


1Second Department of Dermatology and Venereology, Cutaneous Lymphoma Outpatient Clinic, 3Department of Pathology and 5Laboratory of Biological Chemistry, Faculty of Medicine, Aristotle University of Thessaloniki, 2Department of Applied Informatics, University of Macedonia, Thessaloniki, Greece and 4Department of Gynecology and Obstetrics, Klinikum St. Marien Amberg, Amberg, Germany
This study investigated the expression of interleukin (IL)-17A, -17F and -22 in mycosis fungoides. Blood samples were collected from 50 patients with mycosis fungoides and 50 healthy controls. Skin samples were obtained from 26 patients with mycosis fungoides and 5 healthy controls. Protein levels of IL-17A, -17F and -22 were measured in serum by multiplex enzyme-linked immunosorbent assay, and mRNA expression levels were measured in blood and skin samples by real-time quantitative reverse transcription PCR. Both IL-17A and IL-17F mRNA expression levels were significantly lower in blood of patients with mycosis fungoides in comparison with healthy controls. IL-22 serum levels and expression levels of IL-22 mRNA in skin tissue, were significantly increased in patients with mycosis fungoides in comparison with healthy controls. These results suggest that low levels of IL-17A and IL-17F in mycosis fungoides may be connected to impaired immune surveillance contributing to tumourigenesis. Upregulation of IL-22 may play a role in the establishment of the tumour microenvironment in mycosis fungoides.
Key words: mycosis fungoides; primary cutaneous T-cell lymphoma; CTCL; IL-17A; IL-17F; IL-22.
Accepted Nov 4, 2020; Epub ahead of print Nov 10, 2020
Acta Derm Venereol 2020; 100: adv00326.
doi: 10.2340/00015555-3688
Corr: Despoina Papathemeli, Papageorgiou General Hospital, GR-56403 Efkarpia, Greece. E-mail: dpapathem@live.com
The role of interleukin-17A, -17F and -22 in many inflammatory and autoimmune diseases, including psoriasis, is well established. Little is known, however, about the role of these cytokines in mycosis fungoides. This study investigated the expression levels of interleukin-17A, -17F and -22 in blood and lesional skin samples of patients with mycosis fungoides in comparison with healthy controls. The results suggest that the mycosis fungoides tumour microenvironment is characterized by downregulation of interleukin-17A and -17F and upregulation of interleukin-22.
Mycosis fungoides (MF), with an incidence of 0.4–0.5/100,000 people per year, is the most common type of primary cutaneous T-cell lymphoma (CTCL) (1). In early stages the disease presents clinically with limited patches or plaques in a bathing suit distribution (lower trunk, buttocks, groin, axillae, breasts). Early-stage MF is characterized by an uneventful disease course and a favourable prognosis; nevertheless early-stage MF can progress to advanced disease in 25% of cases (2). In advanced stages of MF patients may develop skin tumours or erythroderma, lymph node or visceral spread, and blood involvement, resulting in a poor prognosis (3).
The exact pathogenetic mechanism and the cytokine interplay that occurs in the MF microenvironment is unknown. In early-stage MF, the skin shows a Th1 cytokine pattern characterized by normal-to-increased expression of interferon (IFN)-γ, interleukin (IL)-2 and IL-12, whereas in late-stage MF, there is a loss of Th1 cytokines and an increase in Th2 cytokines (IL-4, IL-5, IL-10 and IL-13). This could be partially explained by the predominance of CD8+ T cells in early stages of the disease, which exhibit a Th1 phenotype and contribute to an anti-tumour response, while in advanced stages the increased number of malignant CD4+ T cells leads to Th2 skewing (4). However, little is known about the role of Th17 and Th22 and their related cytokines in MF.
Th17 cells are a distinct class of T-helper lymphocytes, which play a role in the immune defence, fighting pathogens that cannot be managed by Th1 and Th2. Th17 cells produce IL-17A, IL-17F as well as IL-21, IL-22 and granulocyte-macrophage colony-stimulating factor (GM-CSF) (5). The Th17 lineage is implicated in a number of autoinflammatory disorders, including psoriasis, rheumatoid arthritis, multiple sclerosis and inflammatory bowel disease (5, 6). Th22 is a relatively new class of CD4+ T cells with specific characteristics: they produce IL-22, IL-13 and tumour necrosis factor (TNF)-α, but not IL-17 or IFN-γ (7, 8). Th22 cells affect mesenchymal and epithelial cells and play a role in inflammatory skin conditions, such as atopic dermatitis (6).
Both Th17 and Th22 play an important role in the skin. Irritated epithelial keratinocytes produce IL-1β and IL-6 and stimulate intraepidermal Langerhans cells and dermis-resident dendritic cells to produce IL-23 and migrate to lymph nodes, where Th17 and Th22 differentiate responsively to the antigens presented to them by the antigen-presenting cells (APCs) and migrate to sites of inflammation in the skin. Skin-homing Th17 and Th22 produce IL-17A, IL-17F, IL-22 and TNF-α, which in turn activate keratinocytes to produce cytokines (IL-32 and IL-36), chemokines (CXCL1 and CCL20) and antimicrobial peptides (HBD-2 and S100A7/psoriasin and S100A15/ koebnerisin) that induce local inflammatory reactions (9, 10).
Apart from Th cells, another cellular source of IL-17A, IL-17F and IL-22 are type 3 innate lymphoid cells (ILC3), which are part of the innate immune system. Both IL-17A/F and IL-22 can be produced by ILC3 simultaneously or separately (11). Recent experimental studies indicate the presence of ILC3 in psoriatic skin (12–14). However, their function in the cutaneous immune network is ill-defined and relatively unexplored.
The role of Th17 producing IL-17A, IL-17F and IL-22 in the pathogenesis of psoriasis is well known (15). In the psoriatic skin, IL-22 is also produced by Th22 cells and increased production of IL-22 receptor is observed (16, 17). In line with Th cells, ILC3 are also accumulated in peripheral blood, lesional and non-lesional skin of patients with psoriasis (12–14). Patients with psoriasis are at increased risk of developing CTCL (18, 19). Assuming that this may be caused by a common pathogenetic pathway, it was considered that it would be of great scientific interest to investigate the expression of IL-17A, IL-17F and IL-22 in patients with MF.
Peripheral blood and skin tissue samples
Peripheral blood samples were obtained from 50 patients with MF and 50 healthy controls. Skin tissue samples were obtained from 26 patients with MF and 5 healthy controls. Samples were collected from newly diagnosed patients with MF and from patients with a previous history of MF with active disease despite treatment. Patients with a history of MF, but in full remission, were excluded. Healthy controls had no history of autoimmune or malignant disease. Samples were collected during daily clinical practice in our facilities. Informed consent was obtained from all patients and healthy controls. The study was approved by the bioethics committee of Aristotle University of Thessaloniki, Greece, and was conducted according to the principles of the Declaration of Helsinki.
Enzyme-linked immunosorbent assay
IL-17A, IL-17F and IL-22 protein levels in sera were measured using Milliplex® MAP technology. Th17 Magnetic Bead Panel kit was obtained from Merck, Millippore, USA, and the procedure was performed according to the manufacturer’s instructions. Results were acquired by Luminex® xPONENT® acquisition software using Luminex® 200™ System (Luminex Corporation, Austin, Texas, USA).
Real-time quantitative reverse transcription PCR assay
The mRNA expression levels in blood and skin tissue were measured with real-time quantitative reverse transcription PCR (RT-qPCR). RNA isolation was performed using Nucleospin RNA kit (Macherey-Nagel GmbH & Co. KG, Düren, Germany). cDNA was synthesized from 500 ng total RNA, using PrimeScript 1st strand cDNA synthesis kit (TaKaRa Bio Inc, Japan). RT-qPCR was performed in the StepOnePlus™ Real-Time PCR System (Applied Biosystems) using SybrGreen-based technology (2x qPCRBIO SyGreen Mix Hi-ROX, PCR BIOSYSTEMS, UK) and the following primers: IL-17A: forward 5’-AACCTGAACATCCATAACCGG-3’ and reverse 5’-ACTTTGCCTCCCAGATCAC-3’, IL-17F: forward 5’-GTGCCAGGAGGTAGTATGAAGC-3’ and reverse 5’-ATGTCTTCCTTTCCTTGAGCATT-3’, IL-22: forward 5’-AGTGCTGTTCCCTCAATCTG-3’ and reverse 5’-CTGTGTCCTTCAGCTTTTGC-3’ (product sizes 139bp, 200bp and 149bp, respectively). GAPDH was used as a reference gene and amplified using primers: forward 5’-AGCCACATCGCTCAGACACC-3’ and reverse 5’-GCGCCCAATACGACCAAATCC-3’ (product size 67 bp). Cycling conditions included an initial polymerase activation cycle at 95oC for 2 min, followed by 40 cycles of denaturation at 95oC for 5 s, and anneal/extension at 60oC for 20 s. The specificity of the products was assessed by melting curve analysis and/or agarose gel electrophoresis. The relative quantity of mRNA expression was calculated by the 2–ΔCT[2–(CTgene of interest–CTreference gene)] method (20).
Statistical analysis
To investigate differences in mean values for the protein/mRNA levels of the interleukins of interest between patients and controls, statistical tests were applied to reject the null hypothesis of equality. Because of the skewed nature of the current data, parametric tests were performed assuming that the logarithmically transformed observations follow a normal distribution. For the mRNA expression levels, where all observations were recorded as numerical values, the p-values of a 2-sided t-test were calculated, using the Welch approximation. Regarding the enzyme-linked immunosorbent assay (ELISA) concentration data, where the current data contained a considerable percentage of cases in which the record was that there was a lower than laboratory detection limit value, a parametric log-normal likelihood ratio test for left-censored data was applied, which is the reciprocal of the above usual t-test. Software to implement the latter method is available through the free statistical language R, from the NADA and EnvStat packages (21). A valuable guide to the methods is provided in documentation from USEPA and R packages (22, 23). To validate the current results, exploratory work examined that the log-normal model assumption was fulfilled satisfactorily and the findings were compared with alternative procedures.
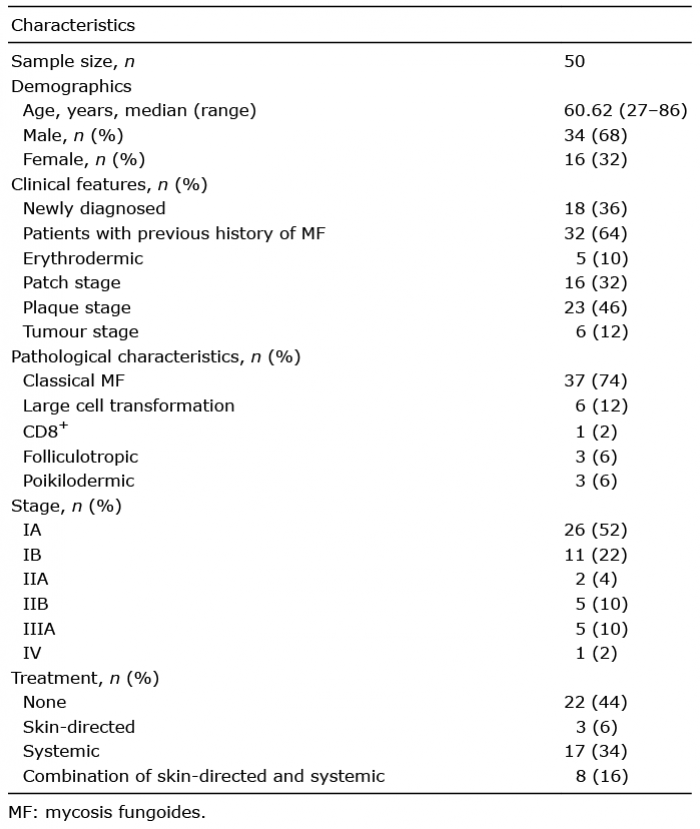
Demographic and clinical characteristics of patients recruited in this study
A total of 50 patients with MF were recruited (n = 50, median age 60.6 years). Among them 34 were male and 16 female, 16 cases had patch-stage disease, 23 cases had plaques, 6 cases tumours, and 5 patients were erythrodermic. Furthermore, the current sample comprised 39 patients with early-stage MF (IA–IIA) and 11 patients with advanced-stage MF (IIB–IV). All patients had LDH serum levels within normal reference range. Twenty-two patients had not received any treatment prior to sample collection. The remaining patients had received skin-directed or systematic treatment, or a combination of those, depending on the disease status. Skin samples from punch/incisional biopsies were collected from 26 consenting patients undergoing biopsy for diagnostic/re-evaluation purposes and were included in the study after histological confirmation of the disease. The demographic and clinical characteristics of the patients are listed in Table I.
Table I. Patients’ characteristics
Serum levels of interleukin-17A, -17F and -22 measured by ELISA
There was no statistically significant difference between serum levels of IL-17A and IL-17F, measured by ELISA, between patients and healthy controls (p = 0.0720 and p = 0.6600, respectively). However, serum levels of IL-22 in patients were significantly higher than in healthy controls (p = 0.0076) (Fig. 1 and Table II). No statistically significant difference in IL-17A, IL-17F and IL-22 serum levels in patients was found between males and females, between early- and advanced-stage patients and between patients at different clinical stages (patch, plaque, tumour, erythroderma). Patients who had received skin-directed therapy had higher levels of IL-17F in comparison with patients under systemic treatment, under combination treatment and under no treatment at all (p = 0.0250). However due to the small sample size (only 3 patients received skin-directed therapy), this result is very doubtful.
Fig. 1. Serum protein levels of interleukin (IL)-17A, IL-17F and IL-22 in patients vs controls. *: Sample mean. Horizontal line: non-detection limit.
Table II. Descriptive statistics (maximum likelyhood estimates) and statistical significance for equality regarding serum protein levels of interleukin (IL)-17A (pg/ml), IL-17F (ng/ml) and IL-22 (ng/ml), detected by enzyme-linked immunoassay (ELISA)
Expression levels of interleukin-17A, -17F and-22 mRNA in blood samples measured by RT-qPCR
IL-17A and IL-17F mRNA expression levels were significantly lower in the blood samples from patients in comparison with healthy controls (p = 0.0089 and p = 0.0004, respectively). There was no statistically significant difference in IL-22 mRNA expression in blood between patients and healthy controls (p = 0.7308) (Table III and Fig. 2). No statistically significant difference in IL-17A, IL-17F and IL-22 mRNA expression levels in blood samples from patients was found between males and females, between early- and advanced-stage patients, between patients with different clinical stages (patch, plaque, tumour, erythroderma) and between patients under different treatment regimens (skin-directed therapy, systemic therapy, both skin-directed and systemic therapy and no therapy at all).
Table III. Descriptive statistics and statistical significance for equality regarding mRNA expression levels (relative quantity; RQ) of interleukin (IL)-17A, IL-17F and IL-22 in blood samples, assessed by Real-time quantitative reverse transcription PCR assay
Fig. 2. mRNA expression of interleukin (IL)-17A, IL-17F and IL-22 in blood samples from patients vs controls. *: Sample mean. RQ: relative quantity.
Expression levels of interleukin-17A, -17F and -22 mRNA in skin tissue samples measured by RT-qPCR
There was no statistically significant difference in IL-17A and IL-17F mRNA expression levels in skin tissue samples, measured by RT-qPCR, between patients and controls (p = 0.3641 and p = 0.6925, respectively). However, expression levels of IL-22 mRNA in skin tissue were increased in samples from patients with MF in comparison with healthy controls (p = 0.0319) (Table IV and Fig. 3). No statistically significant difference in IL-17A, IL-17F and IL-22 mRNA expression levels in skin tissue from patients was found between males and females, between early- and advanced-stage patients, between patients with different clinical stages (patch, plaque, tumour, erythroderma), or between patients under different treatment regimens.
Table IV. Descriptive statistics and statistical significance for equality regarding mRNA expression levels (relative quantity; RQ) of interleukin (IL)-17A, IL-17F and IL-22 in skin tissue samples, assessed by Real-time quantitative reverse transcription PCR assay
Fig. 3. mRNA expression of interleukin (IL)-17A, IL-17F and IL-22 in skin tissue samples in patients and controls. *: Sample mean. RQ: relative quantity.
The exact role of Th17, Th22, ILC3 and the associated cytokines in the immune dysfunction observed in MF have not yet been fully elucidated. IL-17A and IL-17F mRNA expression levels in blood samples in this study were significantly lower in patients with MF, in comparison with healthy controls. Furthermore, elevated IL-22 protein levels were detected in the serum of patients, as well as elevated IL-22 mRNA expression in skin tissue samples of patients, in comparison with healthy controls. These data suggest that MF unbalanced immunity may be characterized by downregulation of IL-17A and IL-17F and upregulation of IL-22.
There are very few studies of the concentration of IL-17A, IL-17F and IL-22 in blood or skin samples of patients with MF, and these studies often present conflicting results. The current findings are consistent with those from a study from Miyagaki et al. (24) in 2011, who demonstrated that IL-22, but not IL-17A and IL-17F, were significantly elevated in lesional skin of CTCL. In the same study, serum IL-22 levels were increased in patients with CTCL and correlated with disease severity. In the current study, however, neither IL-22 levels in serum nor IL-22 mRNA expression in blood and lesional skin tissue correlated with disease severity. In 2013 a case of Sézary syndrome was reported, characterized by high levels of circulating IL-22-producing CD8+ tumour cells under a condition of bacterial sepsis (25). The lack of IL-17 in lesional skin of CTCL has been observed in a study by Wolk et al. (26), in which it was demonstrated that the increased skin infection risk in patients with MF is associated with impaired upregulation of antibacterial proteins (ABPs), and that IL-17A and IL-17F deficiency may be responsible for this. Furthermore, in a study from Ciree et al. (27) in 2004, 5 out of 10 MF/SS biopsies expressed IL-17 mRNA, whereas this cytokine was absent in normal skin. IL-17 mRNA was not detected in the biopsies from 2 patients with initially localized MF, whereas upregulation of IL-17 was demonstrated during disease progression. Similarly, Krejsgaard et al. (28) found that, IL-17A and IL-17F mRNA expression was significantly increased in CTCL skin lesions compared with healthy donors and patients with chronic dermatitis, but patients with MF displayed a considerable heterogeneity in IL-17A and IL-17F expression, and the level of expression was higher in advanced-stage disease. Furthermore, IL-17F expression was associated with progressive disease. In a previous study by the same group in 2011, IL-17 protein was detected by immunohistochemistry in 10 out of 13 examined skin lesions, but not in the sera from 28 patients with CTCL, using ELISA (29). In another study Chong et al. (30) detected by qPCR elevated IL-17 levels in stimulated peripheral blood mononuclear cells (PBMCs) from early MF/CTCL and late MF/CTCL without blood involvement (−B) compared with PBMCs from normal, psoriasis and MF/CTCL with blood involvement (+B). PBMCs from late MF/CTCL with blood involvement (+B) had the lowest levels of IL-17 of all groups.
Studies that have attempted to characterize IL-17A, IL-17F and IL-22 involvement in MF have various results. This could be interpreted by differences between research groups in the study population and controls, in the samples included (skin biopsies, PBMCs, peripheral blood) and the different methodologies and techniques used (ELISA, immunohistochemistry, mRNA expression). A major weakness of the above studies is that they all have small sample sizes due to the rarity of the disease.
The low levels of IL-17A and IL-17F mRNA expression in blood in the current study might reflect the defective host anti-tumour immune response. Th17 cells and their innate equivalent natural cytotoxicity receptor– (NCR–) ILC3 cells produce IL-17, which possesses both pro-tumourigenic and anti-tumourigenic functions (11, 31). Moreover, Murray et al. (32) have demonstrated that IL-17 is produced, not only, by malignant T-cells, but also by non-malignant tumour-infiltrating lymphocytes (TILs) in MF, and that expression of IL-17 decreases during disease progression. The high production of IL-17 from TILs reflects the role of IL-17 in host anti-tumour immunity. IL-17A and IL-17F might play a crucial role in immune surveillance and a decrease in these cytokines may lead to disease progression. This hypothesis is reinforced by reports of psoriatic patients who developed MF after short-term treatment with the IL-17A antibodies secukinumab and ixekizumab (33–35).
The current findings of elevated IL-22 protein levels in serum and IL-22 mRNA expression in skin tissue raise questions about the possible role of IL-22 in the pathogenesis of MF. IL-22 is involved in the modulation of tissue responses during inflammation and plays a role in many inflammatory skin conditions, such as atopic dermatitis and psoriasis (16). IL-22 is also important for maintaining epithelial integrity and for protection against pathogens (36, 37), thus exerting an anti-tumour role. Although Th17 and Th22 are the foremost source of IL-22, recently published data have shown that this cytokine is also produced in the skin by NKp44+ (NCR+) ILC3 cells. ILC3 cells have a dual role in tumourigenesis. They present an anti-tumour effect by releasing TNF and promoting leucocyte recruitment and they also increase tumour growth and tumour cell mobility through IL-22 secretion and STAT3 signalling (38). IL-22 mRNA levels in tissue samples in the current study were not correlated with disease stage, thus we cannot draw conclusions about the prominent role of IL-22 in the development and evolution of MF. Adding to complexity, IL-22 effect can be neutralized by IL-22-binding protein (IL-22BP), which binds free IL-22 (37). Dysregulation of IL-22 expression and signalling has been observed in many common cancers, such as colon, lung and liver cancer. IL-22 receptor is expressed on epithelial cells of the skin, the gastrointestinal tract and the respiratory tract, but not on immune cells. This restricted tissue specificity makes IL-22 a promising future therapeutic target, probably with fewer side-effects (39). Further research is needed to evaluate the potential therapeutic benefit of targeting IL-22 in MF.
Study limitations
A limitation of this study is the small sample size, which might explain the fact that IL-17A and IL-17F downregulation in patients with MF was detected only by mRNA expression level in the blood, and not by protein level in serum or mRNA expression level in skin tissue. Similarly, IL-22 showed significant upregulation in mRNA expression level in skin tissue and in protein level in the serum of patients in comparison with healthy controls, but not in mRNA expression in the blood. Another reason for this discrepancy is that concentration levels of these cytokines, especially in the blood, are very low and cannot easily be detected. In the current study many concentration values in the ELISA were below the detection limit, and survival analysis statistical methods for left-censored data had to be used to overcome this limitation. A further limitation of the current study is the lack of functional data on possible molecular and cellular mechanisms that would explain these immune dysregulations, which would further support the current findings.
Conclusion
The results of this study suggest that the MF tumour microenvironment is characterized by downregulation of IL-17A and IL-17F and upregulation of IL-22. At present it is not known whether these cytokine expression abnormalities are directly responsible for the pathogenesis of the disease, are signs of an ineffective host immune response, or are epiphenomena to the underlying neoplastic mechanisms (40). However, by understanding how cytokine signalling in the tumour microenvironment influences malignant T cells, it might be possible to develop new targeted therapies in the future (41). Additional multi-centre studies including a larger number of patients are needed to further elucidate the cytokine imbalances and immune dysregulation that occur in MF.
This study was funded by the General Secretariat for Research and Technology (GSRT) of Greece and the Hellenic Foundation for Research and Innovation (HFRI).
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize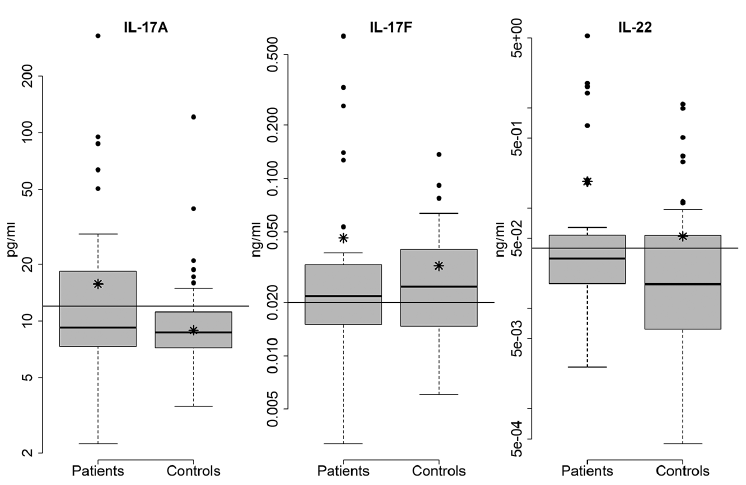 Click to show fullsize
Click to show fullsize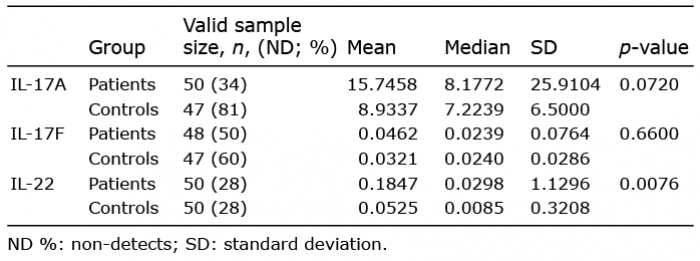 Click to show fullsize
Click to show fullsize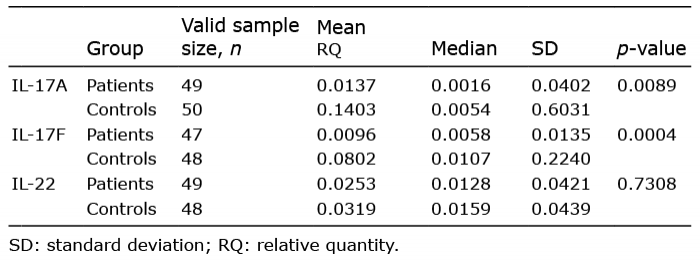 Click to show fullsize
Click to show fullsize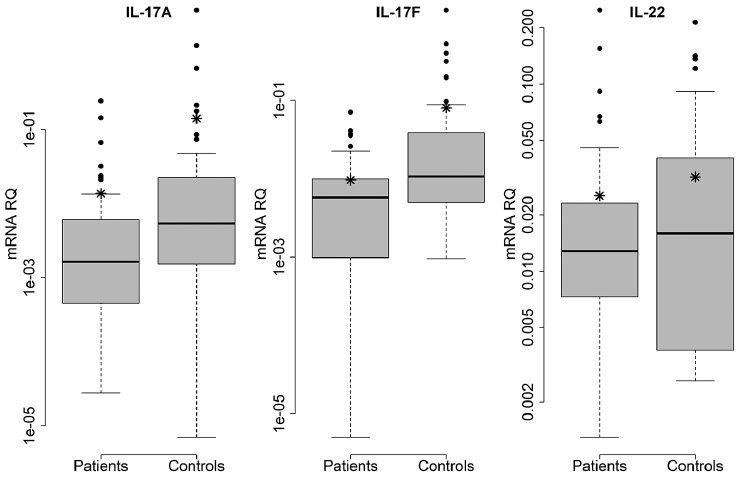 Click to show fullsize
Click to show fullsize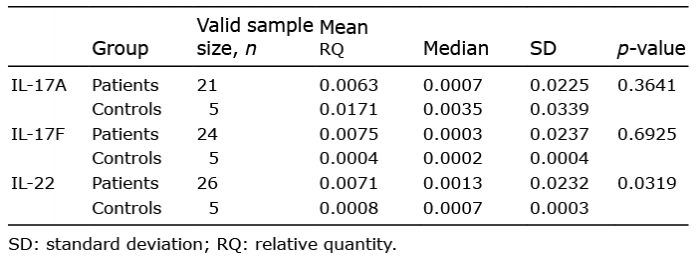 Click to show fullsize
Click to show fullsize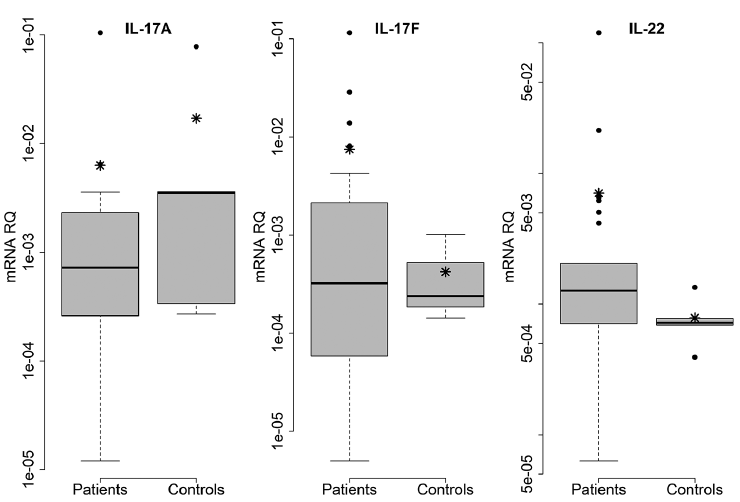 Click to show fullsize
Click to show fullsize