


1Department of Dermatology, Sheba Medical Center, Tel-Hashomer, 2Sackler Faculty of Medicine, Tel Aviv University, Tel Aviv, 3Department of Dermatology, Soroka University Medical Center, 4Faculty of Health Sciences, Ben Gurion University of the Negev, Beer Sheva, 5Pediatric Dermatology Unit, Schneider Children’s Medical Center of Israel, Petah-Tikva and 6Faculty of Medicine, Hebrew University of Jerusalem, Israel; Pediatric Dermatology Service, Department of Dermatology, Hadassah Medical Center, Jerusalem, Israel
Cutaneous leishmaniasis poses a therapeutic challenge in the paediatric population. The aim of this study was to assess the efficacy and safety of miltefosine treatment for Old World cutaneous leishmaniasis in paediatric patients. A multicentre retrospective review of 10 children (≤ 18 years of age) with cutaneous leishmaniasis treated with miltefosine in Israel was performed. Mean ± standard deviation age at diagnosis was 9.1 ± 5.0 years. The Leishmania species diagnosed was L. tropica in 8 cases and Leishmania major in 2 cases. Mean ± standard deviation duration of treatment was 44.8 ± 20.6 days, with a mean follow-up period of 12.1 ± 17.1 months. Complete response was noted in 8 (80%) patients. Treatment failure was noted in 2 (20%) cases. Side-effects related to the medication were minimal. In conclusion, oral miltefosine may be an effective and safe treatment for Old World cutaneous leishmaniasis caused by Leishmania tropica or Leishmania major in children. However, further studies are warranted to draw a definite conclusion.
Key words: leishmaniasis; Leishmania tropica; Leishmania major; miltefosine; amphotericin B; sodium stibogluconate.
Accepted Oct 15, 2020; Epub ahead of print Oct 19, 2020
Acta Derm Venereol 2020; 100: adv00322.
doi: 10.2340/00015555-3669
Corr: Ayelet Ollech, Pediatric Dermatology Clinic, Department of Dermatology, Sheba Medical Center, Tel-Hashomer, Israel. E-mail: ayelet.ollech@sheba.health.gov.il
Treatment options for cutaneous leishmaniasis warranting systemic therapy in the paediatric population include sodium stibogluconate and liposomal amphotericin B. Both of these are intravenous formulations with potentially significant side-effects. There are limited reports on the use of miltefosine in the treatment of Old World cutaneous leishmaniasis in children. In this case series of 10 paediatric patients with recalcitrant cutaneous leishmaniasis caused by Leishmania tropica and Leishmania major species, treat-ment with oral miltefosine was effective in 80% of patients. The oral route of administration was favourable for the patients, with minimal side-effects.
Leishmaniasis is an endemic infestation of the Leishmania parasite with cutaneous, mucosal, or visceral manifestations. Treatment options for diffuse cutaneous and mucosal-visceral subtypes can be prolonged, inconvenient and have potential side-effects (1, 2). Treatment failure can result in scarring in the cutaneous form and more severe complications in the mucosal and visceral forms (1).
In the paediatric population intralesional (IL) or intravenous (IV) administration of medication can be painful and inconvenient, often requiring admission to hospital or day-care facilities for a prolonged time of 6 days to as long as 28 days. An oral medication, which can be taken at home with good tolerance and efficacy, may be a good option in this population (2). In addition, drug resistance is emerging and treatment failures of established treatments are more common (3–6). There is a need for additional treatment options in such cases of treatment failure.
Miltefosine (Impavido, Profunda Inc., USA) is an alkyl phosphocholine drug with anti-Leishmania activity through inhibition of the parasite’s membrane and its metabolic pathways and induction of apoptosis (7, 8). It is manufactured by Profunda Inc. and is approved for sale in Germany, India, Israel, and the USA. Miltefosine has been European Medicines Agency (EMA) approved since 2002 and US Food and Drug Administration (FDA) approved since 2014 for use in subjects who are 12 years and older for visceral leishmaniasis (VL) caused by Leishmania donovani, mucosal leishmaniasis caused by Leishmania braziliensis and cutaneous species mostly from the New World (American), including Leishmania braziliensis, panamensis, and guyanensis. In other species and for patients under 12 years of age, miltefosine is used off-label (7–9).
Adverse events from miltefosine are mild, and may include gastrointestinal symptoms; nausea, vomiting, and diarrhoea in 35–60% of patients, and elevation of liver enzymes and creatinine in 10–20% of patients. Monitoring of blood-urea nitrogen (BUN) test, creatinine, liver transaminases, and total bilirubin levels is recommended weekly, while taking the medication and repeat BUN test and creatinine levels are recommended a month after stopping the drug. For visceral leishmaniasis platelet count monitoring is also recommended (10).
The majority of the literature addresses treatment with miltefosine for the adult population (11, 12) and New World species (8, 13, 14). A review of the paediatric literature reveals a few case reports of miltefosine for Old World (Eastern Hemisphere) cutaneous leishmaniasis (8, 15, 16). There is a single report of successful miltefosine treatment for L. tropica in 2 adolescents from Afghanistan (17).
This paper describes a series of 10 paediatric patients with cutaneous leishmaniasis resistant to recommended therapy, who were consequently treated with miltefosine. The study aimed to assess the efficacy and tolerability of this medication in this cohort and report on the side-effects of the treatment.
This was a retrospective case review of all paediatric patients (≤ 18 years of age) with cutaneous leishmaniasis treated with miltefosine at 4 tertiary medical centres in Israel between 1 January 2015, and 31 December 2019.
Epidemiological variables, place of residence, personal medical history, diagnostic evaluations, Leishmania species, duration of illness, number of lesions, distribution, treatment and treatment duration, clinical response, recurrences, and side-effects of therapy were recorded. Identification of Leishmania species was performed using PCR, carried out on samples from the affected lesion/s using species-specific probes (18).
The indications for systemic treatment were: topical treatment failure; multiple lesions (≥ 5); or non-feasibility of intralesional injection because of the anatomical location (e.g. face and eyelid) (19).
Clinical responses were categorized as follows (20–22). Complete response was defined as 100% re-epithelialization of the ulcer, or for non-ulcerative lesions, regression of the lesion, within 3 months after treatment. Partial response was defined as greater than 50% re-epithelialization of the ulcer or regression within the same period. Treatment failure was defined as less than or equal to 50% re-epithelialization of the ulcer or regression of the lesion within the same period. In addition, any patient who achieved either a complete or partial response within 3 months, but had a relapse at the same distribution during the follow-up period was also considered a case of treatment failure. Treatment was continued in cases of active lesions who achieved partial response, to minimize future aesthetic disfigurement.
Descriptive statistics for demographic and clinical characteristics include mean with standard deviation (SD) for continuous variables and frequency distributions for categorical data. The study was approved by the local institutional review board (IRB) committees.
A total of 10 patients were included in the study (9 females, 1 male). Mean ± standard deviation (SD) age at diagnosis was 9.1 ± 5.0 years. Patient’s place of residence varied and were endemic for the L. major and L. tropica species.
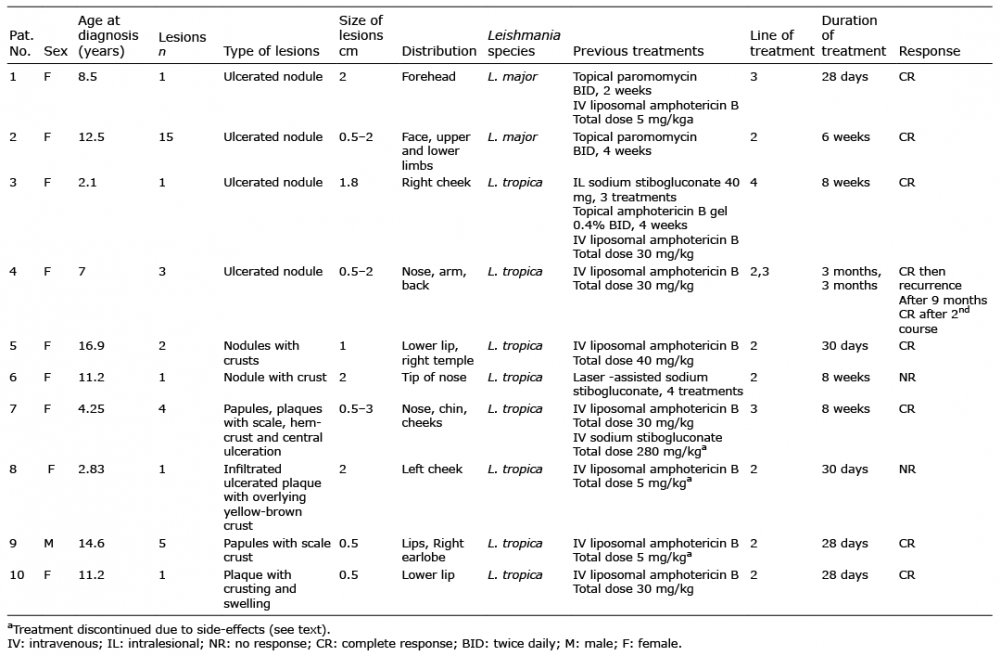
Demographic data, clinical characteristics, and outcomes are shown in Table I.
Table I. Clinical characteristics and response of 10 patients treated with miltefosine for cutaneous leishmaniasis
The mean number of lesions at presentation was 3.67 (range 1–15). Facial lesions were present in 10/10 patients (100%). The mean size of the lesions was 1.4 cm (range 0.5–3 cm). 6 cases had ulcerated lesion at presentation. The remaining 4 had infiltrated nodules or plaques.
Leishmania species identified were L. tropica in 8 cases and L. major in 2 cases.
Miltefosine was not given as a first-line treatment in any of the cases. In 6 cases miltefosine was the second line of treatment, in 3 cases miltefosine was the third line of treatment and in one case it was the fourth line of treatment.
The reason for drug change was treatment failure in 9 previous treatment episodes, including topical paromomycin and methyl benzethonium ointment (2 patients), topical amphotericin B gel (1 patient), laser-assisted sodium stibogluconate (1 patient), IL sodium stibogluconate (1 patient), liposomal amphotericin B (4 patients), and adverse effects in 4 patients, including severe allergic reaction to amphotericin B (3 patients), elevated liver function tests, amylase, and lipase following IV sodium gluconate (1 patient). The side-effects of the medications in these 4 cases were severe and necessitated discontinuation of treatment and switching to miltefosine.
The dosing of the medication was weight-based according to 3 mg/kg/dose divided into 3 doses (maximum 150 mg/day). The mean duration of treatment was 44.8 days (range 28–90 days). The patients’ parents were informed about the off-label use and, gave their informed consent prior to treatment initiation.
A complete response was noted in 8 (80%) patients. Treatment failure was noted in 2 (20%) cases. The presenting lesions and successful outcome of one patient (patient 7) following 28 days of miltefosine treatment is shown in Fig. 1.
Fig. 1. (a) Leishmania tropica in a 4-year-old girl who presented with papules, plaques, and ulcerated plaques on her face. (b) Complete response was noted after 28 days of treatment with miltefosine.
In one patient (patient 4), 9 months after clearance of the lesions, the rash recurred on the previous post-lesional scar (Leishmania recidivans). An additional course of miltefosine treatment was given with clearance of the rash. No recurrence was noted after the second course of treatment during the time of follow-up (52.8 months for this case). The patient’s lesions at presentation and after the second course of miltefosine are shown in Fig. 2.
Fig. 2. (a) Leishmania tropica in a 7-year-old girl who presented with a massive lesion on the tip of her nose. (b) Complete response was noted after 2 courses of miltefosine.
In the 2 cases that resulted in treatment failure, additional treatment options were given: in patient 6 further treatments included daylight photodynamic therapy (PDT) with no response, followed by 4 courses of IL sodium gluconate injections, which resulted in complete response. In one patient (patient 8), a third line of treatment was given; daylight PDT, with complete resolution of the lesions.
Adverse effects related to treatment with miltefosine were mild, and included nausea, vomiting, and abdominal pain in 2 (20%) patients, which did not necessitate discontinuation of treatment.
The sequelae of the lesions resulted in mild dyspigmentation in one patient and atrophic scars in 3 patients.
This report shows that miltefosine treatment for paediatric patients with cutaneous Old World leishmaniasis can be effective and safe. The strengths of the study include a multicentre cohort in a resistant patient population and long-term follow-up. A complete response was seen in 80% of patients.
Available treatments for cutaneous leishmaniasis include topical antimonial preparations, intralesional antimonial injections, and systemic agents, including pentavalent antimony and liposomal amphotericin B (1, 23). Topical paromomycin shows variable efficacy of 39–82% cure rates; however, with much lower response rates in L. tropica infection (24, 25). IL antimonial injections, such as sodium stibogluconate, are considered effective, showing an 83–93% cure rate (26, 27). Systemic pentavalent antimony has shown a 60–80 % cure rate (23). Intravenous (IV) liposomal amphotericin B has shown a cure rate of 84% (19). However, these treatments are poorly tolerated and are inconvenient for patients and their families. In the paediatric population IL or IV administration can be painful and often requires anaesthesia or admission to hospital or day-care facilities for a prolonged time of 6–28 days. An oral medication that can be taken at home with good tolerance and efficacy can be a good option in this population (2).
The majority of studies on paediatric use of miltefosine were performed in India, for the indication of VL. The dosing regimen used was 1.5–2.5 mg/kg/day, 50 mg/day (≤ 25 kg) or 100 mg/day (> 25 kg). Response rates were 81–94%, which is similar to those in adult studies (14). A randomized controlled trial for the treatment of Leishmania species from Brazil and Colombia; L. panamensis and L. guyanensis showed non-inferiority of miltefosine compared with meglutamine antimoniate with a good safety profile; failure rate was 17.2% for miltefosine and 31% for meglumine antimoniate (13). In another comparative study of treatment of L. panamensis showed failure rates of 8.92% for miltefosine vs 22.03% for meglutamine antimoniate (p = 0.006) (10).
Further review of the paediatric literature reveals a few case reports of miltefosine for Old World cutaneous leishmaniasis. A 1-year-old girl with L. infantum was treated with a 28-day course of miltefosine, and the lesion showed regression after 8 weeks and complete healing after 6 months (15). A 15-year-old girl with L. major was treated with a 28-day course of miltefosine with clinical cure at 9 months (8). An 8-year-old girl with L. major was treated with 2 courses of liposomal amphotericin B with clearance after the second course and continued treatment with miltefosine for prevention of relapse (16).
There is a single report of successful miltefosine treatment for L. tropica in 2 adolescents from Afghanistan. A 14-year-old was treated with miltefosine for 28 days and had clinical cure at 9 months, and a 19-year-old male was treated with miltefosine for 28 days with regression at 5 months (17).
In the current cohort of 10 patients in whom at least one previous treatment had failed, complete cure was achieved in 80% of patients. Failure was seen in 2 patients. In both cases, the Leishmania species was L. tropica and the affected area was the face; the tip of the nose (patient 6) and cheek (patient 8). Interestingly, both cases had only a single skin lesion. Patient 8 was 2.8 years of age when she was treated, one of the youngest patients in the cohort. The cause of the treatment failure might be suboptimal dosing. Dorlo et al. (7) showed that children were relatively underexposed to miltefosine compared with adults when given the same mg/kg dosage, and that an allometric dosing schedule may have a better yield in children (28). Thus, higher doses of the drug might be needed. An additional reason might be the location of the lesions. In our experience, the tip of the nose is frequently resistant to treatment, possibly due to decreased vascularity and therefore low drug levels, as seen in patient 6 in the our cohort
One patient relapsed after 9 months. Several cases of relapse, after initial successful primary miltefosine treatment in immunocompetent patients, have been reported for VL and diffuse cutaneous leishmaniasis (3, 5, 6). To the best of our knowledge, this is the first report on relapse in Old World cutaneous leishmaniasis. The relapse probably did not result from the emergence of resistance, as the second course of miltefosine led to complete cure.
The medication package insert recommends a treatment duration of 28 days (22). In 3 cases treatment duration was prolonged from 6 weeks to 3 months due to partial response. Prolongation of treatment achieved a favourable effect without side-effects.
Cutaneous leishmaniasis has been reported to resolve spontaneously. In this series, we evaluated recalcitrant cases in which systemic treatment was indicated for the lesions. Complete response was seen after 1–3 months of therapy with miltefosine; therefore, the response was attributed to the therapy and not to spontaneous resolution. In contrast, in 2 reports of possibly successful miltefosine treatment in L. tropica leishmaniasis after 5 and 9 months (8, 17), the final outcome may be attributed to spontaneous regression of the disease.
Further studies are required to establish the optimal treatment duration for miltefosine in cutaneous leishmaniasis.
Study limitations
Limitations of this study include its retrospective design and small patient population. Likewise, various treatment protocols were applied, since there are no well-established guidelines for therapy with miltefosine.
Conclusion
This study suggests that miltefosine may be an effective and safe oral medication for the treatment of Old World cutaneous leishmaniasis caused by L. major and L. tropica in children. Randomized controlled studies are warranted to draw a definite conclusion. This adds another option to the limited range of treatments available, with a much more convenient (oral) route of administration, which may improve the quality of life of these children and their families. In cases of partial response to miltefosine, in our experience, prolongation of treatment with miltefosine, for 2–8 additional weeks beyond the 28 days, can achieve a complete response without an increased risk of side-effects.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize