


1Department of Dermato-Venereology, Copenhagen University Hospital, Bispebjerg Hospital, 2Department of Biomedical Sciences, University of Copenhagen, 3Department of Clinical Microbiology, Copenhagen University Hospital, Hvidovre Hospital, and 4Institute of Clinical Medicine, University of Copenhagen, Copenhagen, Denmark
The aim of this study was to investigate the characteristics of patients co-infected with Chlamydia trachomatis and Neisseria gonorrhoea. A retrospective case-control study was performed, which included 399 co-infected patients seen at a sexually transmitted infection clinic in Copenhagen, Denmark. Case-control groups included 300 patients who tested positive only for N. gonorrhoea, 300 who tested positive only for C. trachomatis, and 300 who tested negative for both N. gonorrhoea and C. trachomatis in the same study period. For men, non-Danish origin (odds ratio (OR) 2.3, 95% confidence interval (Cl) 1.34–4.12), previous sexually transmitted infections with C . trachomatis (OR 3.3, 95% CI 1.94–5.92) and N. gonorrhoea (OR 10.6, 95% CI 6.36-17.76), and higher number of sex partners (OR 1.7, 95% Cl 1.40-2.28) were significantly associated with diagnosis of co-infection. For women, previous sexually transmitted infections with C. trachomatis (OR 6.7, 95% CI 3.89-11.78) and N. gonorrhoea (OR 10.4, 95% CI 4.99-21.71), and higher number of sex partners (OR 1.8, 95% CI 1.28-2.56) were significantly associated with a diagnosis of co-infection, whereas being of non-Danish origin was, in some cases, a protective factor (OR 0.3, 95% CI 0.17-0.69). Furthermore, this study demonstrated sex-associated characteristics that should raise concern about co- infection, including: for men, being of non-Danish origin, men who have sex with men status, and higher age, and, for women, young age, in particular, and previous sexually transmitted infections.
Key words: chlamydia; gonorrhoea; co-infection.
Accepted Dec 9, 2020; Epub ahead of print Dec 15, 2020
Acta Derm Venereol 2021; 101: adv00356.
doi: 10.2340/00015555-3721
Corr: Farnam Barati Sedeh, Department of Dermato-venereology, Copenhagen University Hospital, Bispebjerg Hospital, Bispebjerg Bakke 23, DK-2400 Copenhagen NV, Denmark. E-mail: farnam07@hotmail.com
Neisseria gonorrhoea and Chlamydia trachomatis are curable sexually transmitted infections of public health importance. It has been suggested that patients with one of these diseases are often simultaneously infected with the other. However, few current data are available regarding the characteristics of co-infected patients. This study demonstrates that chlamydial and gonococcal infections at the same time affect younger women and men who have sex with men, and further demonstrates a strong association between co-infection and previous sexually transmitted infections. This is important in order to investigate which patients in clinical practice might be co-infected and which risk factors in men and women are associated with co-infection.
Neisseria gonorrhoea (NG) and Chlamydia trachomatis (CT) are curable sexually transmitted infections (STIs) of public health importance. The Danish Health Authority estimates that approximately 3,500 infections with NG (1) and 50,000 infections with CT (1) are diagnosed in Denmark each year. In women, these infections are often asymptomatic, which may lead to serious health consequences, such as ectopic pregnancy, infertility and an increased risk of pelvic inflammatory disease (2, 3). Furthermore, it has been suggested that STIs, including gonorrhoea and chlamydia, facilitate the transmission and acquisition of HIV (4). Also, a high risk of reinfection has been found among persons with these STIs (5–7).
Patients infected with NG are often reported to be simultaneously infected with other sexually transmissible diseases; the most common association reported is NG/CT co-infection (8). In 1982, the US Centers for Disease Control and Prevention (CDC) suggested that CT co-existed in up to 45% of patients infected with NG (9).
However, various levels of co-infection with CT have been reported since; 4–64% in attenders at sexually transmitted diseases clinics (10–14). Risk factors associated with NG/CT co-infection vary, based on different studies, and include age, sex work, and drug/alcohol use (15–17). Adolescents and young adults are at higher risk of co-infection because their rates of partner change are, on average, higher than for older adults, they may be more likely to engage in unprotected sexual intercourse, and may choose partners who are at higher risk (18). Men who have sex with men (MSM) have been reported to be more likely to harbour co-infections than do heterosexual males (19). Co-infection has been linked with increased risk of re-infection with CT or NG when retested between 6 weeks and 6 months, NG re-infection in a high NG prevalence population and CT re-infection in women (15, 16, 20). Mathematic modelling studies have found that each infection could increase susceptibility and/or transmissibility of the other, and that the bacterial load might be higher in CT/NG co-infection than in NG alone (21).
With various levels of co-infection reported to date, based on different populations, and increasing interest in the development of new treatments and vaccines against NG/CT co-infection, more data are essential to improve understanding of the characteristics and risk factors associated with this co-infection.
The aim of this study was to describe the characteristics of patients tested for NG and CT, and to compare co-infected patients, patients infected only with NG, and those infected only with CT, with patients tested negative for both NG and CT.
Study design
A retrospective case-control study was performed, including 399 patients co-infected with NG and CT seen at a STI clinic in Copenhagen, Denmark, during the period 1 October 2015 to 31 October 2017. Case-control groups included 300 patients tested positive only for NG, 300 patients tested positive only for CT, and 300 patients tested negative for both NG and CT within the same study period. A combined CT/NG test was used in our clinic; thus, every patient with NG was also tested for CT, and every patient with CT was tested for NG.
The STI clinic at Copenhagen University Hospital, Bispebjerg Hospital, is the largest in Denmark and has approximately 100 daily consultations. All Danish- or English-speaking patients who had a personal identification number (PIN) and were seen at the clinic for STI testing were eligible for the study. The Danish PIN is a unique identification number which is used in all public instutions including the Danish healthcare system. Patients who opted for anonymous STI testing or whose medical history did not include information on demographic and behavioural characteristics were excluded.
Laboratory data, including all NG and CT tests performed within the study period, were obtained from the Department of Clinical Microbiology, Copenhagen University Hospital, Hvidovre Hospital and linked to patient data using the PIN.
During the study period, a total of 2,990 patients tested positive only for NG, 2,407 patients tested positive only for CT, and 500 patients tested negative for both NG and CT. Among the co-infected patients, full medical records were available for only 399 patients. Case-control groups were identified among patients tested in the same study period, and included 300 patients who tested positive only for NG, 300 who tested positive only for CT, and 300 who tested negative for both NG and CT. The study population thus included: (i) patients co-infected with NG and CT (n = 399), (ii) patients infected only with NG (n = 300), (iii) patients infected only with CT (n = 300), and (iv) patients who tested negative for both NG and CT (n = 300).
The following data were collected from the patient records: sociodemographic information, sexual orientation (heterosexual, men who have sex with men (MSM), women who have sex with women (WSW)), history of previous STIs, HIV status, and sexual risk behaviour). Testing was conducted on a voluntary basis and medical staff obtained the samples. All samples were analysed at the Department of Microbiology, Hvidovre Hospital, using nucleic acid amplification test (NAAT); transcription-mediated amplification (TMA), Aptima, Hologic Inc., Massachusetts, USA. Furthermore, samples tested positive for NG were subject to culturing and resistance testing. In addition, patients were offered screening for HIV and syphilis.
Definitions
Co-infection was defined as a positive NAAT result for both NG and CT from any tested location (throat, rectum, urethra, cervix and/or vagina). Infection with NG only was defined as a patient with a positive NAAT result for NG (and all samples negative for CT); infection with CT only was defined as a positive NAAT result for CT (and all samples negative for NG). The non-infected group had negative NAAT results for both NG and CT. Non-HIV was defined as patients with a negative HIV test and patients never tested for HIV (all patients are offered HIV testing and only a minority have never been HIV tested). Time since exposure (in days) was defined based on the last sexual exposure. Sexual risk behaviour was defined as trading (buying/selling) sex for money, drugs, or having sex with a person from a known risk group, i.e. with a person with STI, a sex worker, or a partner of non-Danish origin. Non-Danish was defined as those who were not born in Denmark. Previous history of STIs was defined as lifetime STIs. Length of time for sexual risk behaviour was the last 6 months. Men who had sex with both men and women were also categorized as MSM. Women undergoing gynaecological examination were tested from the urethra and cervix, whereas women without symptoms performed vaginal self-sampling. Men who reported same-sex sexual contact were tested from the throat, urethra and rectum, whereas all other men were tested from urethra as standard care. Patients who reported receptive oral sex were tested from the throat. Patients who reported anal sex were tested for anal CT/NG NAAT. Furthermore, sample collection was performed according to the clinical indication and the risk behaviour of the patient.
Patient who tested positive for gonococci were treated at the STI clinic free of charge and seen at a follow-up visit for re-testing after 2 weeks. Patients who tested positive for CT were prescribed relevant antibiotic treatment and were not seen at follow-up visit. All patients with positive tests results were encouraged to inform current and former sexual partners of the test results, and these individuals were offered testing at the STI clinic
Statistical analysis
First, univariate analyses was performed to assess whether there was a difference between patients with co-infection, those infected only with NG or CT, or the non-infected group, based on demographic and behavioural characteristics. Secondly, multinomial logistic regression analysis was performed to study whether co-infection was associated with any specific demographic or behavioural characteristics, compared with infection with NG only, CT only, and non-infected groups. All 3 infected groups were simultaneously compared with the reference group (non-infected). All variables were included in a single multinomial statistic model. Results were reported as adjusted odds ratio (OR) and 95% confidence intervals (95% CI). Adjusted OR and p-values were adjusted for age, sexual orientation, country of birth, time since exposure, previous STIs, HIV status, risk behaviour and number of sex partners. Time since exposure was defined as risk per 5 days (by dividing the time since the last sexual exposure in days by 5), sex partners was defined as risk per 5 partners, and age was defined as risk per 5 years (by dividing the patient’s age by 5). An entry of “1” in the results (for being MSM, Danish, HIV-infected and no sexual risk behaviour) is based on the fact that this is a category data, where 0 is defined as not being MSM, Danish, HIV-infected and not having sexual risk behaviour, and one is defined as being MSM, Danish, HIV-infected and having sexual risk behaviour. The analysis was performed using IBM SPSS Statistics version 24 SPSS Inc., Chicago, USA. The study was approved by the Danish Data Protection Agency and the Danish Patient Safety Authority (study i.d. numbers 05849 and BFH-2017-088).
Demographic characteristics
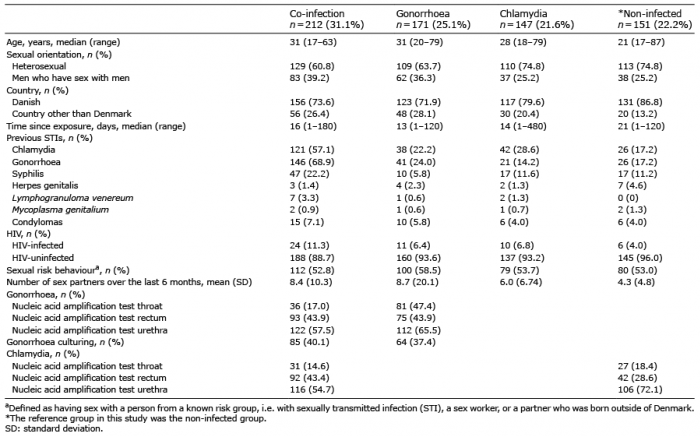
Among the 399 patients who had co-infection with NG and CT, 212 (53.1%) were men and 187 (46.9%) were women. Based on the self-reported sexual orientation of the participants, it was estimated that 220 (32.3%) of the men were MSM and 67 (10.8%) of the women were WSW (Tables I and II).
Men diagnosed with co-infection and men diagnosed only with NG were older than those with only CT and the non-infected men (Table I). However, women diagnosed with co-infection were younger than those with only NG and only CT, but older than the non-infected women (Table II). Compared with heterosexual men, MSM were more often diagnosed with co-infection (Table I). Co-infected men and men only diagnosed with NG were more often of non-Danish origin compared with men with only CT and non-infected men. Also, co-infected women were more often of non-Danish origin in when comparing the 4 groups before any statistical analyses were performed (Table II).
Table I. Characteristics of the 681 men participating in the study
Table II. Characteristics of the 618 women participating in the study
Previous sexually transmitted infections and HIV
Co-infected men more often reported previous infections with chlamydia, gonorrhoea, syphilis and Lymphogranuloma venereum (LGV) compared with the other groups (Table I). Correspondingly, co-infected women more often reported previous infection with chlamydia, gonorrhoea and syphilis compared with the other groups (Table II). All men diagnosed with LGV were MSM, as were most men diagnosed with syphilis. Co-infected men more often had concurrent HIV compared with other men, whereas very few women in the study were HIV-infected (Tables I and II).
Risk behaviour
Co-infected men and women had the longest period of time from exposure to testing compared with the NG-only and CT-only groups, whereas the non-infected men and women were the last group among all patients contacting a STI clinic to be tested (Tables I and II). Men, irrespective of group, reported more sexual risk behaviour and higher number of sexual partners compared with women (Tables I and II). Notably, co-infected men and women both reported less sexual risk behaviour than all other groups (Tables I and II).
Risk factors associated with co-infection
Compared with the non-infected men, previous infection with CT (OR 3.3, 95% CI 1.94–5.92), NG (OR 10.6, 95% CI 6.36–17.76), being of non-Danish origin (OR 2.3, 95% CI 1.34–4.12) and increasing number of sex partners (risk per 5 partners) (OR 1.7, 95% CI 1.40–2.28) were associated with diagnosis of co-infection among men (Table III). However, increasing age was considered a protective factor against co-infection (OR 0.9, 95% CI 0.85–0.96) (Table III). For women, previous infection with CT (OR 6.7, 95% CI 3.89–11.78), NG (OR: 10.4, 95% CI 4.99–21.71), and increasing number of sex partners (OR 1.8, 95% CI 1.28–2.56) were associated with diagnosis of co-infection (Table IV). However, for women, multinomial logistic regression analysis found that being of non-Danish origin (OR 0.3, 95% CI 0.17–0.69) was a protective factor against co-infection (Table IV).
Table III. Factors associated with diagnosis of co-infection, gonorrhoea and chlamydia compared with non-infected men*
Table IV. Factors associated with diagnosis of co-infection, gonorrhoea and chlamydia compared with non-infected women*
A main finding of this study is that co-infection with NG and CT is highly associated with previous STIs. Both men and women with co-infection were more likely to have been previously infected with NG and CT. In addition, an association was found between higher number of sex partners and NG and/or CT infection, compared with non-infected patients. The high risk of reinfection found in this study is in line with findings from a study of STI repeaters in Massachusetts, USA, which concluded that a small subpopulation of high-volume repeaters was likely to have high impact on STI and HIV rates (6).
Surprisingly, co-infected patients of both sexes reported less sexual risk behaviour than all other groups. This was supported by multinomial logistic regression analysis, which could not demonstrate any association between co-infection and increased risk behaviour. An explanation could be that co-infected patients are part of a subpopulation with a high STI burden. This is supported by the fact that co-infected patients had the longest period of time between exposure and STI testing compared with those infected with only NG or only CT. Thus, there is an increased risk of becoming infected with both microorganisms.
This study found a sex distribution of co-infected patients of 53.1% men and 46.9% women. Co-infected women were almost a decade younger than the co-infected men. For men, non-Danish origin was associated with being diagnosed with co-infection, whereas, in women, non-Danish origin was considered a protective factor in the multinomial logistic regression analysis. More detailed information on ethnicity may explain why being of non-Danish origin was apparently a protective factor, even though women of non-Danish origin were overrepresented among co-infected women in the crude characterization of the study participants. One possible explanation is that the group is diverse; many Danish citizens of non-Danish origin originate from Middle Eastern countries and may have fewer sexual contacts, whereas other women of non-Danish origin may have high risk behaviour, such as sex work. The above-mentioned study describing STIs in Massachusetts also found sex differences in high-volume repeaters; here women were younger, non-white, and had no same-sex contacts (6). On the other hand, men spanned the age spectrum, were predominantly white, and the majority reported same-sex contacts (6). The current study also found that women with co-infection were younger compared with other female patients with only NG or CT. This was also demonstrated in a study from UK investigating the occurrence of co-infection among 2,380 patients. The study reported lower age of patients with both infections compared with those with only NG (11). It is only recently that the incidence of gonorrhoea has increased among women; it has been hypothesized that bisexual men pass the infection to heterosexual networks. Another sex difference was seen in reported sexual risk behaviour (characterized by having sex with a person from a known risk group, i.e. with a person with STI, a sex worker, or a partner of non-Danish origin), which was much higher among men (52.8 vs 32.6%).
In this study, the prevalence of HIV was higher among co-infected men than among other men. Conversely, most women in the current study were not HIV-infected; hence this factor could not be investigated further. Other studies have reported that 5–10% of patients receiving treatment at HIV clinics are infected with NG and/or CT at any given time (22), and US guidelines recommend at least one NG/CT screening annually thereafter among patients with HIV (23). In Denmark, STI testing is recommended at least annually and 2–4 times per year for MSM who are sexually active and do not consistently use condoms (24).
The current study found that MSM were somewhat overrepresented in the group of co-infected men, which confirms similar findings from other studies (22, 23), suggesting that expanded screening of MSM (testing also from oral and rectal sites) may contribute to the higher positivity rate among MSM. Screening from these extragenital sites has previously been reported to be as low as <10% (25–27). However, expanded screening has been associated with detection of asymptomatic disease, which is assumed to account for between 50% and 85% of infections at these sites (22, 26, 27).
Due to the retrospective design of the current study it was only possible to draw limited conclusions. Nevertheless, the study is strengthened considerably by the fact that it could access all patient records and link these data to laboratory test results using the unique PIN assigned to all Danish individuals. Furthermore, the healthcare system in Denmark is publicly funded and centralized, which means that all hospital records and laboratory results are filed in a single IT application. For example, if a patient is seen at a HIV clinic and diagnosed and treated for syphilis and thereafter seeks screening for STIs at a STI clinic, all previous patient records and laboratory results are available to the treating physician.
In conclusion, previous STIs are risk factors for new STIs among both men and women, which emphasizes that knowledge about a patient’s medical history is crucial to detect those who are at high risk of new STIs. Furthermore, this study demonstrates that the known disparities in STI epidemiology, in which younger women and MSM bear a disproportionate burden of STI (6), are also applicable in a Danish setting. Consequently, we suggest that physicians testing patients for STIs should be aware of sex-associated characteristics that raise concern about co-infection. For men, these include being of non-Danish origin (significant), MSM status, and higher age; whereas, for women, these characteristics include young age and previous STIs (significant).
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize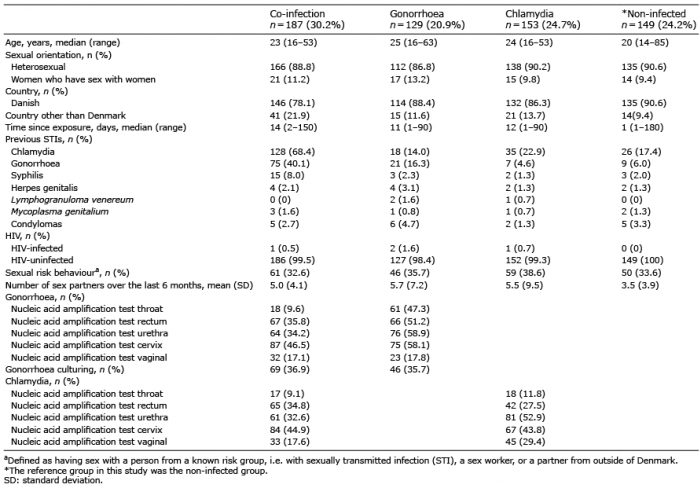 Click to show fullsize
Click to show fullsize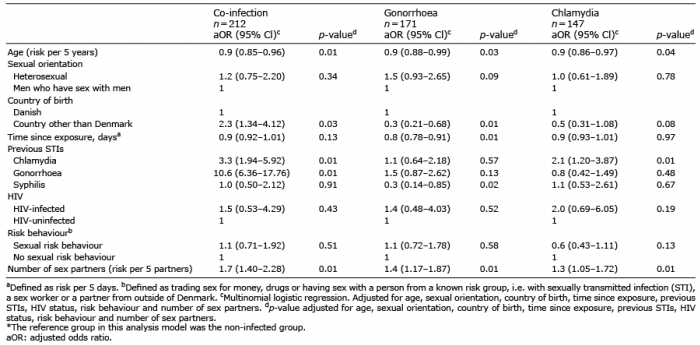 Click to show fullsize
Click to show fullsize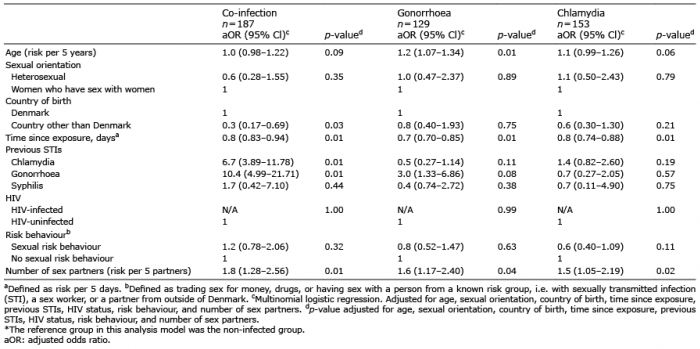 Click to show fullsize
Click to show fullsize