

Ingrid Lindberg1, Mathias Lilja1, Kirk Geale1,2, Haijun Tian3, Craig Richardson4, Amie Scott5 and Amra Osmancevic6,7
1Quantify Research, Stockholm, 2Dermatology, Department of Public Health and Clinical Medicine, Umeå University, Umeå, Sweden, 3Novartis Pharmaceuticals Corporation, East Hanover, NJ, USA, 4Novartis Pharma AG, Basel, Switzerland, 5KMK Consulting Inc., Morristown, NJ, USA, 6Department of Dermatology and Venereology, Institute of Clinical Sciences, Sahlgrenska Academy, University of Gothenburg, and 7Region Västra Götaland, Sahlgrenska University Hospital, Department of Dermatology and Venereology, Gothenburg, Sweden
The incidence of psoriatic arthritis in patients with psoriasis is unclear; existing estimates differ by a factor of ten. Complete population-level data is needed to provide accurate estimates with high confidence. A total of 123,814 adults with psoriasis, free from pre-existing psoriatic arthritis, were identified in population-based data from secondary care in Sweden during 2007 to 2017. Incidence was calculated as the number of psoriatic arthritis diagnosis events per 100 patient-years. Time to diagnosis was assessed using cumulative incidence and Cox proportional hazards models to identify risk factors. Incidence of psoriatic arthritis in patients with psoriasis was 1.69 per 100 patient-years (95% confidence interval 1.65–1.72) overall, and 1.48, 3.00, and 5.49 per 100 patient-years in patients with mild, moderate and severe psoriasis, respectively. Risk of psoriatic arthritis was 3.2 times higher amongst patients with severe psoriasis compared with mild disease. Dermatologists should regularly assess risk factors for psoriatic arthritis in clinical practice in order to improve the detection of psoriatic arthritis.
Key words: incidence; epidemiology; risk factors; psoriatic arthritis; psoriasis; biologics.
Accepted Oct 28, 2020; Epub ahead of print Nov 2, 2020
Acta Derm Venereol 2020; 100: adv00324.
doi: 10.2340/00015555-3682
Corr: Kirk Geale, Dermatology, Department of Public Health and Clinical Medicine, Umeå University, SE-901 87 Umeå, Sweden. E-mail: kirk.geale@umu.se
Although onset of psoriatic arthritis commonly occurs in patients with skin psoriasis, the number of patients affected is unclear. This study used population-based data to provide highly accurate estimates. The results showed that if 10,000 patients with skin psoriasis were followed-up, 169 would be diagnosed with psoriatic arthritis within one year. Patients with more severe skin psoriasis were more likely to be diagnosed with psoriatic arthritis than patients with less severe skin psoriasis. Other risk factors were also identified, which doctors can use to better identify psoriatic arthritis in patients with skin psoriasis and to optimize how they are treated.
Skin psoriasis (PsO) is a chronic, immune-mediated, systemic inflammatory disease affecting 2–4% of the population in Western countries (1). The disease imparts significant patient burden, partially due to the many associated comorbidities. Psoriatic arthritis (PsA), a heterogeneous, immune-mediated disease characterized by inflammation, pain, and stiffness in the joints, is the most well-known (2). Studies have shown that many patients with skin PsO ultimately develop PsA, but the rate of onset and progression are not well understood (3–5).
Like skin PsO, PsA is associated with substantial humanistic and economic burden (6). Prevalence of PsA in patients with skin PsO has been estimated to be 22.7% in Europe (7) and 30% in Sweden (8). Existing literature on the incidence of PsA among patients with skin PsO is inconsistent, with estimates ranging from 0.23 to 2.7 per 100 patient-years (100 py) (5, 7, 9–15), a factor of more than 10. In a review, cumulative incidence rates were also variable, partially depending on the follow-up duration assessed (7). Disease incidence rate is a fundamental quantity in epidemiology, and the incidence of PsA in patients with skin PsO has not been established with an adequate level of accuracy.
Furthermore, establishing the risk factors for disease onset may contribute aetiological and pathological understanding of the disease and help to identify and treat patients early and accurately. Risk factors for onset of PsA are wide ranging, and include type of psoriasis, demographics, genetics, socioeconomics, lifestyle factors, and clinical factors including disease severity (4, 5, 9, 12, 14, 16–21). Early detection and treatment of PsA in skin PsO could represent an opportunity for prevention and reduction in progression (including joint damage) of disease (22).
The Nordic countries maintain administrative registry data with complete coverage that are optimal for studying disease epidemiology. To the best of our knowledge, no existing research has estimated incident PsA in patients with skin PsO in the Nordic countries or using an entire country’s population. The aim of the current study was to determine reliable data for the incidence of PsA in patients with skin PsO, using an observational, retrospective, Swedish cohort study design with lifetime follow-up. A further aim was to assess the risk factors for disease onset using a wide variety of predictors.
Data and ethics
This study used 4 population-based secondary administrative registries containing pseudonymized healthcare data from routine Swedish clinical care, including the National Patient Registry, the Prescribed Drug Registry, the Longitudinal Integration Database for Health Insurance and Labour Market Studies (Swedish acronym: LISA) and the Cause of Death Registry. The National Patient Registry (NPR) includes International Classification of Disease version 10 (ICD-10) diagnosis codes and corresponding dates at in- and out-patient visits to providers of secondary care. The Prescribed Drug Registry (PDR) includes data on all pharmacy-dispensed medications from primary and secondary care, including medications and dispensation dates. LISA contains socioeconomic information, including income, education level, marital status, and migration information. The Cause of Death Registry (CDR) includes the death date. Unique personal identification numbers were used to link data from each registry. The study was approved by the Regional Ethical Review Board in Stockholm.
Study population and design
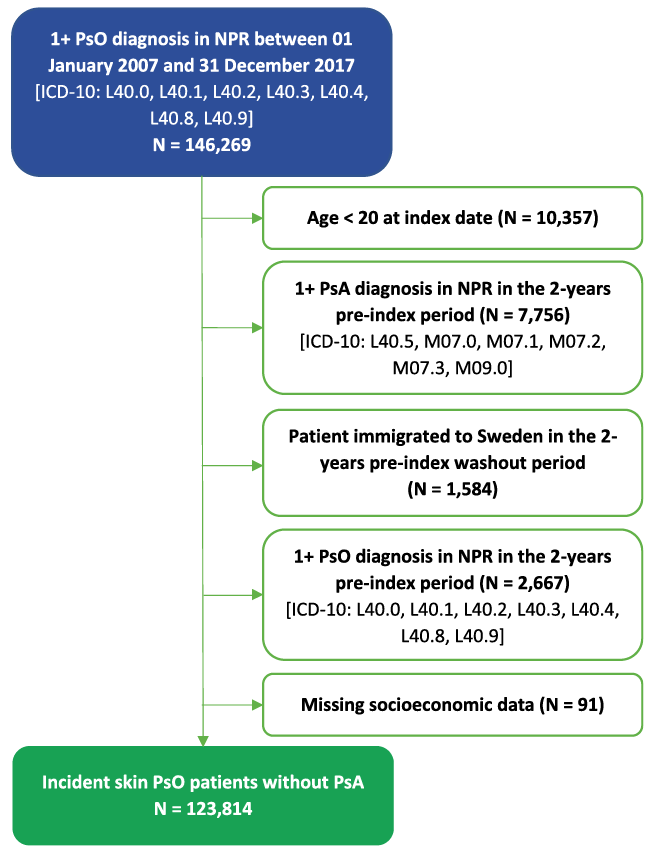
An open cohort of patients with at least one observational diagnosis of skin PsO (ICD-10: L40.0–4 or L40.8–9), as done in previous studies (12–14), registered in the NPR during 2007 to 2017 were enrolled in the study, where the first diagnosis of skin PsO was defined as the index date and start of follow-up. Patients were excluded if they had pre-existing PsA (ICD-10: L40.5, M07.0–3 or M09.0) or skin PsO, or immigrated into Sweden, during the 2 years prior to index. Patients were also excluded if they were below the age of 20 years at index (18 at the start of the exclusion criteria assessment) (Fig. 1). Data collection was prospective, but patients were identified and followed-up retrospectively.
Fig. 1. Patient flow chart depicting the study inclusion and exclusion criteria. Skin psoriasis (PsO) was defined as an International Classification of Diseases, 10th Revision (ICD-10) diagnosis of L40.0–4 or L40.8–9 in the National Patient Registry (NPR) between 2007 and 2017 (index date). Onset of psoriatic arthritis (PsA) was defined as a diagnosis of ICD-10 L40.5, M07.0–3 or M09.0 on the date of or after the diagnosis of skin PsO during 2007 to 2017. Patients below the age of 20 years at index were excluded, as were patients with pre-existing PsA or skin PsO or those who immigrated into Sweden during the 2 years preceding the index date. Patients with missing socioeconomic data were excluded.
The event of interest in this study was onset of PsA following an incident diagnosis of skin PsO. Time at risk was calculated as the duration from index date to onset of PsA or censoring (emigration, death, or end of data). A complete-case analysis was applied to the population and no imputation was conducted.
Disease severity
Patients were classified into severity subgroups defined by treatment proxy according to treatment received at any time up to the index date. Patients receiving skin PsO-indicated biologic treatments or apremilast were classified as biologic-treated patients (severe disease proxy), those receiving skin PsO-indicated conventional systemics including phototherapy were classified as conventional systemic treated patients (moderate proxy), and the remaining patients were classified as other (mild proxy), in line with treatment guidelines (23–25). In Sweden, biologics and apremilast are typically used for patients with moderate-to-severe disease who did not respond to or tolerate conventional systemic therapy, or in those with contraindications for conventional systemic therapy. Similar classifications have been used previously (26–28). Refer to the Table SI for a list of treatments used for skin PsO severity classifications.
Statistical analysis
Descriptive statistics were computed for patients at risk, overall and stratified by treatment as proxy for disease severity as mean ± standard deviation (SD) for continuous variables and number and percentage for categorical variables. Incidence rates were calculated as the number of incident PsA events divided by the number of patient-years at risk per 100 py. Time at risk was calculated as the years between diagnosis of skin PsO and onset of PsA or censoring (death, emigration, or end of data). Incidence rates were calculated overall and in severity subgroups. As a sensitivity analysis, patients receiving conventional systemic or biologic treatment were combined into 1 group (moderate-to-severe proxy) to align with the indication for all PsO-indicated biologics and apremilast.
Time to onset of PsA was visualized using cumulative incidence curves (1-Kaplan–Meier) and associations between risk factors and incident PsA was analysed using a Cox proportional hazards model, adjusted for patient characteristics commonly associated with skin PsO and PsA development, including baseline age, sex, treatment (disease severity proxy), number of outpatient visits, number of inpatient hospital days, Charlson comorbidity index (CCI) (29), presence of rheumatic risk factors, including comorbid rheumatism (defined as at least one diagnosis of ICD-10 M79.0; see Table SII) (20), marital status, employment status, education level, county of residence, and index year. The proportionality assumption of the Cox proportional hazards model was assessed through a visual inspection of the Schoenfeld residuals. The exclusion of pre-existing PsO was removed in a sensitivity analysis to explore the impact of including cases of prevalent skin PsO.
Data management, statistical analyses and graphics, using the tidyverse collection of packages (30), were produced in R version 3.5.1(31). A 2-sided Type I error (alpha) of 0.05 was used for all statistical tests.
A total of 123,814 patients with skin PsO fulfilled the study’s inclusion and exclusion criteria and were retrospectively enrolled in the study. Of these, 110,118 (88.9%) received other treatment (mild skin PsO proxy), while 12,126 (9.8%) received conventional systemic treatment including phototherapy (distributed 4,793 to methotrexate, 2,328 to other conventional systemic treatment, and 5,005 to phototherapy) (moderate proxy), and 1,570 (1.3%) biologic or apremilast (distributed 1,554 to biologic, and 16 to apremilast) (severe proxy). As such, most patients in the severe group did receive biologic treatment.
Characteristics of the study population are shown in Table I. Overall, 51.8% of patients were female with a mean age of 54.8 ± 16.9 years, mean CCI score of 0.3 ± 0.9, mean number of outpatient visits 3.2 ± 4.6, and mean number of inpatient days 1.5 ± 7.8. Mean follow-up was 5.2 years ± 3.3 and maximum follow-up was 10.8 years. Proportionally, biologic-treated patients were more often younger, female, and had higher CCI scores than their counterparts receiving conventional systemic treatment and other treatment. Pre-index healthcare resource use and comorbid rheumatism was higher, but comorbid malignancy was less frequent. Conventional systemic-treated patients were more often male, and patients receiving other treatment were similar to the overall group. No other major differences were seen between the severity subgroups (defined by treatment proxy) in terms of patient characteristics.
Table I. Summary of patient characteristics
Incidence of psoriatic arthritis among adult patients with skin psoriasis
Across a total of 640,993 skin PsO patient-years at risk, 10,809 patients were diagnosed with PsA (8.7%) resulting in an unadjusted incidence rate of PsA in patients with skin PsO of 1.69 per 100 py (95% confidence interval (95% CI) 1.65–1.72), and 1.48 (95% CI 1.45–1.51), 3.00 (95% CI 2.87–3.13), and 5.49 (95% CI 4.94–6.04) per 100 py in those receiving other treatment, conventional systemic and biologic treatment, respectively. When combining patients receiving conventional systemic and biologic (moderate-to-severe proxy) in one group, the incidence rate of onset of PsA was significantly higher (3.23, 95% CI 3.10–3.36) than in patients receiving other treatment.
Association with risk factors
Unadjusted cumulative incidence (1-Kaplan–Meier) curves (Fig. 2) showed that patients receiving other treatment (mild skin PsO proxy) had the lowest risk of receiving the first observed PsA diagnosis, followed by patients receiving conventional systemic (moderate proxy) and biologic treatment (severe proxy). A log-rank test showed that the onset of PsA in biologic-treated, conventional systemic-treated, and other-treated subjects with skin PsO were significantly different from each other (p < 0.05).
Fig. 2. Cumulative incidence curves of time to onset of psoriatic arthritis (PsA) in patients with skin psoriasis (PsO) stratified by disease severity proxy. Cumulative incidence curves (calculated as 1-Kaplan–Meier) illustrating unadjusted time to onset of PsA in an adult incident skin PsO population stratified by disease severity proxy. Light-yellow curve represents patients receiving other treatment (mild skin PsO proxy); red curve represents those receiving conventional systemic treatment including phototherapy (moderate proxy) and dark-brown curve represents those receiving biologics or apremilast (severe proxy). The shaded area next to each curve represents the 95% confidence interval (95% CI). A risk table is included below the cumulative incidence curves, where the number of patients with incident skin PsO at risk (i.e. those with no onset of PsA or censoring event) are shown. Time to onset of PsA were fastest for biologic-treated patients with skin PsO, followed by patients with skin PsO receiving conventional systemic treatment, followed by those receiving other treatment. A log-rank test showed a statistically significant difference between the 3 curves.
Adjusted Cox proportional hazards regressions revealed higher risk of receiving a first observed PsA diagnosis in patients with skin PsO receiving biologics (hazard ratio (HR) 3.34, 95% CI 3.01–3.70) and conventional systemics (HR 2.03, 95% CI 1.93–2.14) (Table II), relative to those receiving other treatment. As a general trend, risk of receiving a first observed PsA diagnosis appears to be increasing alongside skin PsO disease severity defined using treatment as proxy. Women had a slightly higher risk of PsA, and many of the rheumatic risk factors were associated with increased risk of PsA diagnosis. The proportional hazards assumption did not appear to be violated.
Table II. Results of Cox proportional hazards model of time to onset of psoriatic arthritis in patients with skin psoriasis
Incident cases of skin PsO were identified instead of prevalent cases as the start of follow-up in the present study to better capture patients’ true time at risk. The use of prevalent cases of PsO in a sensitivity analysis resulted in similar findings (overall incidence rate 1.53 (95% CI: 1.50–1.56)) and no change in the direction or significance of the risk factors including disease severity proxy.
A 3-dimensional description of time to onset of PsA across treatment (disease severity proxy), sex and age for those with PsA events (Fig. 3) showed that young (20–40 years) and old (> 60 years) women receiving biologics had the shortest median time to onset of PsA: 0.62 and 0.56 years, respectively. The distribution of PsA events often comes soon after onset of PsO, and time to onset of PsA is similar for males and females except in young (20–40 years) and old (> 60 years) patients receiving biologic treatment. In the former group, onset is more consistent over time in females, but more consistent over time in males in the latter group.
Fig. 3. Distribution of time to onset of psoriatic arthritis (PsA) in patients with skin psoriasis (PsO) by disease severity proxy, sex and age. Violin plots illustrating the distribution of time to onset of PsA for those with PsA events stratified by disease severity proxy, sex and age. The box plot inside each violin plot displays the median, and the first and third quantiles. The upper line extends from the upper edge of the box to the largest value no further than 1.5 times the inter-quartile range (IQR, the distance between the first and third quartiles) from the box. The lower line extends from the lower edge of the box to the smallest value at most 1.5 times the IQR from the box. Data beyond the end of the lines are outliers and plotted individually as circles. Time to onset of PsA was fastest for biologic-treated female patients with skin PsO aged >60 years, followed by biologic-treated female patients with skin PsO aged 20–40 years, followed by biologic-treated male patients with skin PsO aged 20–40 years, and longest for male patients with skin PsO aged 20–40 years treated with conventional systemics or other treatment.
Reliable estimates of incidence of PsA in skin PsO and corresponding risk factors demonstrate burden of disease and can help guide physicians in identifying and tailoring treatment towards patients at risk. Most previous studies have assessed the incidence rate of PsA in PsO in much smaller cohorts of patients (1% or less of the present study’s sample size) (5, 11), with the exception of the study by Love et al. (12). In addition, a few population-based European studies of incident PsA in PsO exist, but none focuses on disease severity, including Love et al. (12, 14).
This large-scale retrospective cohort study of the entire Swedish population provides the first population study of incident PsA in 123,814 adult patients with skin PsO overall and by disease severity proxy, and association with risk factors. Contributing a total of 640,993 years of follow-up, a total of 10,809 (8.7%) incident PsA events were observed during the study period, resulting in 1.69 incident PsA cases per 100 py. Large differences in incidence rates were found between treatment subgroups, where the highest incidence rate was observed in patients receiving biologics or apremilast (severe disease proxy) (5.49 per 100 py), conventional systemic treatment including phototherapy (moderate proxy) (3.00 per 100 py), and other treatment (mild proxy) (1.48 per 100 py). The results add confidence to the middle range of previously reported estimates of incidence of PsA in patients with skin PsO (7) and confirm that the incidence rate of PsA is higher in patients with more severe disease (4, 5, 17–19).
In addition, many of the rheumatic risk factors were associated with a statistically significantly higher risk of a first observed PsA diagnosis, in line with previous literature (20). Relative to patients’ treatment, baseline characteristics, such as comorbidity, age and sex, were associated with risks of lower magnitude. However, these factors are still important, and the analysis of treatment as proxy of disease severity stratified by a wider age spectra (20–40, > 40–60, and > 60 years) and sex found that females receiving biologics aged > 60 and 20–40 years, respectively, were associated with the highest risk of receiving a first observed diagnosis of PsA. These findings were consistent with certain previous findings where females were associated with a higher risk of onset of PsA (16). Hypertension, diabetes mellitus, depression, anxiety, malignancy and coronary heart disease were the most common comorbidities in the overall study population. These are typical comorbidities of patients with skin PsO (22, 32).
The current study includes a wide patient population with complete coverage over a long follow-up, and a large set of risk factors predicting time to onset of PsA. The Swedish population-based data allows for a low risk of selection bias in the population at risk. Previous administrative database studies of prevalence and incidence of PsA in skin PsO commonly present lower incidence estimates compared with clinical registry studies (5). Patients with mild PsA may be under-represented in administrative databases, resulting in missing incident PsA events.
Study limitations
While the data used in the current study has many positive features, it is also associated with 3 key limitations. First, the study did not include time at risk in primary care, due to a lack of centralized primary care data in Sweden. Consequently, the skin PsO onset date recorded at a primary care facility was not included and, as such, it may be unclear when skin PsO onset occurred, resulting in an underestimate of patients’ actual time at risk, particularly for those with mild disease. The estimated incidence rate would probably be lower if it had been possible to identify patients with skin PsO earlier in primary care and follow them for a longer period of time. This is supported by a 10-times lower incidence rate reported in a study using UK primary care data (12).
Secondly, administrative secondary care data lacks direct measures of severity, such as the Psoriasis Area and Severity Index (PASI) and body surface area (BSA). The present study used treatments as proxies for disease severity, which has been done in previous research (26–28). The severity level was fixed at baseline, and future research should consider longitudinal updating of severity over time in order to understand the effects of severity dynamics on onset of PsA.
Thirdly, as this study uses observational diagnosis of PsA as the outcome, misclassification of PsA is a potential concern. Pathological overlap between osteoarthritis and PsA can make clinical differentiation impossible when patients present with joint pain. To aid in differential diagnosis, clinicians may test an osteoarthritis-indicated treatment where a lack of response may suggest that a diagnosis of PsA should be considered. Previous research has pointed to biologic testing to help in differential diagnoses, partially explaining why half of patients with PsA discontinue treatment with disease-modifying anti-rheumatic drugs within 2 years (33). The impact of this type of clinical scenario is that the date of diagnosis would be later for patients initially misclassified into non-PsA joint involvement diseases. There will also be scenarios where patients are never properly reclassified into PsA from, for example, osteoarthritis, which poses a limitation to the quality of the PsA endpoint used in this study.
As the study used Swedish data, generalizability of the results may be limited to settings that have similar patient characteristics, available treatments, and prescribing practices as the Swedish skin PsO population.
Conclusion
Psoriatic arthritis is a well-recognized comorbid condition to skin PsO, but the incidence rate is not well-established. This study suggests that close to 2 incident cases of PsA will occur across 100 patients per year. Physicians must be vigilant in screening patients with newly diagnosed skin PsO for important risk factors for onset of PsA during routine clinical follow-up, paying special attention to patients receiving biologics or apremilast, who probably have more severe skin PsO, and those with rheumatic involvement. The latter is not a typical skin symptom, highlighting the need to treat patients with psoriasis holistically.
This study was funded by Novartis Pharma AG.
Conflicts of interest: IL, ML and KG were employed by Quantify Research AB. KG was a board member and holder of stock options of Quantify Research AB. CR was employed by Novartis Pharma AG. AS was employed by KMK Consulting Inc. HT was employed by Novartis Pharmaceuticals Corporation. AO reports consulting fees from AbbVie, Amgen, Eli Lilly, LEO Pharma, MEDA AB, Novartis, Janssen Cilag, Celgen, Merck, UCB Pharma, Kiowa Kirin and Pfizer.


 Click to show fullsize
Click to show fullsize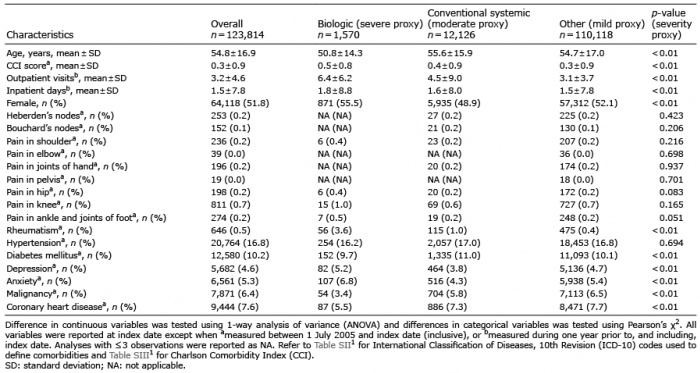 Click to show fullsize
Click to show fullsize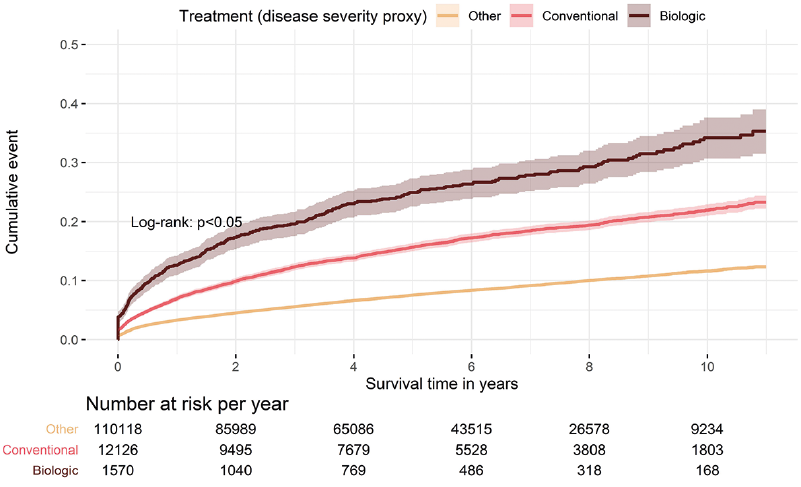 Click to show fullsize
Click to show fullsize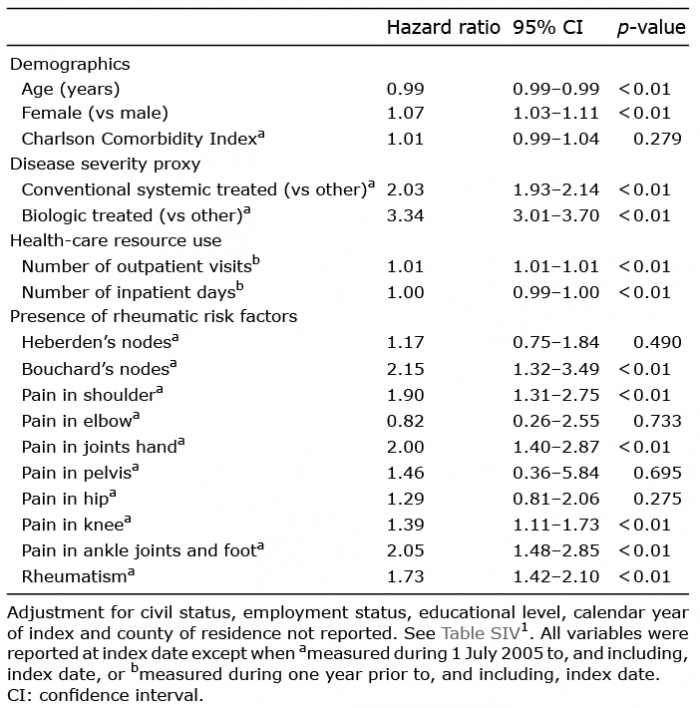 Click to show fullsize
Click to show fullsize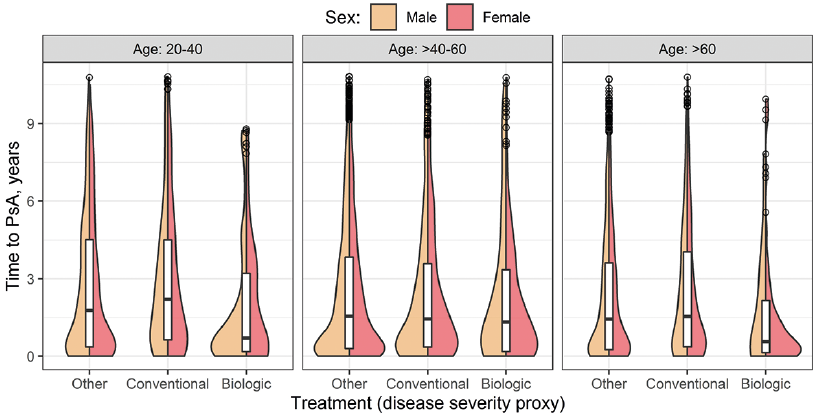 Click to show fullsize
Click to show fullsize