


1Department of Dermatology, University Hospital of Brest, Brest, 2EA 7449 REPERES (Pharmacoepidemiology and Health Services Research), Rennes 1 University, Rennes, Departments of Dermatology, 3University Hospital of Rennes, Rennes, 4University Hospital of Rouen, Rouen, 5University Hospital of Clermont-Ferrand, Clermont Ferrand, 66University Hospital of Nantes, Nantes, 7University Hospital of Dijon, Dijon, 8Hospital of Cornouaille, Quimper, 9AP-HP, Henri Mondor Hospital, Créteil, 10University Hospital of Avicenne, Bobigny, 11University Hospital of Bordeaux, Bordeaux, 12Victor Dupouy Hospital, Argenteuil, 13University Hospital of Bichat, Paris, 14Univeristy Hospital of Marseille, Marseille, 15Hospital of Niort, Niort, 16CUniversity Hospital of Saint Louis, Paris, 17University Hospital of Reims, Reims, and 18University Brest, Lien, Brest, France
#These authors contributed equally to this work.
Pruritus is a common symptom of bullous pemphigoid (BP), but has been poorly studied. The aim of this study was to analyse the characteristics of pruritus in patients with BP and its impact on their quality of life. A multicentre prospective observational study (in 15 French hospitals) was performed. A total of 60 patients were included, with a mean age of 77.4 years. Pruritus occurred daily in 85% of patients, with a mean pruritus intensity of 5.2/10. Tingling sensations were present in 72.4% of patients and burning sensations in 68.9%. Pruritus was exacerbated by stress, fatigue and xerosis. The mean ItchyQol score was 56.2/110 and the mean 5-D Itch Scale score was 16.5/25. The severity of pruritus was not related to age, sex, BP activity score, eosinophilia, or anti-BP230 and anti-BP180 autoantibodies. This study revealed that pruritus in BP is poorly tolerated and is an important cause of impaired quality of life.
Key words: pruritus; itch; bullous pemphigoid; quality of life; 5-D Itch Scale; ItchyQol.
Accepted Oct 6, 2020; Epub ahead of print Nov 2, 2020
Acta Derm Venereol 2020; 100: adv00320.
doi: 10.2340/00015555-3683
Corr: Emilie Brenaut, Department of Dermatology, University Hospital, FR-29609 Brest, France. E-mail: emilie.brenaut@chu-brest.fr
Pruritus is a major symptom of bullous pemphigoid, but has been poorly studied. This study provides data on pruritus in bullous pemphigoid. Pruritus occurred daily in 85% of patients, with a mean pruritus intensity of 5.2/10. A majority of patients reported associated sensations, such as sensations of tingling, burning and pain. Patient’s quality of life was greatly altered by pruritus. Dermatologists must take this observation into account and propose symptomatic treatments for pruritus if bullous pemphigoid treatment is not adequately effective against this symptom.
Bullous pemphigoid (BP) is the most common autoimmune blistering disease. The estimated incidence of BP ranges from 6 to 43 cases per million persons per year in Europe (1). The disease typically presents with bullous lesions over eczematous or urticarial patches associated with fierce pruritus. In approximately 20% of patients, the onset of BP is characterized by a non-bullous phase that can last weeks to months. Pruritus may be the only symptom of the pre-bullous stages of pemphigoid, justifying the search for BP in elderly patients with pruritus of unknown origin (2).
Pruritus is a frequent symptom in dermatology that can greatly alter the patient’s quality of life (3–6). It is a major symptom in BP, described as intense and disrupting sleep. However, no study has yet evaluated the clinical features of pruritus in BP. Better knowledge of the clinical features of pruritus in BP would increase understanding of its pathophysiology and improve patient care. The aim of the current study was to evaluate the characteristics of pruritus and its impact on quality of life in patients with BP.
Patients
This study was multicentre, prospective and descriptive. Patients were recruited from 15 dermatology departments in French hospitals during a 1-year period (October 2017 to October 2018).
Inclusion criteria were: age 18 years and older; newly diagnosed BP; presence of pruritus and normal cognitive functioning (defined by a Mini-Mental State Evaluation score of 21 or more). The diagnosis of BP was made in each centre according to the European Recommendations (7). Exclusion criteria were: adults not legally competent and pregnant women.
Data collection
Data were collected when BP was suspected by a dermatologist and before skin biopsy, treatment, etc. were initiated, in order to avoid any effects. The following data were collected: information about BP activity through the Bullous Pemphigoid Disease Activity Index (BPDAI) (8–10); positivity of anti-BPAG1 (BP230) and anti-BPAG2 (BP180) auto-antibodies by enzyme-linked immunoassay (ELISA) (> 9 U/ml for MBL kit, > 20U/ml for Euroimmun kit) and number of eosinophilic cells in the blood count. Localization of scratching lesions was noted.
The patients completed 4 questionnaires evaluating different dimensions of pruritus. The Brest Questionnaire has been used in other studies (11–13) and deals with chronology, intensity on the numerical rating scale (NRS), disruption of daily activities and characteristics of scratching.
The 5-D Itch Scale is a multidimensional questionnaire evaluating 5 components of pruritus: duration of pruritus each day; degree of pruritus from absent to unbearable; direction with evolution of the symptoms in the last 2 weeks; disability (sleep disruptions, social life, daily activities and work); and distribution (ranging from 5 to 25) (14).
Alteration in quality of life related to bullous disease was evaluated with the Autoimmune Bullous Quality of Life questionnaire (ABQOL), which contains 17 items about symptoms of bullous diseases, effects on daily activities, and effects on social relations and emotions. Each question has a score from 0 to 3 points, in which a higher score represents a lower quality of life (total score ranging from 0 to 51 points) (15).
The alteration in quality of life related to scratching was assessed with the Itchy Quality Of Life questionnaire (ItchyQoL). This questionnaire contains 22 items divided into 3 categories: symptoms, functional limitations, and emotions, and the total score ranges from 22 to 110 (16).
The primary objective of this study was to investigate the characteristics of pruritus in patients with BP. The secondary objective was to investigate the impact of pruritus on the quality of life of patients.
The study protocol was approved by a Jurisdictional Ethics Committee (Comité de Protection des Personnes 8 Ile de France, France). Written informed consent was obtained from all patients. The trial was registered on ClinicalTrials.gov, with the title “Clinical Characteristics of Pruritus and Evaluation of Quality of Life in Patients with Bullous Pemphigoid (PRURIPB)” and the identifier NCT03272958.
Statistical analysis
Characteristics of the pruritus were described using mean (standard deviation; SD) for quantitative variables and number (percentages) for qualitative variables. Univariate and multivariate linear regression models were used to assess the association of covariates with the continuous outcomes of the intensity of pruritus, the severity of BP and the quality of life, respectively, measured using the 5-D Itch Scale, the BPDAI and the ABQOL. The covariates examined were: sex, age, score on the 5-D Itch Scale, BPDAI, eosinophilia (as continuous variables), and positivity for anti-BP230 and anti-BP180 antibodies. Covariates with p-values less than 0.3 in the univariate analysis were included in the multivariate regression model. Due to a large amount of missing data for eosinophilia, anti-BP230 and anti-BP180 antibodies, these were not included as potential confounders in the multivariate analysis. For all statistical analyses the type 1 error was set at 5%. Statistical analysis was performed using RStudio Version 1.0.136 (RStudio Inc., Boston, MA, USA).
Demographic, clinical and biological data
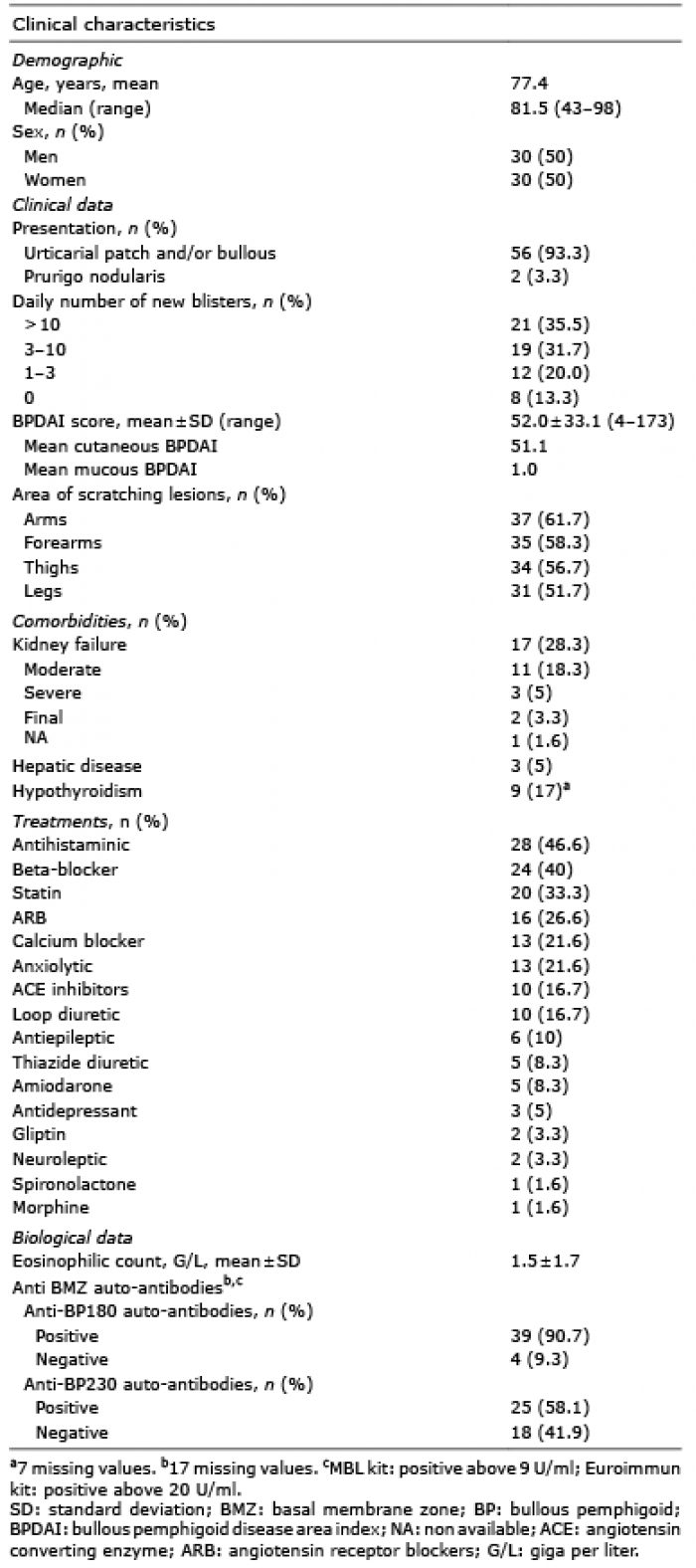
A total of 62 patients were included in the study, but 2 patients were excluded due to absence of pruritus. The demographic, clinical and biological characteristics of patients are shown in Table I.
Table I. Demographic, clinical and biological characteristics of patients with bullous pemphigoid (BP) (n = 60)
Characteristics of pruritus
Brest questionnaire. The data are presented in Table II. Symptoms occur more frequently in the evening and night than in the morning and afternoon, as shown in Fig. 1. Pruritus was associated with stinging sensations in 72.4% of patients and burning sensations in 68.9%. The other related sensory symptoms are shown in Fig. 2. The following parameters tended to exacerbate pruritus: stress, fatigue, xerosis, sweating, heat and specific clothes. Cold water tended to alleviate pruritus. Effects of different factors on pruritus are shown in Fig 3.
Table II. Characteristics of pruritus
Fig. 1. Frequency of pruritus in relation to time of day.
Fig. 2. Sensory symptoms associated with pruritus in patients with bullous pemphigoid.
Fig. 3. Effects of different factors on pruritus.
5-D Itch Scale. The mean 5-D Itch Scale score was 16.5 ± 4.3 (range 5–25). Approximately 60% of patients had pruritus for more than 6 h per day. The intensity of pruritus was mild in 3.3% of patients, moderate in 43.3%, high in 36.6% and unbearable in 16.8%. Pruritus delayed sleep and frequently woke 32.8% of patients. The most common locations of pruritus were the forearms (88.1% of patients), arms (86.4%), thighs (83.0%), back (77.9%) and legs (74.5%).
Quality of life
The mean ABQOL score was 14.9 ± 7.5 (range 3–30). The mean ItchyQol score was 56.2 ± 16.9 (range 25–93). The symptoms most described by patients as impacting their quality of life were the need to scratch (84.9%), sleep quality (56.6%), burning sensations (21.6%), pain (42.3%), and the presence of scars (41.1%). One-third of patients reported difficulties at work or during leisure activities due to pruritus, 13.3% found that scratching made them crazy, 18.2% felt irritable, 38.4% felt embarrassed by their itchy skin condition, and 6.6% reported that the pruritus affected their interactions with other people. More than a quarter of patients reported depressive symptoms linked to their pruritus.
Multivariate linear regression
A multivariate linear regression was performed to identify factors linked to the severity of pruritus in BP, the severity of BP and the alteration in quality of life (Table III). There was no correlation between severity of pruritus and age, sex, BPDAI score, eosinophil count or positivity of anti-BP230 and anti-BP180 antibodies. Only the eosinophilic count was associated with the severity of BP (evaluated with the BPDAI score) (coefficient 7.90; p = 0.002). Factors linked to the impact on quality of life (ABQOL) were analysed. Younger patients (coefficient –0.06 per year, p = 0.005), women (coefficient –1.43 for men, p = 0.004), and patients with intense pruritus (score on the 5-D Itch Scale) (coefficient 0.15, p = 0.004) had a greater alteration in their quality of life. There was no association between the alteration in quality of life and severity of BP (BPDAI) (coefficient –0.004, p = 0.57).
Table III. Factors associated with severity of pruritus, severity of bullous pemphigoid (BP) and alteration in quality of life
This study presents data about the characteristics of pruritus in BP and its impact on the quality of life of patients. The intensity of pruritus in the last 24 h in the patients with BP was rated 5.2/10 on the numerical rating scale (NRS). For comparison, the intensity of pruritus is estimated at 7–8/10 in atopic dermatitis (AD), 7/10 in urticaria, and 4–6/10 in psoriasis on the same measurement scale (17, 18). Thus, the intensity of pruritus can be considered moderate. However, any comparison with patients with other skin diseases should be made with caution, because the patients in the current study are older and may assess the intensity of their pruritus differently from younger patients, e.g. patients with AD. In this study, pruritus was increased by xerosis, so it may be important to use emollients in combination with BP treatment. As in psoriasis, pruritus was aggravated by heat, sweating, stress, and was more prominent in the evening (5, 19). In the current patients, the parts of the body affected by pruritus were mainly the upper arms, thighs and back, which are the locations where bullous lesions are most often found.
Autoimmune blistering diseases are known to disrupt patients’ quality of life (20). In a Polish study of 43 patients with BP, the mean ABQOL score was 16.3 ± 9.9, which is similar to that found in the current study (21). The burden of pruritus has been demonstrated in several studies (3–5, 11–13, 22). In a European study of 533 patients with various pruritic skin diseases, half of them indicated that their quality of life was often or always affected by chronic pruritus. The mean ItchyQol score in the patients with BP in the current study (56.2 ± 16.9) was lower than that in patients with AD (67.8 ± 20.6), prurigo nodularis (74.1 ± 15.4) or psoriasis (64.1 ± 18) (5), and similar to that in patients with Gougerot-Sjögren syndrome (57.3 ± 18) (22). However, the mean 5-D Itch Scale in the current patients (16.5 ± 4.3) was higher than in patients with severe AD (14.8 ± 2.9) (23). All the domains of quality of life were affected in the current patients: sleep, concentration and work, leisure, self-worth and, to a lesser extent, relationships. A high prevalence of depressive symptoms was recorded. In the current study, different questionnaires were used: some specific to BP (BPDAI and ABQOL) and others for pruritus in general (the validated 5-D Itch Scale and ItchyQol and the, not validated, Brest questionnaire).
A majority of patients patients reported nociceptive symptoms (e.g. stinging or burning sensations) associated with pruritus. In a recent study Rosen et al. (24) suggested that these symptoms were more frequent in inflammatory pruritus than in neuropathic pruritus. Nociceptive symptoms might be caused by inflammatory mediators acting on the cutaneous nerves. In addition, scratching may induce epidermal damage, including epidermal nerve alterations. Pain was associated with pruritus in 48.3% of patients, which is higher than in small-fibre neuropathies and psoriasis (17.6% and 17%, respectively) (12, 19), possibly because of post-bullous erosions. Pruritus concerned normal-looking localizations in 65% of the patients in the current study, which means that local inflammation might not be the only process involved. It could be caused by neural sensitization or circulating inflammatory mediators.
The pathophysiology of pruritus in BP seems to be related to various cytokines. Rüdrich et al. (25) founded a higher level of interleukin (IL)-31 in the blisters of patients with BP, which may trigger itch. Recently, Hashimoto et al. (26) demonstrated that severity of itch in BP correlated with rates of eosinophils, substance P (SP), neurokinin 1R (NK1R), IL-31RA, IL-13, periostin, and basophils. IL-17 could also play a role in BP pruritus, as has been shown in psoriasis. There is a high level of expression of IL-17 in BP lesions, leading to an amplification of the inflammatory response (27).
Study limitations
This study has some limitations. Patients with cognitive impairment were excluded because they could not provide reliable information about their pruritus. However, BP is more frequent in elderly people and patients with neurological disorders (28, 29). This could explain why the mean age of the study population was lower than that in the literature (77.4 vs 82.6 years in a French study cohort of 502 patients) (1). Antibody data were missing for 28.3% of patients. However, assay of BP180 and BP230 is not necessary to establish a diagnosis of BP in the presence of other specific clinical and pathological criteria (7). This could explain the lack of correlation between severity of BP and level of anti-BP180 antibodies in the current study.
Conclusion
This exploratory study revealed that intensity of pruritus is moderate in patients with BP. Pruritus is poorly tolerated and is the leading cause of impaired quality of life. Dermatologists should take this observation into account and propose symptomatic treatments for pruritus if BP treatment is not adequately effective with regards to this symptom (30).
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize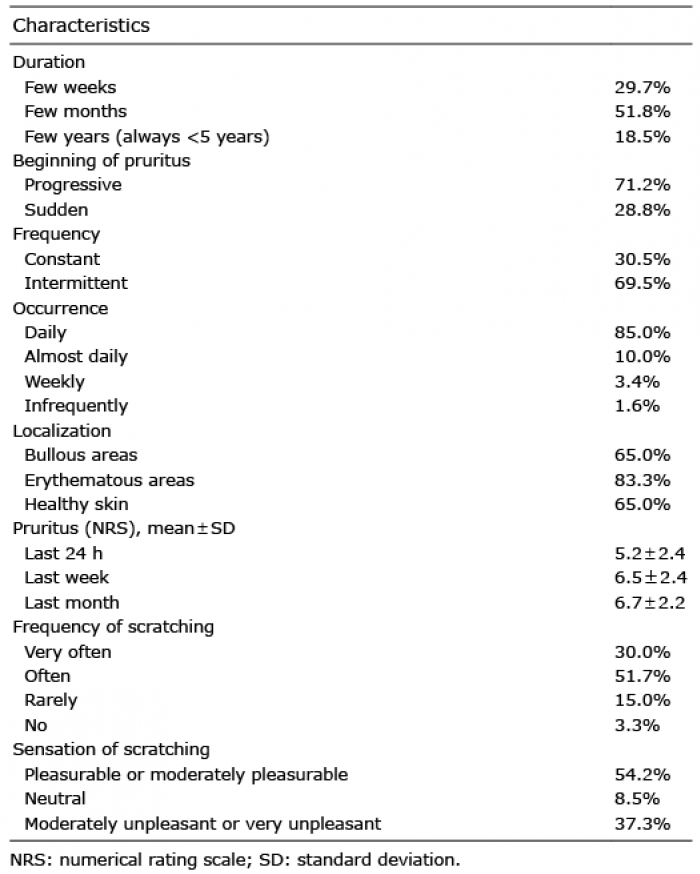 Click to show fullsize
Click to show fullsize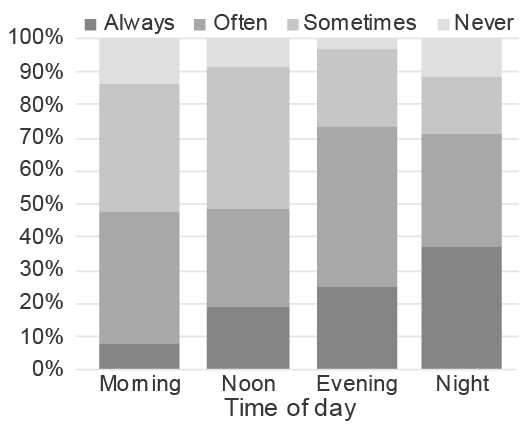 Click to show fullsize
Click to show fullsize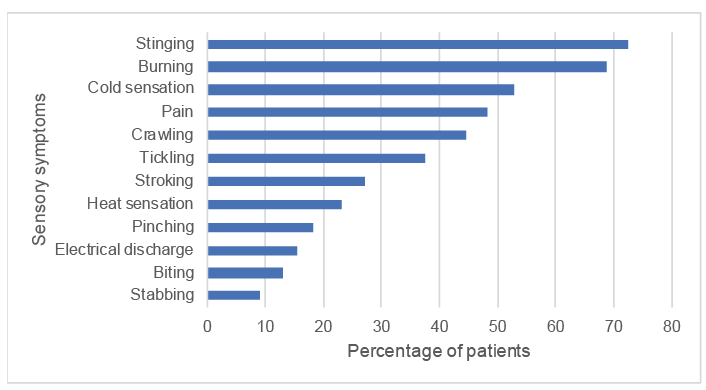 Click to show fullsize
Click to show fullsize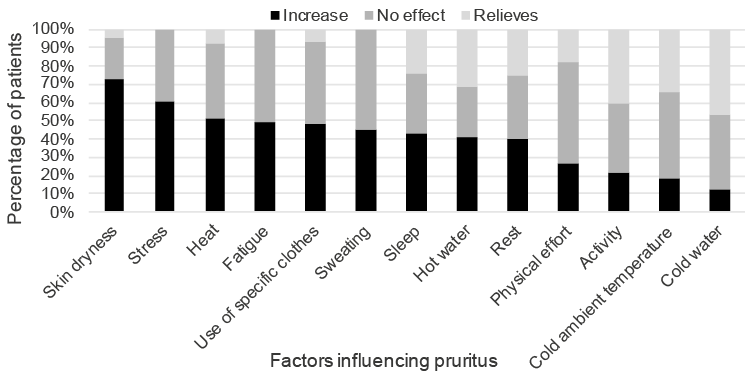 Click to show fullsize
Click to show fullsize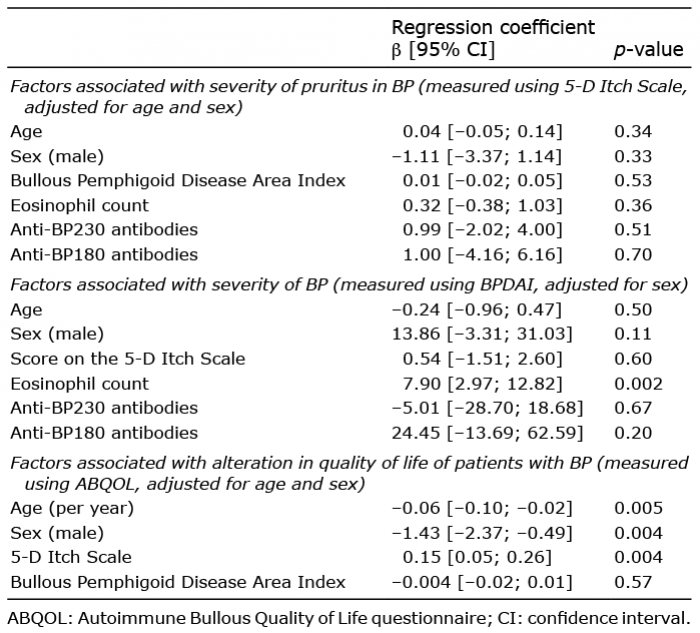 Click to show fullsize
Click to show fullsize