


1Dermatology Clinic, Department of Medicine and Ageing Science and 4Department of Medical Oral Science and Biotechnology, University G. D’Annunzio Chieti-Pescara, 2Department of Dermatology, University of Brescia, Brescia, and 3Istituto di Chirurgia e Laserchirurgia in Dermatologia, Milan, Italy
Basosquamous carcinoma is a rare clinical entity, which comprises 1.7–2.7% of all skin carcinomas. It is described as a basal cell carcinoma with features of squamous differentiation. To date, studies of the epidemiology of basosquamous carcinoma have been few and small in size. We report here the most extensive series of basosquamous carcinomas published to date, highlighting the differences between basosquamous carcinoma and other keratinizing tumours. Patients undergoing surgical excision for keratinizing tumours were enrolled in this study. Age, sex and tumour characteristics were recorded. A total of 1,519 squamous cell carcinomas, 288 basosquamous carcinomas and 4,235 basal cell carcinomas were collected. Basosquamous features were compared with those of basal cell and squamous cell carcinomas. For basosquamous carcinomas, 70.5% were located on the head and neck, particularly on the nose, forehead and cheeks, and represented almost 10% of the keratinizing tumours on the ears. Significant differences were found between basosquamous carcinoma and basal cell or squamous cell carcinomas. Basosquamous carcinoma should be considered a distinct type of keratinizing tumour with different anatomical, sex and age distributions.
Key words: basosquamous carcinoma; basal cell carcinoma; keratinizing tumour; squamous cell carcinoma; skin tumour.
Accepted Nov 27, 2020; Epub ahead of print Dec 3, 2020
Acta Derm Venereol 2021; 101: adv00353.
doi: 10.2340/00015555-3710
Corr: Simone Soglia, Department of Dermatology, University of Brescia, Piazzale Spedali Civili 1, IT-25123 Brescia, Italy. E-mail: simone-soglia@libero.it
Basosquamous carcinoma (BSC) represents a clinically and histologically ill-defined skin neoplasm with an aggressive behaviour, significant metastatic potential (1) and a high risk of recurrence (2, 3). It is frequently described as a basal cell carcinoma (BCC) with features of squamous differentiation (4), but there is a lack of a clear histological definition.
Although this description is considered a requisite for diagnosis of BSC, there is no clear understanding of how these features should present to fulfil the diagnosis (4).
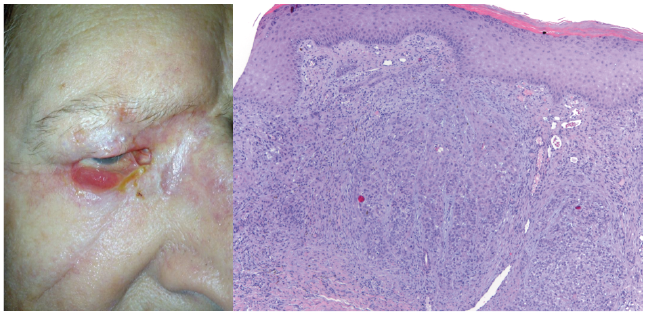
Confusion regarding this tumour was increased by the several terms used for its reporting: mixed carcinoma, metatypical carcinoma, basal cell carcinoma with squamoid differentiation, and keratotic basal cell carcinoma. Some authors even considered that BSC could be a keratinizing BCC, a collision tumour between a BCC and a squamous cell carcinoma (SCC), or a BCC evolved towards a BSC (5, 6). Nonetheless, today, BSC is recognized as an independent entity (7). Histologically, BSC shows areas of mitotically active basaloid cells and polygonal squamoid cells with eosinophilic cytoplasm, separated by the variable presence of a transition zone (3, 8). Clinically, BSC often presents with a non-specific aspect, making it difficult to distinguish from other keratinizing tumours (KTs) (Fig. 1). Dermoscopic diagnosis could be suggested by the presence of both BCC-dominant polymorphous vasculature and SCC-dominant findings of keratinization (9). In particular Giacomel et al. (10) found that the most frequent dermoscopic criteria for BSC were: unfocused peripheral arborizing vessels in association with keratin masses and white structureless areas. Epidemiologically, BSC is considered a rare tumour, representing 1.7–2.7% of all skin carcinomas (4, 11). To date, few studies have directly evaluated the epidemiology of BSC, and most of these studies were small in size due to the relatively recent histological definition of this clinical entity (3, 8, 12, 13).
The aim of this paper is to report the most extensive series of BSC to date, and to determine the differences between BSC and other KTs, in order to share our experience and define the epidemiological features of BSC.
Fig. 1. Clinical and histological details of a basosquamous carcinoma of the lower eyelid in an 85-year-old man. Basaloid cells and eosinophilic polygonal squamoid cells with no transition zone. Hematoxylin-Eosin staining 10x magnification.
This prospective study enrolled all patients scheduled to undergo surgical excision for KT at the Department of Dermatology of the Spedali Civili, Brescia, Italy, between January 2012 and December 2015. For each patient: age, sex and tumour characteristics, including anatomical site, were recorded. All surgical excisions were performed according to the current international guidelines for each tumour type. Two independent pathologists evaluated all the skin lesions; in the case of disagreement about the diagnosis a third pathologist was consulted. Tumours that were histopathologically diagnosed as BCC, BSC or SCC were included in the final analysis. Histological types of BCC were identified as superficial, nodular and infiltrative/morpheaform, while SCC were divided into superficial and invasive. The diagnosis of BSC was made in the presence of both of the following histopathological criteria: areas of small, mitotically active, hyperchromatic basaloid cells; and large polygonal squamoid cells with eosinophilic cytoplasms, with a transition zone between them. Patients who had 2 or more tumours diagnosed were counted as 2 or more tumour cases.
Ethical aspects
The study was performed in accordance with the principles of the Declaration of Helsinki. All patients provided written informed consent.
Statistical analysis
The categorical variables: sex, age, general anatomical location, and anatomical site, were summarized as frequencies (row percentages). Pearson χ2 test was used to test independence, and p-values for pairwise comparisons were adjusted by Bonferroni correction. To determine the association between exposure factors and types of tumours, the relative risks (RRs) and 95% confidence intervals (CIs) were calculated. Collected data were analysed using IBM SPSS 25.0 software (SPSS Inc., Chicago, IL, USA). All results were considered statistically significant for p-values < 0.05.
A total of 6,042 KTs were collected, and stratified as follows: 1,519 SCCs (25.1%), 288 BSCs (4.8%) and 4,235 BCCs (70.1%). Of these patients, 2,522 were female and 3,520 were male. The mean age of the female patients was lower (69.30 ± 15.0 years) than that of the male patients (70.79 ± 12.3 years) (p = 0.13*). Most of the KTs were located on the head and neck (3,936; 65.1%), 1,262 were on the trunk (20.9%), 340 on the legs (5.6%), 494 on the arms (8.2%), and the remainder (0.2%) were on the genitals and oral mucosa (Fig. 2). BSC represented 6.4% of all BCCs. Compared with all KTs by anatomical site, most BSCs developed on the head and neck area: nose (6.75%), lips (6.95%) and ears (9.45%), while fewer were found on the upper limbs (5.02%) and lower limbs (6.28%) (Fig. 3). The BSC population was 64% male and 36% female. Fig. 4 shows the distribution of the 3 skin neoplasm populations by anatomical site: 203 (70.5%) BSCs were located on the head and neck, 41 (14.2%) on the trunk, 23 (8%) on the arms, and 21 (7.3%) on the legs; no BSCs were found on the genitals or mucous membranes. In the head and neck area, the highest number of BSCs was located on the nose (47 tumours), followed by the forehead (46 tumours) and cheeks (34 tumours).
Fig. 2. Distribution of keratinizing tumours by anatomical location.
Fig. 3. Percentage of basosquamous carcinoma compared with all keratinizing tumours by anatomical site. Red line corresponds to the mean of the distribution.
Fig. 4. Distribution of skin neoplasms by anatomical site. Red rectangles: statistically significant p-values < 0.001.
The anatomical location of the relative numbers of BSCs was compared with BCC, SCC and KT (BCC+SCC) groups. Compared with BCCs, a significantly higher number of BSCs was present on the lower limbs (p = 0.025*, RR 1.67) and ears (p < 0.001*, RR 3.64), while a lower number was located on the back (p < 0.001*, RR 0.48) and on the chest/abdomen (p = 0.022*, RR 0.61). More BSCs than SCCs were located on the nose (p < 0.001*, RR 2.05), eyelids (p = 0.021*, RR 2.23), back (p < 0.001*, RR 2.64) and chest/abdomen (p = 0.024*, RR 1.76), while more SCCs were found on the hands (p = 0.003*, RR 0.16) and scalp p = 0.001*, RR 0.46).
When comparing the number of BSCs with the total number of other KTs (BCC+SCC) significant differences were found for localization on the nose (p = 0.009*, RR 1.45), ears (p < 0.001*, RR 2.09) and back (p = 0.019*, RR .62).
Finally, BSCs were divided into age groups and their distribution compared with that of BCCs and SCCs (Table I). In the current cohort 178 BSCs (61.8%) were found in patients over 80 years of age and only 10 (3.47%) in people under 50 years of age. BSCs are less frequent than BCCs in the age range 50–79 years. A significantly higher number of BSCs were found in the 80–89 years (p < 0.001*, RR 1.54) and 90–99 years (p < 0.001*, RR 12.23) age groups compared with the age distribution in the BCC group. Fewer BSCs were found in the 60–79 group compared with the age distribution in the SCC group, while more BSCs were found in the 50–59 years (p = 0.023*, RR 1.83) and the 90–99 years (p < 0.001*; RR 4.62) age groups. No differences in prevalence were found between BSCs and SCCs in the 8th decade.
Table I. Prevalence of basosquamous carcinoma (BSC) in different age groups compared with other keratinizing tumours
The frequency (row percentage) for sex, general anatomical location, and age variables, and p-values and pairwise comparison results from the χ2 test are shown in Table II. All exposure variables were statistically different across the KT groups; in particular, 72.0% of females and 68.7% of males were in the BCC group. By comparison, in the BSC and SCC group, respectively, males were 183 (5.2%) and 917 (26.1%) and females 105 (4.2%) and 601 (23.8%). There was a significant association between type of tumour and age according to the χ2 test (p < 0.001). Indeed, post-hoc tests showed that the only pairwise comparisons confirming independence were the pairs of classes: < 50 vs 50–59 years and 80–89 vs 90–99 years.
Table II. Frequency (row percentage) for sex, general anatomical location, and age
BSC is considered a rare skin tumour, but data about its incidence are poor and fragmentary. Martin et al. (3) reported 31 cases of BSC from a total of 2,075 skin carcinomas (1.5%) treated at the University of Louisville-affiliated hospitals between 1985 and 1988. In a review of 1,000 consecutive cases of Mohs surgery performed on histologically confirmed KTs, Bowman et al. (13) found 27 BSC (2.7%). Again, in a comparative study of 2,565 KTs of the head and neck, Schuller et al. (12) reported 33 BSC (1.3%). All of these studies have a limited number of patients and were retrospective.
The current prospective cohort of 6,042 KTs, included 288 BSCs, with an incidence of 4.8%, which is higher than that found previously in the literature. According to existing data, a male predominance was registered, with 64% of BSCs affecting men. A number of studies have analysed the anatomical distribution of BSCs, documenting that this type of tumour is most commonly located on the head and neck (2, 3, 13). Some authors have reported up to 95% of cases of BSCs being treated with Mohs surgery in this anatomical region (14); most commonly on the nose (33.1%), auricular area (18.5%) or periocular area (11.2%). However, it must be considered that there may be a referral bias for treatment of facial tumours with Mohs surgery. Only 70.5% of the BSCs in the current study were localized on the head and neck, with the majority of tumours found on the nose, forehead and cheeks. Analysis of the different anatomical sites revealed that it was easier to find a BSC on the ears, lips and nose; in particular they represent 9.45% of all tumours located on the auricular region. These findings suggest that some of the more aggressive BCCs found in the “H area” of the face could, in fact, be BSCs. In the current study the distribution of BSCs in the different anatomical regions appears to differ from that of other KTs. The majority of cases of BSCs in the current study were found in the eighth decade of life (34.4%). BSCs distribute differently from the other KTs in the various age groups and, interestingly, a significantly higher number was found in patients over the age of 90 years compared with the other tumours (in the current population BSCs represented 29.9% of the tumours in this age group). Several statistically significant differences were found in the distribution of BSCs compared with both BCCs and SCCs, suggesting that this skin tumour may represents a separate entity with a specific biological behaviour. This evidence is supported by several data in the literature (3, 11, 13). Tan et al. (10) reported a recurrence rate of 8.9% after Mohs surgery and 12–45.7% after wide local excision. Bowman et al. (12), analysing 1,000 skin tumours after Mohs surgery, reported a prevalence of pulmonary metastasis in 7.4% of cases of BSC, compared with 0.87% of cases of SCC. Martin et al. (3) reported 5 cases of lymph node metastasis, 9 cases of recurrence and one of pulmonary metastasis in a cohort of 28 BSCs.
No specific guidelines exist for the treatment of BSC. The surgical risk of incomplete exeresis in this tumour appears to be similar to that of BCCs, depending on the site, size and whether primitive or recurrent. The biological behaviour is comparable with SCC because of the risk of progression and metastasis. Thus, the best therapeutic options appear to be either wide surgical excision of the lesion (15), Mohs micrographic surgery, or re-surgical evaluation with reflectance confocal microscopy (16). The last approach can help to minimize incomplete excisions, even though some studies have highlighted that BSCs less frequently show deep involvement of surgical margins, compared with other BCC subtypes (17). As most of the significant prognostic factors reported for recurrence (tumour size >2 cm, lymphatic invasion, male sex, perineural invasion, and positive surgical margins) (6) coincide with those specific for SCCs, and considering that BSCs frequently manifest as locally advanced disease or show lymph node metastasis at presentation, a post-surgical approach with frequent follow-ups and lymph node ultrasound are essential. The characteristics of locally advanced, inoperable and metastatic lesions suggest an approach to this neoplasm as for advanced SCC, using current protocols for this latter type of KT (18).
In conclusion, this prospective study demonstrates that also for the different anatomical, sex and age distribution, BSC should be considered a distinct, separate kind of KT.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize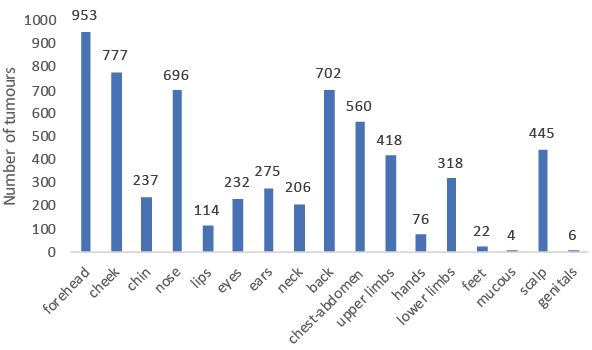 Click to show fullsize
Click to show fullsize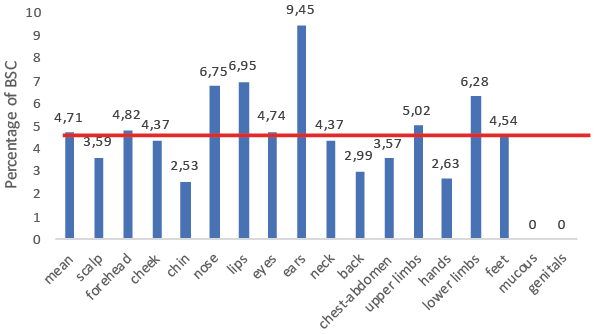 Click to show fullsize
Click to show fullsize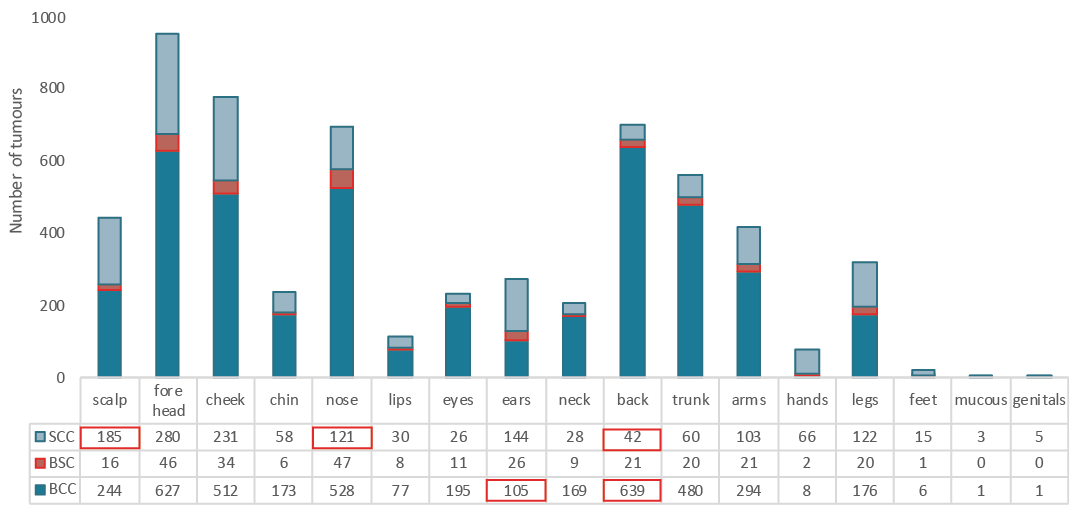 Click to show fullsize
Click to show fullsize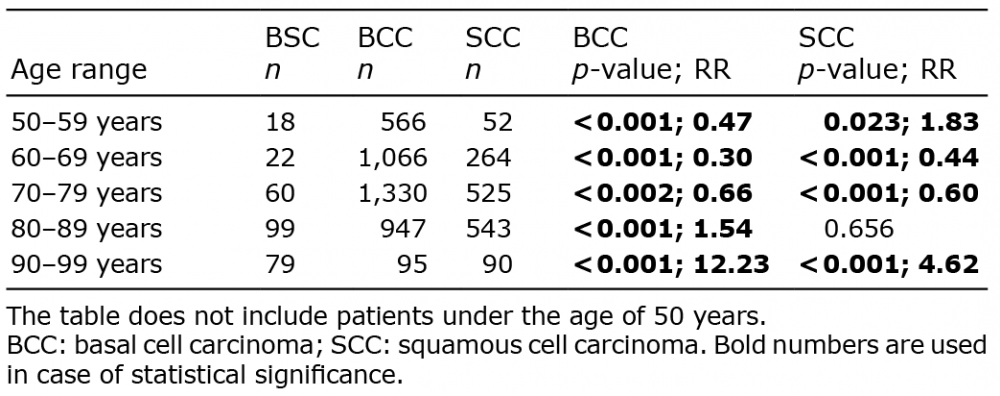 Click to show fullsize
Click to show fullsize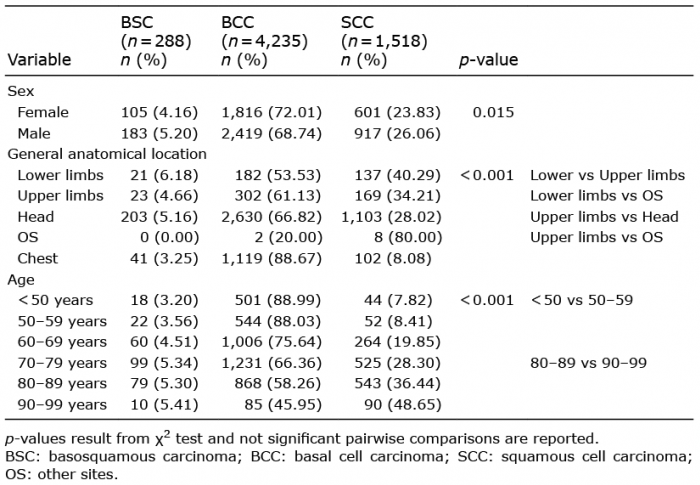 Click to show fullsize
Click to show fullsize