


Department of Dermatology and Venereology, Peking University First Hospital; Beijing Key Laboratory of Molecular Diagnosis on Dermatoses; National Clinical Research Center for Skin and Immune Diseases, No. 8 Xishiku Street, Xicheng District, Beijing, China. *E-mail: yangwang_dr@bjmu.edu.cn
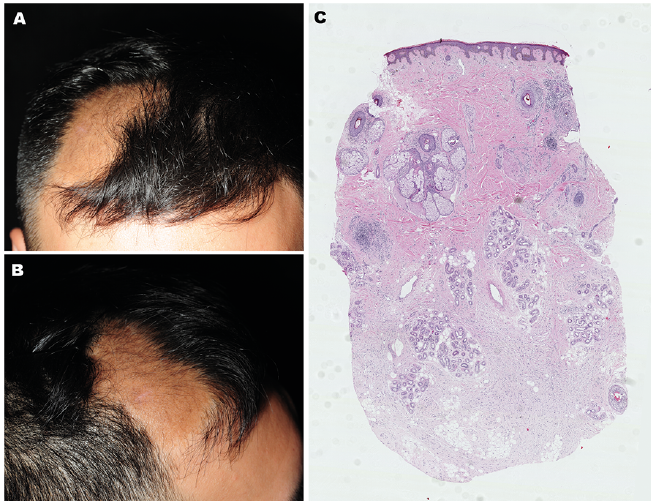
A 32-year-old man presented with a 10-year history of an asymptomatic alopecic plaque on his scalp. This lesion had slowly enlarged in size since it was first noted. The patient was otherwise healthy. His family history was unremarkable, and no family members had similar skin conditions. Physical examination revealed a circumscribed, 12×6 cm, slightly hyperpigmented plaque on the right frontal region of the scalp. The plaque was soft on palpation, with loss of hair on the overlying hyperpigmented skin (Fig. 1A, B). Physical examination was otherwise unremarkable, with no café-au-lait macules or skinfold freckling. A skin biopsy was obtained from the alopecic plaque for histopathological examination (Fig. 1C).
What is your diagnosis? See next page for answer.
Fig. 1. (A, B) Alopecic plaque on the scalp. (C) Skin biopsy from lesional scalp (haematoxylin-eosin, original magnification ×20).
Acta Derm Venereol 2021; 101: adv00361.
Diagnosis: Diffuse neurofibroma
Histopathology of the biopsy revealed an infiltrative lesion extending from the deep dermis into the subcutaneous fat. Terminal hair follicles were scarce and dislodged by the infiltration. Other skin appendages, including eccrine glands, were preserved (Fig. 1C). The infiltrates were composed of loosely arranged spindle cells with elongated wavy nuclei, surrounded by a matrix of collagenous fibres. Mast cells were numerous and easily found in the lesion (Fig. 2). A diagnosis of diffuse neurofibroma was confirmed by the histopathology. Further systemic evaluations did not reveal intracranial involvement or signs suggestive of neurofibromatosis. A complete resection of the lesion was performed. No recurrence was observed during follow-ups.
Neurofibroma is a common benign tumour that originates from the peripheral nerve sheath. In most cases, it presents as a solitary polypoid or nodular soft tumour. It may occur as multiple or widespread lesions accompanied by systemic features, referred to as neurofibromatosis. Histopathologically, several variants of neurofibroma were recognized: classical, myxoid, cellular, hyalinized, plexiform, epithelioid, diffuse, Pacinian, pigmented, and granular cell neurofibromas (1). Diffuse neurofibroma is a rare subtype, generally presenting as localized dermal and subcutaneous thickening with a predilection for the head or neck regions of children and young adults (2). Histologically, diffuse neurofibroma commonly reveals poorly defined, expansile proliferation of spindle cells infiltrating the dermis and subcutaneous tissue (3). Despite its infiltrative growth, it does not destroy, but rather envelops or dislodges, the skin appendages that it encompasses. As a result, it may lead to neoplasm-related alopecia when occurring on the scalp by “pushing away” the pilosebaceous units. Approximately 10% of diffuse neurofibromas are associated with neurofibromatosis type 1, but this subtype rarely undergoes malignant change (3).
Diagnosis of diffuse neurofibroma requires a combination of clinical and histopathological findings. Immunostaining with S100, CD56, or CD57 may be useful (4). Ultrasound, computed tomography, and magnetic resonance imaging may help determine the extent of the skin lesion and its anatomical relationship with adjacent structures (5). As for treatment, surgical excision is considered the first-line option for isolated neurofibromas, especially for large or symptomatic lesions (2). However, clinical recurrences may occur due to the extensive and infiltrative nature of many of these lesions. The difficulty of the operation depends partly on the dimensions of the tumour. Timely diagnosis is therefore important in order to improve the outcome of patients with diffuse neurofibroma.
In conclusion, this case highlights the importance of recognizing diffuse neurofibroma as a differential diagnosis of localized alopecia, which is important for appropriate treatment and achieving a better outcome.
Fig. 2. The tumour was composed of spindle cells with elongated ovoid to wavy nuclei, surrounded by a matrix of collagenous fibres (haematoxylin-eosin, original magnification ×200).


 Click to show fullsize
Click to show fullsize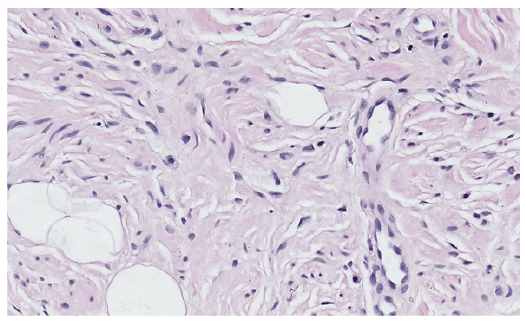 Click to show fullsize
Click to show fullsize