


1Department of Dermatology, Peking University People’s Hospital, No. 11 Xizhimen South Street, Xicheng District, Beijing, China and 2Department of Dermatology and Dermatologic Surgery, Medical University of South Carolina, Charleston, SC, USA. *E-mail: chengzhou@live.cn
Accepted Nov 11, 2020; Epub ahead of print Nov 16, 2020
Acta Derm Venereol 2021; 101: adv00352.
doi: 10.2340/00015555-3693
Ectodermal dysplasia is a group of rare genetic disorders that affect structures of ectodermal origin, which includes nearly 170 syndromes (1). Hypohidrotic ectodermal dysplasia (HED), the most common variation, is characterized by hypohidrosis or anhidrosis, hypotrichosis, hypodontia or anodontia, and distinct facial features, including prominent forehead and lips, epicanthic fold, everted nose, and prognathism.
HED has autosomal dominant, autosomal recessive, and X-linked forms (2). The most frequent subtype is X-linked HED (XL-HED; MIM #305100), with a prevalence of 1.6–22 per 100,000 persons, which is caused by mutations in the ectodysplasin A gene (EDA; NM_001399.4) located at Xq12–q13.1 (3). Currently, according to the NCBI ClinVar database, at least 131 novel pathogenic mutations have been identified in patients with HED, among which more than 80% were EDA mutations (4). The EDA gene encodes the transmembrane protein EDA, a member of the tumour necrosis factor α-related signalling pathway (1, 5). The protein is critical for signal transduction from ectoderm to mesenchyme, leading to the development of hair follicles, teeth, skin, nails, and eccrine glands during morphogenesis.
Additional findings associated with XL-HED may include recurrent upper respiratory infections, asthma, nasal crusting, keratoconjunctivitis sicca, dry skin and eczema (6). We report here a novel mutation of the EDA gene in a Chinese patient with HED and severe atopic dermatitis that responded well to the treatment of an oral Janus kinase (JAK) inhibitor, tofacitinib.
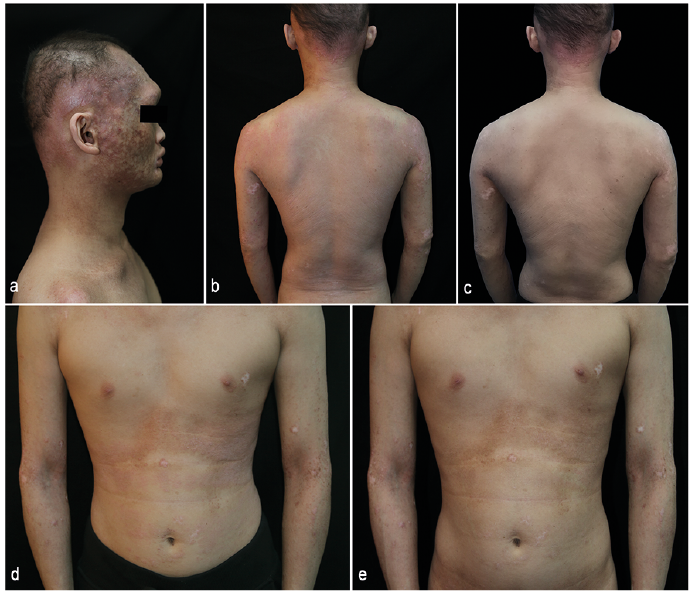
A 22-year-old man presented with severe itching for more than 20 years and early-onset asthma. He was the second child of non-consanguineous parents and all his relatives were unaffected. Examination revealed xerosis and extensive lichenification on the face, trunk and extremities (Fig. 1b, d). Multiple, discrete, flesh-coloured follicular keratotic papules were noted on the forehead and cheeks, and confluent pinkish plaques were noted on the occipital scalp, compatible with keratosis follicularis spinulosa decalvans (KFSD) (Fig. 1a, b). His scalp hair, eyebrows and eyelashes were sparse, and body hair (including pubic hair) was absent. His facial appearance included a saddle nose, everted lips, frontal bossing and small chin (Fig. 1a). Teeth were absent and faciocervical poikiloderma was noted. Nails and mucosa were normal. White blood cell count was 9.21/μl with 12.7% eosinophils, and the total serum IgE was >2,000 IU/ml. Serum allergen-specific IgE antibody scoring was class 6 for Artemisia and cedar pollen, class 5 for ragweed and cat hair, class 4 for dog hair and altenuene (Alternaria), class 3 for cypress pollen, class 2 for house dust mites, and class 1 for ascarid.
Fig. 1. Clinical features. (a) Characteristic facial appearance, presenting as frontal bossing, small chin, everted lips, sebaceous hyperplasia, atrophy and alopecia of the temporal scalp. (b–e) Eczematous lesions with lichenification on the trunk: before and after 2 weeks of oral tofacitinib, showing significantly improvement. (b, c) Back, (d, e) chest and abdomen.
After obtaining written informed consent, peripheral blood was collected from the proband and his mother, and genomic DNA was isolated. Genomic DNA was also extracted from 100 unrelated healthy Chinese individuals as controls. A hemizygous deletion mutation in the EDA gene (c.28delG; p.E10Nfs*47) was identified in the proband by next generation sequencing and verified by Sanger sequencing. His mother was found to be a carrier with a heterozygous mutation (Fig. 2). The mutation was not found in normal controls or in the Human Gene Mutation Database (http://www.hgmd.org). No mutation was found in atopic dermatitis-associated genes, including FLG, SPINK5, KLK5 and CLDN1 genes.
Fig. 2. Molecular analysis of the ectodysplasin A (EDA) gene. (a) Sequencing analysis identified a hemizygosity deletion mutation, c.28delG; p.E10Nfs*47, in exon 1 in the patient. (b) Results of the DNA sequencing analysis of his mother. Deletion site indicated by arrows.
The patient did not respond to treatment with oral antihistamines, topical corticosteroids or traditional Chinese medicines and declined treatment with methotrexate and ciclosporin. Dupilumab was not available in China at the time, and he was prescribed oral tofacitinib tablets 5 mg twice daily based on availability and the success of other JAK inhibitors in atopic dermatitis. The skin lesions and pruritus were significantly improved after 2 weeks of treatment with tofacitinib (Fig. 1c, e). The percentage of blood eosinophils fell to 3.3% (absolute count 0.30/μl). Sweating showed no significant change, but his asthma did not recur during the drug therapy. Continuous improvement in skin symptoms and the appearance of vellus hair on the forehead were noted over the next 6 months with no adverse events.
We describe here a novel EDA mutation leading to XL-HED with severe atopic dermatitis. To date, approximately 340 variants have been reported in EDA genes (Human Gene Mutation Database). Among these, 187 (54.8%) were missense/nonsense mutations, 87 (25.5%) were deletions, 32 (9.4%) were splicing, 28 (8.2%) were insertions and 7 (2.1%) were indels. The phenotype relates to the type and location of mutations. EDA mutations with protein truncating (including frameshift and nonsense) correlate with a more severe phenotype, and missense mutations associated with a milder phenotype (2). Burger et al. (7) reported that EDA genotype correlates with the severity of atopic dermatitis-like skin lesions in XL-HED patients. The deletion mutation of c.28delG (p.E10Nfs*47) in the current patient resulted in loss-of-function of the signalling protein EDA, affecting the ectodysplasin/nuclear factor-κB (NF-κB) signalling pathway (5, 8), and resulted in severe atopic dermatitis. Patients with HED often have dry skin (94%) and eczematous skin (47–84%) in various degrees (7, 9, 10) as well as bronchial asthma (>30%), allergic rhinitis (>70%) and physician-diagnosed food allergies (20.7%) (11). The current patient presented with severe atopic dermatitis and KFSD-like skin lesions, which has not been reported previously in XL-HED-affected patients.
Tofacitinib is a JAK1-3 inhibitor (12, 13), which is available in China. Based on prior reports of response to JAK inhibitors (13, 14), tofacitinib was prescribed in the current patient and resulted in rapid and sustained improvement in pruritus and skin lesions.
We speculate that the novel loss-of-function mutation in EDA resulted in defective activation of NF-κB pathway and upregulation of inflammatory cytokines that activate JAK signalling. This patient’s response suggests that JAK inhibitors deserve further study in patients with atopic dermatitis associated with ectodermal dysplasia.
The patient provided written informed consent to publication of his case details.
This study was supported by the National Natural Science Foundation of China (No. 81773311).
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize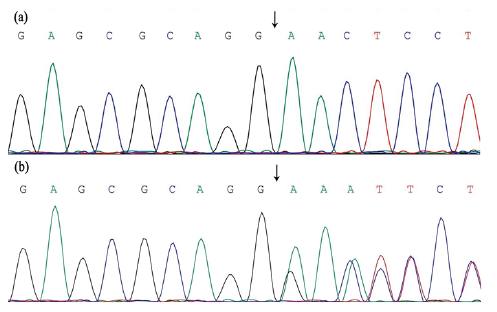 Click to show fullsize
Click to show fullsize