


¹Infectious Diseases and Dermatology Unit, ²Microbiology Laboratory, and ³INSERM CIC 1410, CHU Réunion, FR-97410 Saint Pierre, La Réunion, France. *E-mail: antoine_bertolotti@yahoo.fr
#These authors contributed equally.
Accepted Oct 21, 2020; Epub ahead of print Oct 26, 2020
Acta Derm Venereol 2020; 100: adv00313.
doi: 10.2340/00015555-3675
Chlamydia trachomatis (CT) is the most common bacterial sexually transmitted infection (STI) (1). While a single dose of azithromycin (AZM) is generally recommended for treating patients with asymptomatic urogenital CT, treatment guidelines for asymptomatic rectal CT (AR-CT) vary between countries. European and World Health Organization (WHO) guidelines advise treating AR-CT with doxycycline 100 mg twice a day for 7 days (1, 2), whereas US Centers for Disease Control and Prevention recommend either a doxycycline regimen or a single 1-g dose of AZM to maximize adherence in populations with high-risk behaviour (3). However, the effectiveness of different treatments for AR-CT has been evaluated in only a few retrospective studies and a meta-analysis (4–6), all of which emphasized the importance of compliance for the success of treatment.
In this context, and given the poor compliance of patients with high-risk behaviour in Reunion Island, we report the results of treatment of AR-CT with a single 1-g dose of AZM, and discuss whether this treatment could be proposed as surrogate method for use in poor adherence settings.
A retrospective cohort study was conducted at the STI department of St Pierre Hospital in Reunion Island from data collected between 1 January 2016 and 31 July 2019. As part of the epidemiological surveillance mission, all patients who visited the department during this period answered a standardized questionnaire regarding their sexual behaviour. Patients with STI risk factors were invited to undergo HIV, syphilis, hepatitis B and C screening by enzyme-linked immunoassay (ELISA), as well as Neisseria gonorrhoeae (NG), Mycoplasma genitalium (MG) and CT screening by real-time multiplex PCR (urethritis basic kits, Fast-Track Diagnostics®, Luxembourg) on pharyngeal, vaginal, urinary and rectal samples. All patients diagnosed with rectal CT were enrolled in the cohort, and those with MG or lymphogranuloma venereum were ruled out. Participants were treated orally with a single 1-g dose of AZM and asked to undergo a test-of-cure with CT screening 6 weeks later. This study was conducted according to the reference methodology MR-004 from the National Commission of Informatics and Liberties (CNIL). In accordance with French regulations, this study was also recorded in the register of the National Institute of Health Data (number MR 3509160420).
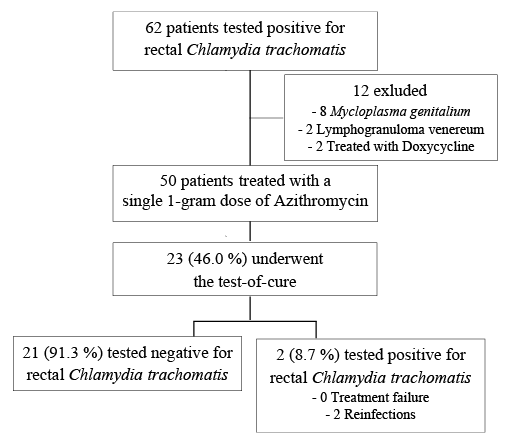
A total of 62 patients tested positive for rectal CT. Of these, 8 were also positive for rectal MG, 2 had lymphogranuloma venereum, and 2 have been treated with doxycycline for 7 days (Fig. 1). The final cohort comprised 50 patients, with a median age of 27 years (interquartile range (IQR) 25–39 years), 35 (70.0%) of whom were male (Table I). Twenty-three patients (46.0%) underwent the test-of-cure. There were no significant differences in baseline characteristics between those who re-tested and those who did not. Among those who re-tested, 21 (91.3 %) were CT-negative and 2 were CT-positive. After examination of their medical file, CT infection in the last 2 patients was attributed to reinfection rather than to treatment failure. The first patient was co-infected both with NG and syphilis, and she was known to have epileptic and psychiatric disorders (several hospitalizations for psychiatric and social reasons were reported in her medical file). The second patient, a homosexual man with HIV, was a regular visitor to the STI department and reported engaging in risky sexual behaviour.
Fig. 1. Study population.
Table I. Characteristics of the study population (n = 50)
In this uncontrolled open-label retrospective cohort study, no treatment failure was observed in patients who received a single 1-g dose of AZM. Thus, we conclude that this regimen could be effective against AR-CT.
Importantly, a pharmacokinetic study has found that AZM titres in rectal tissue remain above the minimum inhibitory concentration for CT for at least 14 days after administration of a 1-g dose of AZM (7). Recent studies, however, have suggested that administration of AZM increases macrolide resistance in MG, prompting concerns about the appropriateness of this treatment (8). Yet, while increasing macrolide resistance has been observed in MG worldwide, this has not been the case in Reunion Island (5.9%) (9). Moreover, in our centre, no increase in the incidence of MG infection has been observed in recent years. According to the latest recommendations, only symptomatic patients with treatment failure for CT and NG should be screened for MG. However, in Reunion Island there is a high prevalence of asymptomatic MG infection, especially in women, who represent 30% of the study population, and this may be responsible for pelvis inflammatory disease and infertility. In areas where resistance to AZM is low and poor adherence common, routine screening of at-risk populations for MG could be proposed. Indeed, the prevalence of MG is more important than that of NG, complications are at a similar level to CT, and triplex PCR techniques are often the same price as biplex techniques. This supports systematic screening to continue the use of single-dose AZM to treat AR-CT without fear of the emergence of resistance in undetected MG.
This work has several limitations. First, this is an open-label retrospective observational study with no comparator group and a small sample size, which means that it has a low level of evidence. Secondly, more than half of the patients did not undergo the test-of-cure (this is similar to the results of other studies) (4, 5). Yet, while the latter reflects poor compliance among high-risk Reunionese patients, it also reinforces our opinion that a single-dose treatment could be more appropriate than a multi-day regimen for the treatment of AR-CT. Surprisingly, the subgroup of patients who underwent the test-of-cure might have been underestimated, because some of them were returned anonymously, making the control test impossible to link to the initial test. Notwithstanding, it is worth mentioning that all of the anonymous tests labelled as test-of-cure were negative.
In conclusion, this retrospective cohort study suggests that a single 1-g dose of AZM could be effective for treatment of AR-CT, so long as it is accompanied by systematic MG screening and a test-of-cure. However, randomized clinical trials are necessary before this can be proposed as a surrogate treatment for AR-CT in poor compliance settings.
The authors would like to thank the team at our sexually transmitted infection department for their precious help and our copy editor Arianne Dorval.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize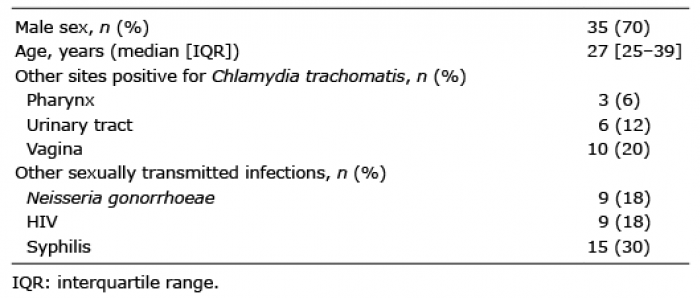 Click to show fullsize
Click to show fullsize