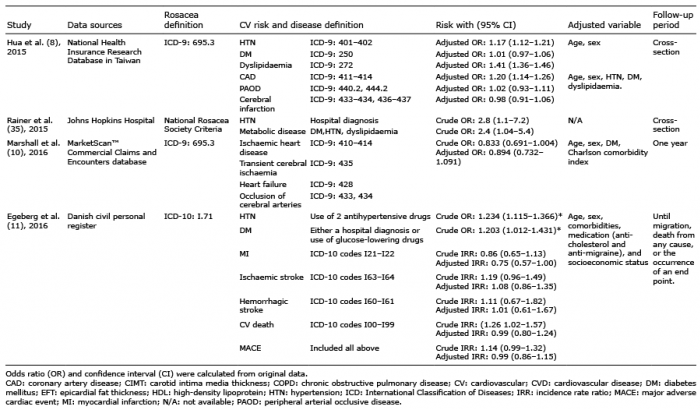 Click to show fullsize
Click to show fullsize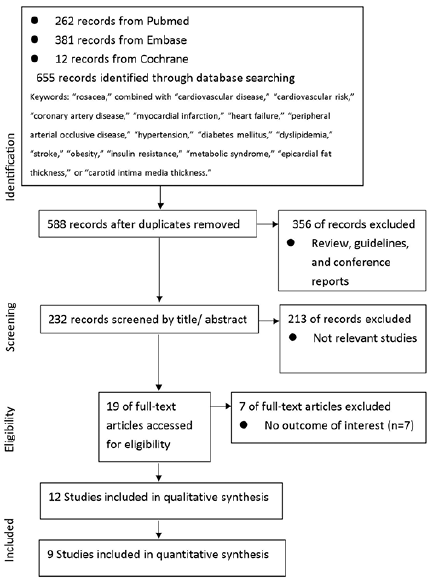 Click to show fullsize
Click to show fullsize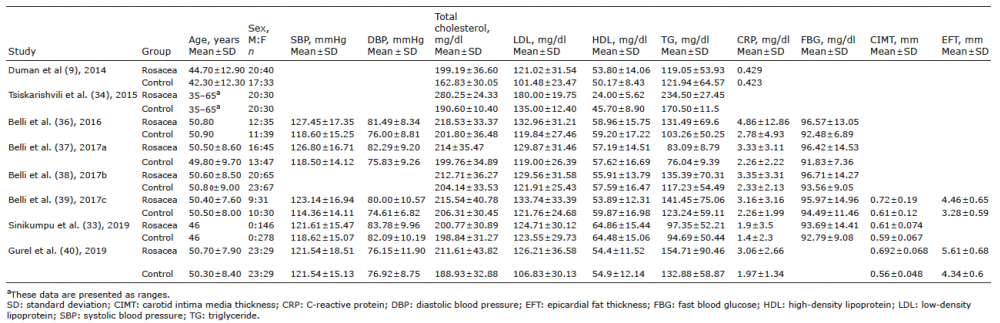 Click to show fullsize
Click to show fullsize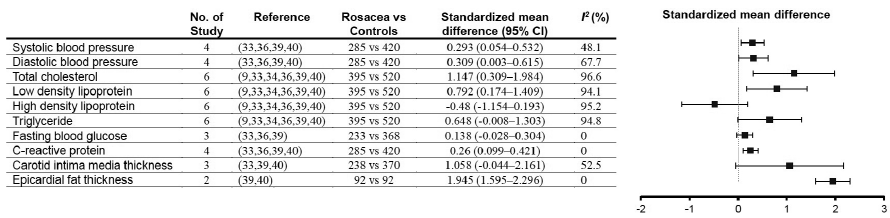 Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize