


1Center for Dermatooncology, 3Division of Dermatopathology and 4Division of Dermatosurgery, Eberhard Karls University, Tuebingen, Germany and 2Department of Dermatology, Koc University Hospital, Istanbul, Turkey
Electrical impedance spectroscopy is a non-invasive technique that can help clinicians in diagnosing malignant skin tumours. Depending on the cellular irregularity of the lesion, electrical impedance spectroscopy can reveal changes in the structure and form of the cells, using a harmless electrical current applied to the skin. A score between 0 and 10 is generated by the electrical impedance spectrometer, where 0 is considered benign and 10 is malignant. This prospective study was conducted in 101 patients with a total of 200 skin lesions; 62 benign and 138 malignant. There was a significant difference between the electrical impedance of malignant and benign lesions (p < 0.001). The sensitivity, specificity, positive predictive value and negative predictive value of electrical impedance spectroscopy for non-melanoma skin cancer were 94.2%, 41.9%, 78.3% and 76.5%, respectively, when the cut-off for the electrical impedance spectroscopy score was set between 5 and 6. The area under the curve in receiver operating characteristics analyses was 0.758.
Key words: electrical impedance spectroscopy; non-melanoma skin cancer; sensitivity and specificity.
Accepted Nov 4, 2020; Epub ahead of print Nov 10, 2020
Acta Derm Venereol 2020; 100: adv00328.
doi: 10.2340/00015555-3689
Corr: Claus Garbe, Center for Dermatooncology, Department of Dermatology, Eberhard Karls University, Liebermeisterstraße 25, DE-72076
Tuebingen, Germany. E-mail: claus.garbe@med.uni-tuebingen.de
The development of non-invasive diagnostic tools for skin cancer is an important topic for researchers. The objective of this study was to evaluate the diagnostic accuracy, sensitivity and specificity of use of an electrical imped-ance spectroscopy technique in non-melanoma skin cancer. Electrical impedance spectroscopy was able to distinguish between benign and malignant skin lesions. The results of this study suggest that electrical impedance spectroscopy measurements can improve diagnostic performance with a high sensitivity in detection of non-melanoma skin cancer.
The incidence rate of non-melanoma skin cancer (NMSC) is increasing worldwide in white populations (1). Mortality caused by the disease, comorbidities, cost and time loss during follow-up and treatment period raise the importance of early diagnosis. The development of non-invasive tools for the early diagnosis of skin cancer has attracted the attention of researchers in recent years (2).
Electrical impedance spectroscopy (EIS) is a non-invasive, rapid method for evaluating malignant skin lesions. The electrical properties of cutaneous tissue vary, depending on cell size, shape, density, and membrane structure. Malign transformation of the cells affects the capacity of a tissue to conduct and store electricity, and this can be detected by EIS technique (3). Although EIS was developed as a diagnostic decision support tool for early detection of melanoma, the same mechanism can be applied to NMSC and benign lesions (4, 5).
This pilot study aimed to test whether EIS can also be used to diagnose NMSC. The objective of the study was to evaluate the diagnostic accuracy, sensitivity, and specificity of EIS in NMSC.
Study population and design
This pilot study focused on the diagnosis of NMSC, mainly basal cell carcinoma (BCC) and squamous cell carcinoma (SCC). In addition, lesions with a clinical pre-diagnosis of sarcoma, melanocytic naevi, benign epithelial or dermal tumours were included. Patients ≥ 18 years old, with benign or malignant skin lesions excised for diagnostic or therapeutic purposes in the Department of Dermatology at University Hospital of Tuebingen were enrolled into this prospective study. EIS diagnostics were performed in the operating room. All tumours were examined histopathologically. Patients with suspicious lesions of melanoma, lesions located on acral skin, genitalia, mucosal surfaces, bony areas, under nails, lesions with foreign material (e.g. a tattoo or splinters), or lesions located on acute sunburn were excluded. The study was approved by the Ethics Commission of the Medical Faculty at the University of Tuebingen (protocol number: 183/2019BO1).
Electrical impedance was measured with the NevisenseTM system (SciBase, Stockholm, Sweden) using a handpiece containing a disposable 5 bar electrode on the distal part. Before each measurement, lesions were moistened for 30 s with physiological saline solution. The electrode penetrates the stratum corneum with 150 µm gold-coated pins, which apply an electrical current to the skin and receive the return current from the tissue. The electrical resistance and reactance of the skin is measured at 35 different frequencies, logarithmically allocated between 1 kHz and 2.5 MHz, at 4 different depths, utilizing 10 permutations (3, 6). The infiltration depth of the electrical current applied by the electrode is up to 2.5 mm (7). Depending on the cellular irregularity of the lesion, a score of between 0 and 10 is created by the device, where 0 is considered as benign and 10 as malignant. For each lesion one or more measurements were performed, depending on the size of the lesion. Multiple measurements were required for lesions greater than 5 × 5 mm2, which is the surface area of the electrode.
The accuracy of EIS was evaluated, comparing the scores with histopathological diagnosis, which is regarded as gold standard. Histopathological examination was performed by dermatopathologists at the dermatology department.
Actinic keratosis has been shown to have similar histopathological and mutational changes to those of invasive SCC and is considered to be the earliest stage of SCC in situ (8–11). Therefore, actinic keratosis was classified as a subgroup of SCC in the malignant tumours.
Statistical analyses
Statistical analyses were made to define the sensitivity, specificity, positive predictive value (PPV) and negative predictive value (NPV) of the EIS method. The receiver operating characteristics (ROC) and the area under the curves were calculated to determine the optimal cut-off values of the EIS score in order to report sensitivity and specificity. The electrical spectroscopy measurements were recorded as true-positive (correct diagnosis of NMSC), true-negative (correct rejection of NMSC), false-positive (incorrect diagnosis of NMSC) and false-negative (missed diagnosis of NMSC). Formulae for calculating the diagnostic accuracy were as follows:
For not normally distributed samples, correlation was evaluated with Spearman rho correlation analyses, and Mann–Whitney U test was performed for comparing the scores of the groups. Statistical analyses were performed with SPSS Statistics Version 26.0 (Statistical Package for Social Sciences, SPSS Inc., Chicago, IL, USA). Throughout the analyses, p-value < 0.05 was considered statistically significant.
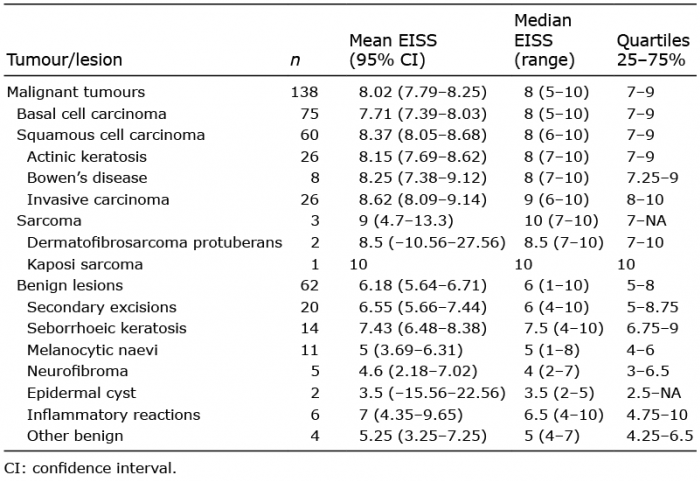
A total of 200 lesions excised in the operating room were included in the study. Lesions were obtained from 101 patients (67 males (66.3%) and 34 females (33.7%)). The mean age of the patients was 71.97 ± 13.4 years, with a median of 76 (minimum 25, maximum 96) years. A total of 138 (69%) lesions were malignant and 62 (31%) were benign. Malignant tumours were categorized as BCC, SCC and sarcoma; benign lesions were categorized as secondary excisions, seborrhoeic keratosis, melanocytic naevus, neurofibroma, epidermal cyst, inflammatory reaction and other benign lesions. EIS scores according to tumour group are summarized in Table I.
Table I. Electrical impedance spectroscopy score (EISS) according to the tumour/lesion groups
The EIS mean score ± standard deviation (SD) was significantly (p < 0.001) lower in benign lesions (6.18 ± 2.1) than malignant tumours (8.02 ± 1.3). There was no statistically significant difference in EIS scores between BCC and SCC (p = 0.72). For malignant tumours, the median EIS scores ranged between 5 and 10. Nearly all epithelial malignant tumours had median EIS of 8; only invasive SCC had a median EIS of 9. In addition, the median score of cutaneous sarcomas was 10. On the other hand, the benign lesions (melanocytic naevi, neurofibroma, epidermal cyst and other benign lesions, including fibrous papules of the nose, syringoma and solar elastosis) had median EIS scores of 5 and lower. Although secondary excisions, seborrhoeic keratosis, and inflammatory reactions are categorized as benign lesions, they had median EIS scores of 6, 7.5 and 6.5, respectively.
The correlation between tumour thickness and EIS score was evaluated for the malignant tumours for which tumour thickness data was available (n = 92). The mean ± SD tumour thickness was 2.4 ± 1.9 mm. There was no correlation between tumour thickness and EIS score (p = 0.392, r = 0.09).
The threshold values set for the ROC curves, which assign the sensitivity and specificity of the EIS, are shown with PPV and NPV in Table II.
Sensitivity, specificity, PPV and NPV were calculated for different EIS scores from 1 to 10. The smaller the EIS score the higher the sensitivity and the lower the specificity; both values were reversely correlated. The choice of a threshold should aim first for high sensitivity for recognizing the malignant tumour, with acceptable low specificity in order to avoid unnecessary excisions. According to Table II an EIS score of 5 is proposed as a threshold for the diagnosis of NMSC; values above 5 indicate a malignant tumour. For this cut-off value the sensitivity of EIS for NMSC was 94% and the specificity was 42%, with 78% PPV and 77% NPV.
Table II. Electrical impedance spectroscopy (EIS) diagnostic parameter values based on different cut-off scores
Using this method in the present cohort, only 3 tumours were missed, all of which were BCC. The diagnostic accuracy, combining sensitivity and specificity, can be seen on the ROC curve in Fig. 1. The area under the curve was 0.758.
Fig. 1. Sensitivity and specificity of electrical impedance spectroscopy technique represented on receiver operating characteristics (ROC) curve.
The early versions of EIS (Nevisense, SciBase AB, Stockholm, Sweden) were used by the cosmetic industry and researchers to investigate reactions of the epidermal barrier and oral mucosa (12, 13). With development of the measurement technique, the EIS device is progressing to become an adjunct diagnostic tool for use in melanoma detection in the field of dermatology (14).
The properties of the electrical current passing through the tissue provide information about the malignant potential of the lesion (15, 16). The EIS method reveals different cellular properties, such as the composition of both intracellular and extracellular environments, cell shape and size, and cell membrane composition, in the different frequency regions of measurement (3). These features are affected even if pleomorphism and atypia are minimal in the tumour cell. It has been shown that adding EIS measurements to the information from naked eye examinations or dermoscopic examinations conducted for detecting melanoma improves the diagnostic performance of dermatologists, decreases the number of biopsies of benign lesions, and reduces the need for sequential digital dermoscopy imaging (17–19). EIS could also assist general practitioners to decide which patients to refer to a dermatologist due to suspicion of skin cancer (19). A combination of more than one non-invasive method may be efficacious, especially when surgical excision cannot be performed. EIS has advantages over the new generation non-invasive imaging devices, such as spectrophotometric intracutaneous analysis and multispectral imaging, in terms of improved sensitivity and specificity for melanoma detection, and the ability to provide rapid results (6). Moreover, the score of EIS measurement is not dependent on the clinician performing the assessment, and training to use the device is easier than for other non-invasive diagnostic methods. In addition to dermoscopy, non-invasive diagnostics, such as reflectance confocal microscopy (RCM) and optical coherence tomography (OCT) are also being used in the diagnosis of NMSC. With development of the technology, the reported sensitivity and specificity values of RCM and OCT differ according to the modality of the device or tumour type (20, 21). Although the sensitivity and specificity of the EIS technique found in this study are not much higher than the other methods mentioned, it could be speculated that EIS is a promising tool due to short processing time, ease of transportability, decreased error rate resulting from the clinician’s interpretation, and more accessibility due to cost advantage.
To the best of our knowledge, no previous studies have evaluated the diagnostic accuracy of EIS for NMSC alone. The sensitivity and specificity of EIS for NMSC have only been reported by multicentre studies targeted mainly at diagnosing melanoma. These studies reported a sensitivity of 100% for both BCC and SCC, but the specificity varied between 17% and 43% (22, 23). The higher sensitivity value can be interpreted by the lower determined cut-off value, namely between 3 and 4, compared with the assumed threshold in the current study, which is above 5. Similar to the current study, the number of NMSC cases in these studies is limited. The results of the present study showed that EIS has a promising discriminative power for distinguishing between NMSC and benign skin tumours. This was particularly true for BCC and SCC, as well as sarcomas, which showed very high EIS values. Therefore, the indication for the use of this diagnostic tool should probably also be extended to NMSC. Interestingly, there was no statistical difference between the mean EIS scores for SCCs and BCCs. Both tumours presented with higher values than the benign lesions.
It can be assumed that the electrical impedance score was positively correlated with tumour thickness. Although the results of some studies on melanoma support this relationship (19, 23), the current study did not find a correlation between tumour thickness and the EIS score in this study. A possible reason for this finding is the significant difference between melanoma thicknesses in the above-mentioned studies and NMSC thicknesses in the current study. The penetration depth provided by the electrode, which is up to 2.5 mm, may be affected by the structure of the stratum corneum (7). A theoretical explanation is that the damaged upper layer of the stratum corneum may block the electrical current and not allow it to flow down to the deeper layers of the lesion. On the other hand, if the structure of the tumour at the superficial penetration depths of the electrical current has already changed, the EIS measurements can result in high scores regardless of tumour thickness or the invasion level of malignant cells.
In this study, the secondary excisions were performed for NMSC in order to maintain an adequate safety margin when 3D histologically-confirmed free resection margins were not previously achieved. Although all of the secondary excisions were reported as tumour-free, this re-excision implies that the area measured with the electrode contained scar tissue. Measuring ulcerated, fibrotic, or scar tissue with the EIS method is not recommended because of the possibility of false-positive results. Conversely, the lesion can be considered as benign despite the presence of scar tissue when the score is low. The mean EIS score of the secondary excisions was 6.55 (5.66–7.44). When the secondary excisions were excluded from the evaluation, a sensitivity of 94.2% and a specificity of 42.9% (AUC: 0.776) were achieved, which were quite similar to the previous results. Seborrhoeic keratosis, another subgroup of benign lesions, also presented rather high EIS scores. The mean EIS value for seborrhoeic keratosis was 7.43 (6.48–8.38) and, thus, most of these lesions were regarded as skin cancer. Previous studies have already shown that EIS can be inaccurate for diagnosing seborrhoeic keratosis, as it can provide false-positives, and for this reason it is not recommended for such evaluations (3, 23). However, some seborrhoeic keratoses are difficult to distinguish from NMSC; therefore they should not have been excluded from the benign lesions in this study, as it aimed to improve NMSC diagnostics.
Study limitations
This study has several limitations. Firstly, this is a single-centre study, which may be biased by the specific patient collective being treated at this centre. Secondly, thick SCC and BCC tumours may be overrepresented in the dermatosurgery division of the university hospital, whereas thinner lesions are frequently operated in private dermatology offices and outpatient clinics. Thirdly, this study analysed a rather limited number of cases, particularly for the benign lesions, which limits the statistical power of the study. Since the EIS score is affected by cellular features, it would be optimal to evaluate tumours derived from different tissues in separate studies and to make the comparison in malign and benign tumours of similar origin. In this study, there were only 3 connective tissue-derived benign lesions, which were fibrous papule of the nose (n = 1) and solar elastosis (n = 2). Although the mean EIS score of these 3 lesions was lower than the sarcoma group’s score, the sample size was not adequate to make a significant comparison.
Conclusion
EIS has good discriminative power to distinguish NMSC from benign cutaneous lesions. Although EIS cannot replace the gold standard, histopathology, it may guide and support the clinicians in early diagnosis of NMSC, as in melanoma. Due to the ease of use and no requirement for dermatology expertise training, the EIS device seems to be most appropriate for use in primary healthcare offices as a screening tool for triage of the lesions for referral to specialists for further evaluation. Additional prospective trials with larger numbers of tumours are required to test the sensitivity and specificity of this method and to confirm or reject the results of the current study.
The authors thank SciBase AB, Stockholm, Sweden, for providing the Nevisense electrodes for this study.
Conflicts of interest: ES, AM, LK and HMH have no conflicts of interest to declare. TKE reports personal fees from Amgen, personal fees from BMS, personal fees from MSD, personal fees from Roche, personal fees from Novartis, personal fees from Pierre Fabre, personal fees from Sanofi, personal fees from Leo Pharma, outside the submitted work. SF reports personal fees from Takeda Pharmaceutical. CG reports personal fees from Amgen, grants and personal fees from BMS, personal fees from MSD, personal fees from Philogen, grants and personal fees from Roche, grants and personal fees from Novartis, personal fees from Pierre Fabre, personal fees from Sanofi, outside the submitted work.


 Click to show fullsize
Click to show fullsize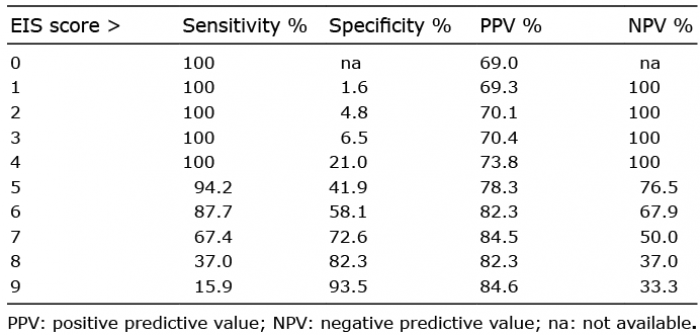 Click to show fullsize
Click to show fullsize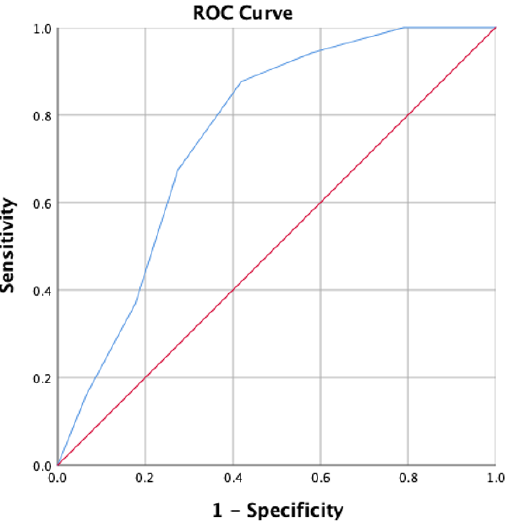 Click to show fullsize
Click to show fullsize