


1Department of Ophthalmology and 2Department of Dermatology and Venereology, Sahlgrenska University Hospital, Gothenburg, Sweden
Uncertainty exists regarding the results of treating basal cell carcinomas with a more aggressive growth pattern than nodular growth with cryosurgery. Over the years, some medium aggressive, well-defined basal cell carcinomas have been treated with cryosurgery at the combined ophthalmology-dermatology recipiency at Sahlgrenska University Hospital, Gothenburg in Sweden. The medical records of these patients were reviewed to analyse the results. A total of 53 cryosurgeries were performed in 52 patients during 2009 to 2016. None of these patients had a recurrence within the first 3 years. There were 2 recurrent tumours after 5 years and 1 after 9 years. It is concluded that cryosurgery is an effective treatment option for well-defined basal cell carcinomas with an intermediate growth pattern.
Key words: basal cell carcinoma; Glas type 2; cryosurgery; eyelids.
Accepted Nov 4, 2020; Epub ahead of print Nov 10, 2020
Acta Derm Venereol 2020; 100: adv00336.
doi: 10.2340/00015555-3691
Corr: Oscar Finskas, Department of Ophthalmology, Sahlgrenska University Hostpital, Göteborgsvägen 31, SE-431 30 Mölndal, Sweden. E-mail: oscar.finskas@vgregion.se
Basal cell carcinomas can be classified into 3 major types depending on aggressiveness: low, medium/mixed, and high. Cryotherapy is usually reserved for basal cell carcinomas with low aggressiveness. This study reviewed the outcome of 53 cryotherapies of medium aggressive basal cell carcinomas in the periocular region performed during the years 2009 to 2016. The results suggest that cryotherapy is an effective treatment option for well-defined medium aggressive periocular basal cell carcinomas.
Basal cell carcinoma (BCC) is the most common malignant skin tumour: one-third of the fair-skinned population will be affected during their lifetime (1). During the last 30 years the incidence of BCC is estimated to have increased by 20–80% in the USA (2) and is also on the rise in the Scandinavian countries (3). Periocular BCC accounts for 10% of all cases of BCC (4). The treatment for BCC is controversial. The commonly used methods are Mohs micrographic surgery (MMS), surgical excision and reconstruction, curettage and electrocautery or electrodessication (C&E), photodynamic therapy and cryosurgery (5–7). Cryosurgery is a method proven to have a low recurrence rate and also has a good cosmetic outcome (8–12). It has been in use since the 1960s (7). Cryosurgery is most commonly used to treat well-defined BCCs with low aggressiveness, and MMS is most commonly used for ill-defined, aggressive BCCs (13). Usual clinical practice in Sweden is to use cryosurgery for low aggressive BCCs not located in the face region, and surgery or MMS, depending on the aggressiveness of the BCC, when located on the face. Previous studies from our group have shown good results with cryosurgery but have not differentiated subgroups of BCCs. This paper analyses our results for treating a more aggressive group of BCCs.
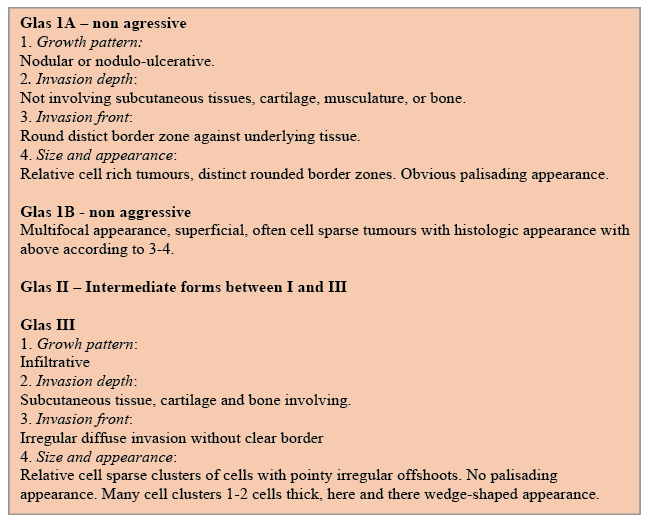
The medical records of all patients who had visited the combined ophthalmology – dermatology recipiency during the years 2009 to 2016 were reviewed. In Sweden BCCs are divided histopathologically by the classifications proposed by Jernbeck et al. (“Sabbatsbergsmodellen”) (14). Nodular BCCs (Glas 1A), superficial BCCs (Glas 1B), infiltrative, moderately aggressive BCCs (Glas II) and highly aggressive, morpheiform BCCs (Glas III). Glas II BCC accounts for approximately 10–20% of all BCCs (14, 15) (Fig. 1).
Fig. 1. Histological definition according to Sabbatsberg’s model (14).
The patients referred to us had biopsy-proven BCCs judged to be suitable for treatment with cryosurgery, low and medium aggressive BCCs, and a well-defined clinical border. The medical records were reviewed until 31 December 2019. Variables recorded were: age, sex, size of lesion, location (upper eyelid, lower eyelid, medial and lateral side of the eye), if curettage had been used, any tumour recurrence and time interval (in months) between treatment and recurrence. The patients were actively monitored for one year and later instructed to contact the dermatology or ophthalmology department in case of a suspected tumour recurrence. Only patients with a primary BCC were treated with cryosurgery. The protocol for cryosurgery was 2 complete cycles of more than 60 s thaw time, described by Lindgren et al. (16). A completed thaw cycle involved a fully frozen tumour and a margin of 3 mm. The patients were treated during an outpatient visit. Location, side and largest diameter of the tumour were recorded. Local anaesthetic (lidocaine, 10 or 20 mg/mL with adrenalin 5 µg/mL) was injected in the tumour area. Anaesthetic (oxybuprocaine or tetracaine) eye drops were applied on the surface of the eye. Any tumour with a height of more than 3 mm was reduced with a curette. Neoprene cones (Cortex Technology, Hadsund, Denmark) with 3-mm thick walls with various diameters were used during the freezing process. Liquid nitrogen was sprayed onto the with the neoprene cone surrounding the tumour. Jaeger plates were used to shield the bulb when the eyelid margin was involved. Freezing was continued until whitening of the exterior margin of the cone was observed, usually after 25–30 s. The freezing time was defined as the time required to freeze the selected area (tumor and margin). The tissue was allowed to defrost completely, then a second freeze-thaw cycle was performed. If any of the 2 freeze treatments were under 1 min, a third freeze-thaw cycle was performed. Patients had a follow-up at 1 week, 1 month and 1 year (Fig. 2). They were told to contact the treatment centre if they had a suspected recurrence thereafter.
Fig. 2. Patient with Glas type 2 basal cell carcinoma. (A) Before cryosurgery. (B) Three years after treatment.
A total of 53 cryosurgeries from 52 individuals were included, of these 39 (74%) were performed on women. Twenty-nine (55%) tumours were located on the right side. Forty-five (85%) tumours were classified as Glas II, 8 (15%) were considered to be a mixed type at least partly classified as medium aggressive. The inferior eyelid was most commonly affected in 33 (62%) instances, followed by the medial 15 (28%), upper 4 (8%) and the lateral 1 (2%). The mean age by the time of diagnosis was 73 years (range 49–97). The mean size of the tumour was 9.6 mm (SD ± 3.4), the largest successfully treated tumour had a diameter of 20 mm. Curettage had been used in only one instance. During the first 3 years no recurrence was found. Among reviewed cryosurgeries only 3 had recurred: 2 cases 5 years after cryosurgery and 1 after 9 years. Three patients died from unrelated causes. They all had a follow-up for at least 2 years. In this study no recurrence of Glas II BCC was observed during a 3-year follow-up. None of the 3 patients assessed as having a relapse used immunosuppressive medication. One of the patients had the first tumour located medially with the recurrence far laterally on the lower eyelid. We chose to interpret all new BCCs on the same side as recurrences (Table I).
Table I. Characteristics of the 53 cryosurgeries included in this study
The recurrence rate (6%) was comparable to that found in previous studies. Mallon et al. (17) showed a 95.3% cure rate in the face area using a similar protocol as described here (2 freeze-thaw cycles). A systematic review of recurrence rates found a cumulative risk of 4–17% with a 5-year follow-up (18). A study performed previously at our centre showed a recurrence rate of less than 0.5% (16). In that paper, BCCs with low aggressiveness were not separated from medium aggressive BCCs. The recurrence rate after Mohs microsurgery treatment is estimated as 3% with a 5-year follow-up (19). The current study could not identify any adverse events or self-reported dissatisfaction with the cosmetic results after cryosurgery. Thissen et al. (18) showed that 87.5% of cryosurgery treated patients achieved a “good” cosmetic result, 12.5% “fair”, and no patients reported a “bad” result. The current study suggests that cryosurgery for large clinically well-defined Glas II BCCs is an effective treatment with low tumour recurrence. There are many advantages of cryosurgery. It is performed in an outpatient setting with no need for an operating theatre. Cryosurgery does not require the aseptic environment needed for Mohs surgery. The adnexal tissue is preserved, which is especially valuable with large tumours and those involving the tear drainage system. Anticoagulation therapy does not need to be discontinued before surgery. Cryosurgery may be less expensive than surgery, which is an important factor with increasing cancer incidence worldwide, although studies are needed to confirm this. Cryosurgery is a valuable treatment option in addressing the increasing global incidence of BCC.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize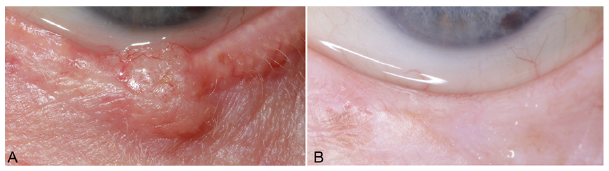 Click to show fullsize
Click to show fullsize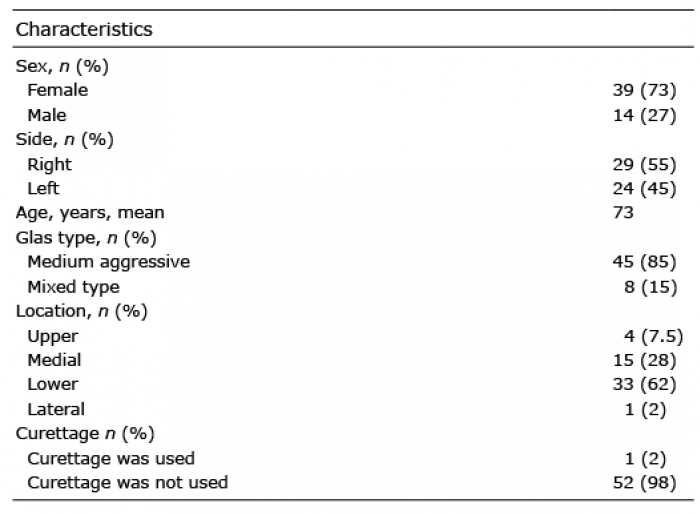 Click to show fullsize
Click to show fullsize