


1University Brest, LIEN, 2Department of Dermatology, University Hospital of Brest, Brest, and 3EMMA, Fontenay-sous-Bois, France
The aim of this study was to examine the prevalence and nature of fatigue in patients with skin diseases by comparison with controls, using a survey of a large representative sample of the French population (n = 2,502). Of the respondents, 659 reported having a skin disease and 1,843 did not. Quality of life was decreased in people with skin diseases compared with controls, while levels of stress and sleep deprivation were higher in people with skin diseases. Level of fatigue was higher in people with skin diseases than in controls. The relative risk of fatigue was 4.71 (3.44–5.98, p < 0.001). Mediation analysis, adjusted according to sex, age and each skin disease, showed that the effects of skin diseases on fatigue were more commonly direct than indirect. To our knowledge, this is the first study to demonstrate that patients with skin diseases experience fatigue more frequently and more intensely. Hence, fatigue should be used as a new patient-related outcome in clinical trials.
Key words: fatigue; skin; dermatosis; inflammation; quality of life; sleep.
Accepted Nov 11, 2020; Epub ahead of print Nov 16, 2020
Acta Derm Venereol 2020; 100: adv00327.
doi: 10.2340/00015555-3694
Corr: Laurent Misery, Department of Dermatology, University Hospital of Brest, 2 Avenue Foch, FR-29200 Brest, France. E-mail: laurent.misery@chu-brest.fr
To date, there has been little research regarding fatigue in patients with skin diseases. This study, based on a survey of the French population, found that fatigue is almost 5 times more frequent in patients with skin diseases. Statistical analysis suggests that both direct and indirect effects could explain the fatigue. Fatigue should be taken into account when treating patients with skin diseases.
Fatigue can be defined as “an overwhelming, debilitating, and sustained sense of exhaustion that decreases one’s ability to carry out daily activities, including the ability to work effectively and to function at one’s usual level in family or social roles” (1). Fatigue is a common symptom in primary care, with many causes, ranging from benign to life-threatening (2). Fatigue is influenced by an individual’s age, sex, physical condition, mental status, psychological condition, personality type, health status, diet, the the latency from an individual’s previous meal, and life experiences (3). In addition, fatigue can be classified as a condition occurring at rest or under exercise or stress, as a physiological reaction or a pathological condition, as a spontaneous phenomenon or a triggerable state, as a resistant or a non-resistant response to preconditioning, training, or attitudes, as a prominent or collateral experience, and as an accessible or an inaccessible response to any type of treatment or intervention (3). Fatigue may be the sole symptom of a disease or one symptom among others. It may also be classified as acute or chronic (3). Fatigue is common in the general population, with a prevalence of approximately 20% (4).
Fatigue is rarely considered a symptom of skin diseases or even a comorbidity, but patients frequently report fatigue. In a previous study, we found that acne was associated with fatigue on waking (5). More women than men reported fatigue on waking. Among the individuals who were tired on waking, compared with those who were not tired on waking, the proportion of people who felt stressed every day was higher, but there was not a considerably higher proportion of people with sleep disorders. After adjusting for sex and age, the presence of acne remained highly associated with fatigue on waking.
In order to determine whether fatigue is also associated with skin diseases other than acne, a survey of a representative sample of the French population was performed. The prevalence of fatigue in patients with skin diseases was compared with controls.
A polling institute (HC Conseil Paris, France) performed the survey between 5 April 2019 and 2 May 2019, using a representative sample of the adult population (n = 2,502) aged over 15 years. Proportional quota sampling was applied to render the study population representative of the French general population aged > 15 years, based on the National Institute for Statistics and Economic Studies Institute (INSEE) data. The e-mail addresses of 900,000 internet users who agreed to participate in the surveys (megabase-Quantar) were collected, and fixed quotas of subjects fulfilling the predefined sociodemographic criteria were applied. Double stratification according to age and sex, as well as geographical area of residence, was conducted. If the contact was unsuccessful, another potential participant with the same characteristics was randomly selected. Each participant completed an online questionnaire containing approximately 30 items, which took approximately 12 min.
The first set of questions concerned sociodemographic characteristics and general health status and aimed to avoid biased answers. These questions were followed by more specific questions on dermatology, such as existing skin diseases diagnosed by a clinician, and more specific questions on fatigue and sleep. Stress and fatigue levels were measured by a visual analogue scale (0–100).
The validated French version of the MFI-20 questionnaire (Multidimensional Fatigue Inventory) was also administered to the interviewed subjects (6). The MFI is a 20-item self-report instrument designed to measure fatigue. It consists of 20 questions divided into 4 dimensions: general/physical fatigue; mental fatigue; reduction in activities; and lack of motivation (7). Patients answered the questions by selecting a number between 1 (“yes, it is true”) and 5 (“no, it is not true”) that best reflected their feelings in the days before the questionnaire was administered. High values indicate a high level of fatigue. This questionnaire is relevant for measuring patients’ fatigue level because it measures the 3 components of fatigue (physical, psychological, and cognitive), provides a total fatigue score, and has valuable psychometric properties (7).
The quality of life of the participants was measured with the Short Form-12 Health Survey (SF-12) (8). Two scores can be calculated: a Physical Component Summary (PCS-12) and a Mental Component Summary (MCS-12). There is no overall score. The higher the score, the better the subject’s quality of life (9).
First, the association between presence of a skin disease diagnosed by a clinician and tiredness level was measured with a t-test, and the association between sleep deprivation and stress level was measured with a Wilcoxon test. The links between tiredness and stress level assessed with the VAS, and between tiredness and sleep deprivation, were assessed using Pearson’s correlation coefficient. Univariate and multivariate linear analyses were used to assess the associations between tiredness, lack of sleep, and stress level and each skin disease (acne, rosacea, psoriasis, atopic dermatitis and contact dermatitis). The multivariate analysis was adjusted for age, sex, Clinical Stage Prediction (CSP) and each of the other skin diseases. Because lack of sleep, stress and tiredness were thought to have a mediating, rather than a confounding, effect on each other, the analysis was not adjusted for these factors.
Mediation analyses quantify whether the strength of the relationship between 2 variables is affected by the presence of a third variable, known as the mediating variable. Direct and indirect effects can therefore be differentiated; the indirect effect corresponds to the effect, which is due to the increase in mediating factor (e.g. patients are more tired when they have a skin disease, because they are more stressed or have poorer sleep) and the direct effect, which is not due to these factors (e.g. patients are more tired when they have a skin disease, independently of being more stressed or having poorer sleep). These direct and indirect effects add up to give the total effect. In the current analysis sleep deprivation and stress were used as mediating factors and the analysis was adjusted for age, sex, socio-professional category and each of the other skin pathologies. The mediation analyses were adjusted for age, sex, CSP and each of the other skin diseases. The imputation method from the medflex package in R Foundation, Vienna, Autsria was used. All statistical analyses were performed using R version 3.5.1.
Among the 2,502 participants in the study, 1,286 were female (51.4%) and 1,216 were male (48.6%). Of the participants, 659 reported having a skin disease (mean ± standard deviation (SD) age 43.8 ± 16.3 years; females 50.1%, males 49.9%), while 1,843 did not report having a skin disease (mean ± SD age 46.3 ± 15.2 years; females 51.9%, males 48.1%) (p < 0.001). Among the 659 patients, 522 had 1 dermatosis, 101 had 2 and 36 had 3 dermatoses. There were 132 patients with acne, 123 with contact eczema, 117 with atopic dermatitis, 116 with psoriasis and 78 with rosacea. Other diseases were reported by fewer than 75 patients.
Comparisons between subjects with skin diseases (patients) and those without skin diseases (controls) showed that quality of life, as assessed by mental composite score (39.6 vs 432 , respectively, p < 0.001) and physical composite score (49.1 vs 51.7, respectively, p < 0.001) scores, was lower, while stress level (4.6 vs 3.1, respectively, p < 0.001) and sleep deprivation level were higher (4.3 vs 3, respectively, p < 0.001) in patients with skin diseases than in controls.
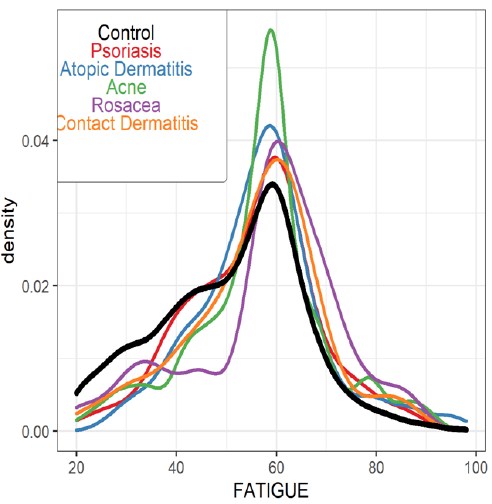
Fatigue level was higher in patients than in controls (55.8 vs 51.1, respectively, p < 0.001). Fatigue level was well correlated with sleep deprivation (Pearson’s correlation coefficient 0.35, p < 0.001) and stress (Pearson’s correlation coefficient 0.42, p < 0.001) levels, which were also well correlated with each other (Pearson’s correlation coefficient 0.43, p < 0.001). Analysis of the 5 most frequent skin diseases (psoriasis, atopic dermatitis, acne, rosacea, and contact dermatitis) showed that fatigue was higher in patients with any of these diseases than in controls (Fig. 1).
Fig. 1. Fatigue in patients with the 5 most frequent skin diseases.
Univariate analysis showed a relative risk of fatigue of 4.71 (3.44–5.98, p < 0.001), while multivariate analysis showed a relative risk of fatigue of 4.23 (2.98–5.47, p < 0.001). The results for the 5 most frequent dermatoses are shown in Table I. Multivariate analysis showed that sleep deprivation was higher in patients (p < 0.001), especially those with rosacea (relative risk (RR) 1.38; 0.61–2.16, p < 0.001), psoriasis (RR 1.17; 0.53–1.82, p < 0.001) or acne (RR 1.13; 0.51–1.75, p < 0.001).
Table I. Relative risk of fatigue in patients with the 5 most frequent (> 75 patients) dermatoses according to univariate and multivariate analyses
Multivariate analysis showed that stress levels were higher in patients (p < 0.001) than in controls, especially those with rosacea (RR 1.33; 0.59–2.07, p < 0.001) or psoriasis (RR 1.68; 1.07–2.29, p < 0.001).
Mediation analysis showed that the effects of skin diseases on fatigue were both direct and indirect. In all skin diseases, the direct effect was higher than the indirect effect (direct RR 2.61, 1.42–3.79, p < 0.001; indirect RR 1.61, 1.17–2.05, p < 0.001). When examined individually, the skin diseases were quite different; acne (direct RR <0.001, 1.43–3.79, p = 0.84; indirect RR 1.97, 1.17–2.05, p < 0.001) and psoriasis (direct RR 0.24, 1.43–3.79, p = 0.83, indirect RR 3.22, 1.17–2.05, p < 0.001) presented almost only indirect effects, whereas rosacea (direct RR 2.78, 1.43–3.79, p = 0.067; indirect RR 2.87, 1.17–2.05, p < 0.001), contact dermatitis (direct RR 1.68, 1.43–3.79, p = 0.15; indirect RR 1.03, 1.17–2.06, p = 0.068) and atopic dermatitis (direct RR 1.26, 1.43–3.79, p = 0.28; indirect RR 2.39, 1.17–2.06, p < 0.001) presented both direct and indirect effects, and there was a nearly significant direct effect for rosacea (Fig. 2).
Fig. 2. Mediation analysis.
Sensitive skin was also associated with higher fatigue, stress and sleep deprivation levels, and these data were more demonstrative when examined by the severity of skin sensitivity according to the subject’s opinions (none, low, medium, or high) (see Table II for results regarding fatigue).
Table II. Relative risk of fatigue according to the severity of sensitive skin
To our knowledge, this is the first study to show that patients with skin diseases report fatigue more frequently and more intensely than controls through direct and indirect (stress, alterations in quality of life and sleep) effects. Hence, fatigue should be considered as a symptom or a comorbidity of many skin diseases and can be used as a new patient-related outcome in clinical trials.
In a literature review, we found only one paper on fatigue in individuals with acne (5), one on fatigue in individuals with atopic dermatitis (10), and a few on fatigue in individuals with psoriasis (11–13). Notably, all of these studies were conducted recently. Research on fatigue in individuals with psoriatic arthritis is slightly more developed and more dated (14, 15). Recently, an international patient and physician consensus on a psoriatic arthritis core outcome set for clinical trials identified fatigue as one of the most important outcomes (16). In the field of dermatology, fatigue appears to be more underestimated than pruritus (17) or psychological disorders (18), which are heavily underestimated.
The sample size of the current study allows accurate statistical analysis and specific analysis of patients with the 5 most frequently studied dermatoses. Surveys are currently being used more frequently in dermatology (19, 20).
Although the answers to the questionnaires were not confirmed by doctors, they are valuable for subjective assessment of conditions such as fatigue or sensitive skin. The results are more debatable than those of objective diagnoses for conditions such as skin diseases, but the respondents were asked to report provide only dermatological diagnoses provided by doctors, in order to limit such a bias. Another putative limitation of the study is that fatigue is a product of a patient’s representation of their condition and is part of the perception that they form about their illness (21); however, the use of scales and questionnaires in a large population allows pertinent results to be revealed for a population. Finally, the association of fatigue with other co-factors, such as professional activities or comorbidities, should be analysed in further specific studies on each skin disease. There was no selection bias in the current study, because the respondents did not know the purpose of the study before they began to answer the questionnaire.
Why skin diseases induce fatigue or are associated with fatigue is not known; the answer is probably multifactorial. This study suggests that both direct and indirect effects occur. Indirect effects could be higher stress levels, more sleep deprivation, alterations in quality of life, psychiatric morbidity, other comorbidities, or the use of some treatments. Direct effects could be related to systemic inflammation. The effects of itch on fatigue can be understood through both direct and indirect effects.
This study shows that the direct effects of skin diseases are higher than the indirect effects. Hence, a direct relationship between skin or systemic inflammation and fatigue is probable. The role of inflammation is probably crucial in diseases such as psoriasis and atopic dermatitis. Associations between fatigue and inflammatory markers have been documented in individuals with various medical conditions (21). Compelling evidence for a causal link between inflammation and fatigue comes from studies conducted in individuals receiving recombinant cytokines, such as interferon-alpha for the treatment of hepatitis C virus infection, malignant melanoma, or kidney cancer (21). In patients with skin diseases, inflammatory mediators can influence neurones directly or indirectly (21). Awareness of fatigue is triggered by interoceptive stimuli arising from the activation of afferent nerve endings that monitor the condition of tissues in the body (21–23).
The results of this study show that fatigue is correlated with higher stress and sleep deprivation levels. Stress is frequently associated with skin diseases (24). Similar to fatigue, sleep disorders in dermatological diseases are poorly studied (25). Sleep and skin disorders can interact at several levels (25).
Pruritus (itch) is a frequent symptom in dermatology (26, 27). Itch may be associated with fatigue through cytokines and neurotransmitters, which can induce both itch and fatigue. Itch is frequently responsible for sleep disorders and is associated with psychiatric comorbidities (28–30).
A recent study on the prevalence of fatigue in patients with psoriatic arthritis showed that the level of fatigue was moderate or intense in < 25% of patients (31). Fatigue seemed to be more related to the emotional and social aspects of the disease than to inflammatory aspects of the joints, confirming that the disease’s visibility is the most disturbing aspect for the patient and that “skin pain” is more intense than joint pain.
There is an increasing number of studies demonstrating that psychiatric comorbidities are usually associated with skin diseases. The most convincing study, an international multicentre observational cross-sectional study in 13 European countries, showed a high prevalence of depression and anxiety in patients with skin diseases, and the prevalence of depression and anxiety was highest for patients with psoriasis, atopic dermatitis, hand eczema, and leg ulcers (32). For several reasons, sleep disorders and fatigue are common symptoms of depression and anxiety.
However, psychiatric comorbidity is not the only factor that can explain fatigue in patients with skin diseases. For example, an association between psoriasis and chronic fatigue syndrome has also been evidenced (33). Psoriasis and rosacea are commonly associated with cardiovascular diseases, while fatigue is frequently associated with arterial hypertension and coronary heart disease (34). Fatigue is highly prevalent in individuals with diabetes or hyperlipaemia, which are commonly associated with psoriasis, but fatigue is not directly explained by hyperglycaemia or glucose variability (35). Fatigue is also highly prevalent in individuals with asthma (36), which is commonly associated with atopic dermatitis.
In many patients, fatigue may be an adverse event of treatments. Indeed, corticosteroids, cyclosporine, methotrexate, azathioprine, retinoids, apremilast and many others are well known for inducing fatigue. Patients also frequently report fatigue after injections of biological treatments. From the long-term perspective, a meta-analysis of randomized controlled trials in which anti-interleukin-12/23, -23, -17, or anti-tumour necrosis factor-α agents were used for the treatment of psoriasis vulgaris was conducted with fatigue as an outcome measure. These drugs were shown to have a consistently small-to-moderate beneficial effect on fatigue, independent of the type of drug (37).
This study shows that sensitive skin can be associated with fatigue and that fatigue is more frequently reported according to the severity declared by subjects. Since sensitive skin is a benign and very frequent disorder (38), we consider that fatigue is a facilitating factor of sensitive skin, rather than a result of sensitive skin.
In conclusion, fatigue is frequently reported by patients with skin diseases, and clinicians should take this symptom into account. In clinical trials, fatigue should more commonly be measured as a patient-related outcome.
Funding sources: EMMA (http://emma.clinic).
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize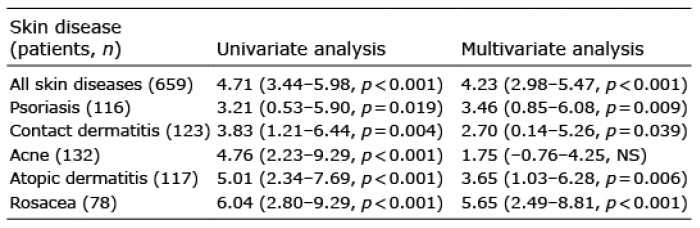 Click to show fullsize
Click to show fullsize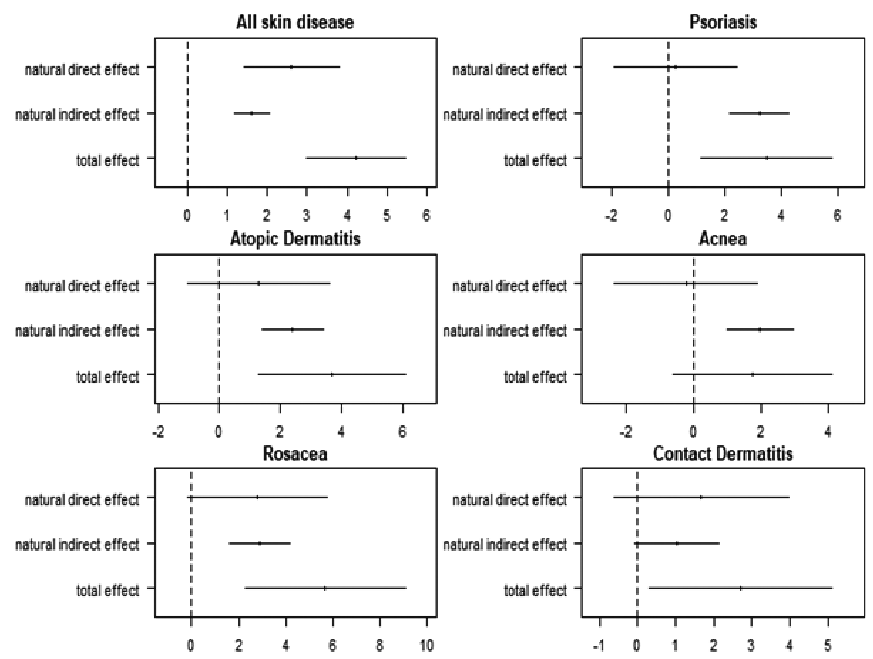 Click to show fullsize
Click to show fullsize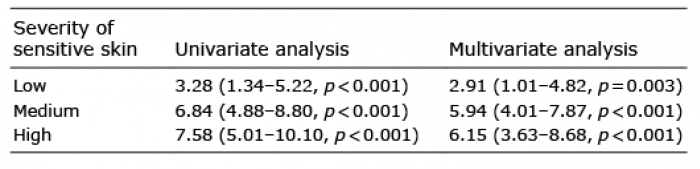 Click to show fullsize
Click to show fullsize