


Department of Dermatology, Geneva University Hospital, Rue Gabrielle-Perret-Gentil 4, CH-1205 Geneva, Switzerland. E-mail: shireen.dumont@gmail.com
Accepted Oct 21, 2020; Epub ahead of print Oct 26, 2020
Acta Derm Venereol 2020; 100: adv00314.
doi: 10.2340/00015555-3676
Cocaine use, by its pro-adrenergic, prothrombotic and proinflammatory actions, can lead to a wide variety of clinical conditions (1). Cocaine-induced midline destructive lesions (CIMDL) are the most frequent mucocutaneous manifestations and are caused by drug-induced chronic rhinitis leading to the destruction of osteocartilaginous structures of the nose, sinuses and palate (2). Cocaine use may also cause vascular injuries manifesting as systemic disease, including acute myocardial ischaemia, thrombosis, ischaemic stroke, organ infarction or vasculitic syndromes mimicking primary autoimmune diseases (3). In the skin, it may lead to Raynaud’s phenomenon, distal ulcers or retiform purpura. Few cases of neutrophilic diseases associated with cocaine abuse have been reported and most of them manifest as pyoderma gangrenosum (PG) (1, 4–7). We report here a severe case of cocaine-induced neutrophilic systemic disease with neutrophilic infiltrates involving the skin and multiple organs, presenting as PG ulcers and aseptic organ abscesses with a serological profile of vasculitis. The clinical picture in the presented case may be difficult to distinguish from granulomatosis with polyangiitis (GPA) (3).
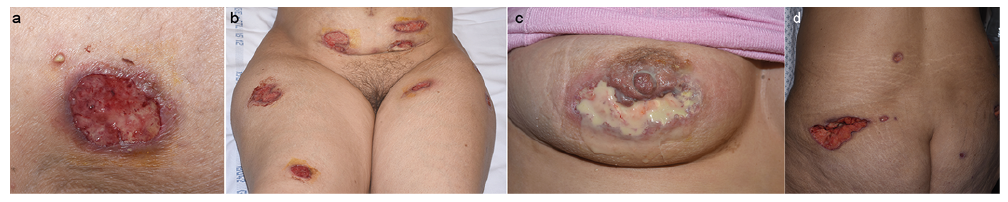
A 40-year-old woman presented with numerous pustules and large skin ulcers over the whole body and had no significant medical history. Initially, she presented a solitary deep abscess on the buttock that did not respond to several courses of antibiotics. After 3 weeks, cutaneous pustules and nodules appeared over her entire body, evolving rapidly into painful ulcers (Fig. 1a). She did not present fever or other symptoms, had not travelled recently, and had no family medical history. She reported only one recent recreational use of cocaine. Physical examination revealed multiple pustules, nodules and superficial skin ulcers on her chest, upper and lower extremities (Fig. 1b, c). She had 2 large, 4 cm-deep, ulcers on the buttocks (Fig. 1d). All ulcer borders were purplish-red, undermined, and boggy with perforations that drained pus, consistent with PG. A few days after admission, she developed a dental abscess. Laboratory tests showed macrocytic anaemia, and an inflammatory syndrome. Serological tests ruled out hepatitis, HIV, parvovirus B19, syphilis and Epstein-Barr virus infection. Immunological tests revealed the presence of perinuclear anti-neutrophil cytoplasmic antibodies (pANCA) positive for antiproteinase 3 (PR3) and antimyeloperoxidase (MPO) negative, antiphospholipid antibodies were negative. Microbiological samples taken from blood and ulcers were all negative. Histopathological results of 2 skin biopsies showed dermal infiltrates consisting mainly of neutrophils, histiocytes and eosinophils with no vascular involvement. Direct immunofluorescence was negative. A full-body computed tomography (CT) scan revealed only a small nasal septal perforation. The patient was initially treated with oral prednisone, skin ulcers improved with no sign of new lesions. Soon after discharge from the hospital, she developed new cutaneous ulcers associated with deep intra-abdominal and pulmonary abscesses (Fig. 2a, b). Urine toxicology and hair drug test were positive for cocaine and negative for levamisole. The patient improved after drainage of abdominal and pulmonary abscesses (analysis of which revealed their aseptic nature) and cessation of cocaine use, she did not receive any other treatment. Based on the clinical history, a final diagnosis of cocaine-induced neutrophilic disease was retained, with neutrophilic dermatosis and multiple aseptic organs abscesses.
Fig. 1. (a) A pustule and an ulcer with purplish-red and undermined edges on the right leg. (b) Clinical images of multiple ulcerations on the lower abdomen and top of the thighs. (c) A purulent ulcer on the right breast. (d) A deep ulcer on the left buttock.
Fig. 2. Computed tomography showing (a) a voluminous mesenteric abscess (white arrow) and (b) a lung abscess (black arrow).
There are a wide range of clinical conditions associated with cocaine abuse, from localized (CIMDL, retiform purpura, PG) to systemic disease (1, 2, 4, 8). It is not clear whether clinical manifestations are due to levamisole, an immunomodulator added to cocaine as a bulking agent, or to the cocaine itself. Cocaine and levamisole seem to enhance inflammation and autoimmunity (9). A well-known complication of levamisole-contaminated cocaine is ANCA-vasculitis, which presents with a retiform purpura and haemorrhagic bullae on the face, ears and extremities (10). PG is already recognized as a rare complication of cocaine abuse (5, 11), and ulcers in cocaine-induced PG often share the characteristics of conventional forms. Levamisole may play a role in the development of cocaine-induced PG lesions. In most reported cases, immunological markers are similar to those found in levamisole-induced vasculitis, and skin biopsies may present with histological findings of vasculitis, even if levamisole exposure has not been detected, tested, or it is negative (1, 5). In the current case, the patient developed superficial PG ulcers with no sign of vascular involvement on skin biopsy and no traces of levamisole in the hair. She also displayed painful subcutaneous nodules and, following cocaine relapse, deep sterile lung, dental and abdominal abscesses that could be consistent with a deep form of neutrophilic disease (extracutaneous PG). To our knowledge, all published cocaine-induced PG manifest as superficial ulcers and no deep-seated and extended disease, as in our patient, has been reported (4–7, 11). The concept of neutrophilic systemic disorder has emerged, with neutrophilic infiltrate being described in the skin, but also in many organs (8). Clinico-biological conditions induced by chronic use of cocaine may be difficult to distinguish from immunological diseases (especially ANCA-vasculitis as GPA) due to similar nasal (2) and skin lesions (4), and serological findings that can mirror those found in vasculopathy (4, 12). However, the lack of expected systemic symptoms in our patient (renal damage, fever, arthralgias) and the course of the disease make the diagnosis of GPA less likely (4). Most cocaine-related neutrophilic dermatoses display serological abnormalities with positive ANCA with both MPO-ANCA and PR3-ANCA. In the current patient, pANCA against PR3 have been detected, which is not usual, because anti-PR3 typically produces a pattern of cytoplasmic positivity (cANCA) on indirect immunofluorescence (IIF) (13). It has been demonstrated that a discordance between the patterns of ANCA on IIF and the presence of specific antigenic targets, such as ANCA reacting with human neutrophil elastase (HNE), may be markers of clinical conditions induced by cocaine (13, 14). Unfortunately, we did not have access to the HNE assay at our centre. The current case reveals an uncommon presentation of neutrophilic dermatosis induced by cocaine with both superficial ulcers and deep sterile abscesses, revealing a neutrophilic systemic disorder with a serological profile of vasculitis. There was no evidence of levamisole detected in the hair, suggesting that levamisole is not always responsible for cocaine-induced neutrophilic dermatoses, such as PG, and no specific serological profile is indicative of levamisole toxicity (11). Neutrophilic systemic disease may appear as a complication of cocaine use and has to be distinguished from vasculopathy. It is important to always suspect and rule-out this systemic complication, cocaine avoidance being the cornerstone of the treatment.
Written informed consent was obtained from the patient for publication of this case report and any accompanying images. A copy of the written consent is available for review.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize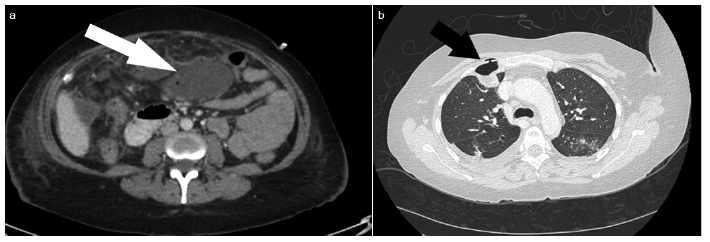 Click to show fullsize
Click to show fullsize