


Departments of 1Internal Medicine, 2Hematopathology, 3Pathology, and 4Medical Oncology, University of Colorado School of Medicine, 12801 E. 17th Ave L18-8400, Aurora, CO 80045, USA. E-mail: william.robinson@cuanschutz.edu
Accepted Nov 19, 2020; Epub ahead of print Nov 26, 2020
Acta Derm Venereol 2021; 101: adv00362.
doi: 10.2340/00015555-3709
Telangiectasia macularis eruptiva perstans (TMEP) is a rare cutaneous mastocytosis that has a high frequency of progression to systemic disease, including aggressive systemic mastocytosis (ASM). We describe successful treatment of refractory TMEP that progressed to ASM in a 35-year-old woman who failed multiple lines of therapy until receiving a new targeted agent, avapritinib (BLU-285) in a clinical trial IRB 15-2178 on November 2016. Within 8 weeks of treatment with avapritinib, her symptoms resolved, and she achieved complete remission for over 3 years.
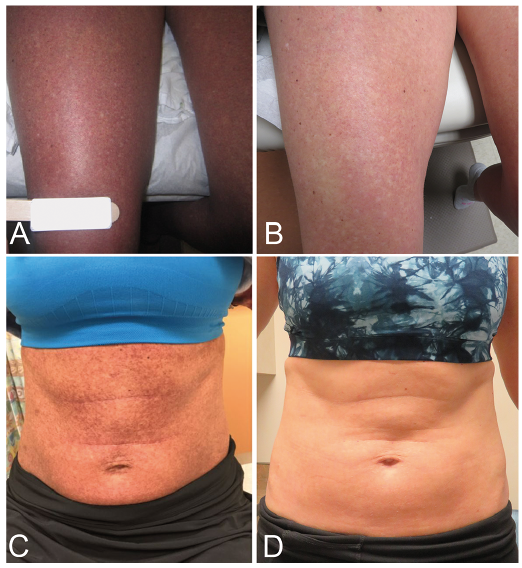
In 2007, a 35-year-old woman developed a pruritic rash on her left thigh that progressed to both thighs over 5 years (Fig. 1A). On initial exam, the rash consisted of diffuse, erythematous macules with telangiectasia, lacking papules and Darier’s sign, resembling the rare disorder, TMEP. Skin biopsy revealed moderate infiltrate of mast cells in a perivascular and interstitial distribution associated with superficial telangiectasia confirming TMEP with D816V mutation in KIT in skin (Fig. 2A). Otherwise, all hematological and chemical laboratory values were within normal limits. PUVA, narrow band UV radiation, and 30 Gy in 10 fractions of electron beam radiotherapy were all ineffective. The rash progressed to her whole body including the abdomen, chest, arms, and face (Fig. 1C). In 2012, she developed abdominal pain and diarrhea. CT of abdomen and pelvis revealed new hepatosplenomegaly with ascites. Biopsy of colon revealed pan-colonic infiltration by mast cells. Bone marrow biopsy revealed a hypercellular marrow of > 90% cellularity with 10–20 % of cells found CD117 and CD25 positive atypical mast cells within multifocal clusters consistent with aggressive systemic mastocytosis (ASM) (Fig. 2C). Treatment with cladribine (a purine nucleoside analogue) then cabozantinib (a tyrosine kinase inhibitor of VEGF) improved the rash, but with unacceptable systemic toxicity. A repeat bone marrow biopsy contained over 35% mast cells. Despite two cycles of nivolumab (an immune checkpoint inhibitor of PD-1), her disease progressed and serum tryptase level rose to 60 ng/ml (Fig. 3).
Fig. 1. Skin photographs of initial presentation and post-treatment with avapritinib. (A) Initial presentation of telangiectatic, erythematous macules on bilateral thighs. (B) Resolved telangiectatic, erythematous macules on bilateral thighs after avapritinib. (C) Telangiectatic, erythematous macules progressed to whole body including abdomen. (D) Resolved telangiectatic, erythematous macules on abdomen after avapritinib.
Fig. 2. Pathology of skin and bone marrow pre- and post-treatment with avapritinib. (A) Skin biopsy with increased number of mast cells in a perivascular and interstitial distribution associated with superficial telangiectasias, consistent with telangiectasia macularis eruptiva perstans (H&E stain, 12.6x magnification). (B) Skin biopsy after avapritinib without atypical population of mast cells (H&E stain, 12.6x magnification). (C) Bone marrow biopsy revealing hypercellular marrow of > 90% cellularity with 10–20% CD117- and CD25-positive atypical mast cells within nodules consistent with systemic mastocytosis (H&E, 12.6x magnification). (D) Bone marrow biopsy after BLU-285 with normocellular marrow negative for increased mast cells. (H&E, 12.6x magnification).
Fig. 3. Serum tryptase level during treatment. Note the downtrend after start of avapritinib and again with the increased dose of avapritinib.
She enrolled in clinical trial IRB 15-2178 in November 2016, using oral avapritinib (BLU-285, a targeted KIT inhibitor) 130 mg daily. Her rash and diarrhea resolved over 10 weeks (Figs 1B, D, and 2B) along with elevated serum tryptase level (Fig. 3), hepatosplenomegaly, and ascites. Bone marrow biopsy after two years of treatment revealed complete remission with a mildly hypocellular marrow (40%) with active trilineage hematopoiesis without increased CD 117 mast cells (Fig. 2D). Despite histologic clearance of abnormal mast cells, the KIT (D816V) mutation was detected in the bone marrow by PCR. Due to grade 2 fatigue, avapritinib was reduced to 100 mg daily after 17 months. After 38 months in January 2020, she relapsed with 10–20% mast cells in the bone marrow with a rise in serum total tryptase from 8 to 23 ng/ml without cutaneous lesions. Avapritinib was increased to 200 mg and after 6 months, she achieved complete remission with detectable KIT mutation by PCR.
Mastocytosis is a clonal hematopoietic stem cell disorder with mast cell expansion and accumulation. Most cases have an acquired driver mutation, somatic exon 17 KIT activating point mutation D816V (1). TMEP is an old terminology of a rare type of cutaneous mastocytosis (CM) that has a high frequency of progression to systemic disease, including ASM (2). TMEP is now reclassified under the term maculopapular cutaneous mastocytosis (MPCM) (3). To our knowledge, we describe the first and successful treatment of avapritinib for refractory MPCM in a 35-year-old woman who failed multiple lines of therapy. Within 8 weeks of treatment with avapritinib, her skin lesions resolved, and she achieved complete remission for over 3 years.
Current treatment for CM is oriented to reducing symptoms including antihistamines, cromoglycates, and anti-leukotrienes. Given the high risk of progression to devastating systemic diseases, CM, should be monitored for systemic involvement. Our patient met WHO criteria for ASM with major criteria of multifocal, dense infiltrates of mast cells aggregates detected in sections of bone marrow and extracutaneous organs of colon; minor criteria of D816V KIT mutation in bone marrow and skin, mast cells expressing both CD117 and CD25 in bone marrow, and serum tryptase level persistently over 20 ng/ml; C-findings of palpable hepatosplenomegaly and ascites.
If refractory to symptomatic therapy, in addition to workup for systemic involvement, patient with CM should be considered for systemic treatment targeting its driver mutation. Once the marrow is involved, minimal residual disease status should be monitored after initiation of systemic therapy, as it may be a predictor of relapse as seen in our case.
Avapritinib is a selective type I KIT D816V inhibitor. Type I inhibitors, unlike type II inhibitors binding to inactive kinase conformations, bind to the active conformation, leading to higher potency (4). Evans et al. (4) demonstrated superior efficacy compared to another type I inhibitor, dasatinib, and type II inhibitors (imatinib, sunitinib, regorafenib) both in vitro and in vivo. A phase 1 EXPLORER trial (NCT02561988) demonstrated decrease in bone marrow mast cells in advanced SM, as seen in our patient (5). Based on the promising results of phase 1 NAVIGATOR trial (NCT02508532), U.S. Food and Drug Administration has recently approved for its use in advanced gastrointestinal stromal tumor, another malignancy with acquired driver mutation of KIT/PDGFRA (6, 7). Common side effects are edema, anemia, and thrombocytopenia. Most reports are grade 1 or 2, and half of all patients reported greater than grade 3 without any discontinuation of the trial.
We report a successful and durable treatment of refractory CM, a debilitating mast cell disorder that has a high risk of progressing to systemic mastocytosis, that developed ASM. Our result raises consideration of additional treatment modality of refractory CM with systemic therapy, especially with targeted agents such as avapritinib.


 Click to show fullsize
Click to show fullsize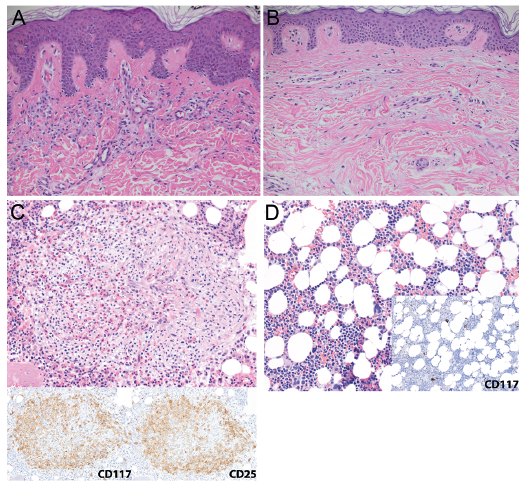 Click to show fullsize
Click to show fullsize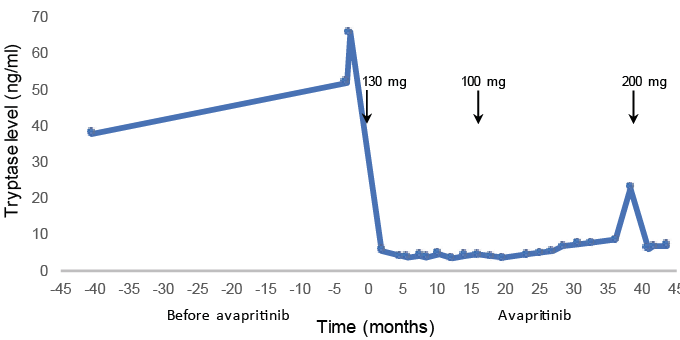 Click to show fullsize
Click to show fullsize