


1Istituto Dermopatico dell’Immacolata-Istituto di Ricovero e Cura a Carattere Scientifico, Dermatological Research Hospital (IDI-IRCCS) and 2Dermatology Unit, “Cristo Re” General Hospital, Rome, Italy
#These authors contributed equally to this research.
The difference between men and women in the impact of keratinocyte carcinomas on quality of life has not been widely studied. This study of 364 patients with keratinocyte carcinoma, measured quality of life using the self-administered 12-item Short Form Health Survey (SF-12) and Skindex-29. Results for both the physical and the mental components of SF-12 were worse in women than in men. For the mental component, women had significantly lower scores compared with men in almost all subgroups, based on demographic and clinical variables. The Skindex-29 emotions mean score was worse in women than in men. Women reported significantly higher level of worry that the disease could get worse and of developing scars, and more depression. On the other hand, men reported lower quality of sleep. The impact of keratinocyte carcinomas on quality of life is generally higher in women than in men. Such data may be important for tailored management of the disease in different categories of patients.
Key words: sex; health status; keratinocyte carcinoma; non-melanoma skin cancer; quality of life; sex.
Accepted Dec 22, 2020; Epub ahead of print Dec 29, 2020
Acta Derm Venereol 2021; 101: adv00439.
doi: 10.2340/00015555-3736
Corr: Francesca Sampogna, IDI-IRCCS (Istituto Dermopatico dell’Immacolata-Istituto di Ricovero e Cura a Carattere Scientifico, Dermatological Research Hospital), Via Monti di Creta 104, IT-00167 Rome, Italy. E-mail: fg.sampogna@gmail.com
Keratinocyte carcinomas, i.e., basal cell carcinomas and squamous cell carcinomas, are common skin tumours. Patients with keratinocyte carcinomas, especially basal cell carcinoma, rarely develop metastasis, and the mortality rate is therefore low. However, these tumours may have a negative impact on patients’ quality of life, due to symptoms, functional limitations, cosmetic burden, treatment, and costs. This study found that the impact of keratinocyte carcinomas on quality of life was different in women and men, with a higher emotional impact in women, especially concerning worry that the disease could get worse and of developing scars, and depression.
Non-melanoma skin cancers (NMSC) are mainly represented by basal cell carcinomas (BCC) and squamous cell carcinomas (SCC), and are the most common cancers in Caucasian individuals (1). More recently, the term “keratinocyte carcinomas” (KC) has been used to distinguish BCC and SCC from the other types of NMSC, because of the shared lineage with epidermal keratinocytes (2). The incidence of KCs is increasing, and it is higher in people aged 65 years or over compared with younger patients, and in white people compared with other ethnic groups (3). Risk factors for KCs include genetic factors, exposure to ultraviolet (UV) radiation, age, skin pigmentation, recreational behaviour, immunosuppression (4), and some types of cutaneous human papillomavirus (in SCCs) (5). Patients with KCs, especially BCC, rarely develop metastasis, and thus the mortality rate is low (6). Nevertheless, a high morbidity for KCs is reported, mostly for patients with head and neck cancer localization, in which higher recurrence and local destruction can occur. The decrement in QoL due to KC is generally small (7, 8). Compared with many other dermatological conditions, KC generally appears as one of the conditions with the smallest impact on QoL (9). However, this impact is not negligible, and may be due to symptoms, functional limitations, cosmetic burden, treatment, and costs (10). This is particularly true when the lesion is localized in the head/neck area. It was observed that, among skin cancers, KCs had a higher impact on the symptomatic component of QoL, while melanoma affected psychological aspects more (11). Differences have also been observed depending on age, with older people with KC reporting a worse health status compared with young patients (12). An interesting aspect, which is worth studying, is the association of QoL impairment with sex. In fact, sex may affect health status and have implications for disease prevention, diagnosis and treatment (13). In general, a higher incidence of KC has been reported in men than in women (14–16), which some have attributed to greater sun exposure in men. However, indoor tanning, which uses artificially produced UV radiation, is more commonly used by women than men. In Europe, the incidence of KCs is increasing in both sexes; however, a faster increase in women than in men has been reported for BCCs (17, 18). Sex-specific differences were recently observed with respect to lesion localization, i.e. in patients affected by KCs of the pinna. In particular, while in male patients the ratio between BCCs and SCCs was almost equal, females showed a 4-fold higher frequency of BCCs of the pinna compared with males (19).
Mortality rates for individuals with KC have been reported to be higher in men than in women (15), except for genital localization, where mortality rates were higher in white women (20).
Sex differences in QoL or health status of patients with skin diseases have been analysed and observed in many studies (21, 22) with women generally reporting greater impairment in QoL and more psychological symptoms than men. To our knowledge, very few studies have investigated QoL in patients with KCs separately for men and women (12, 23, 24). Such data may be important for tailored management of the disease in different categories of patients.
The aim of this study was to analyse sex-specific differences in health-related QoL (HRQoL) of KC patients recruited in a dermatological outpatient clinic in Italy with regards to demographic and clinical variables.
Study population
Patients with a diagnosis of KC were recruited at the day surgery unit of an Italian dermatological reference centre. Inclusion criteria were: (i) written informed consent; (ii) age >18 years; (iii) clinical diagnosis of KC (BCC or SCC); (iv) ability to understand Italian and to complete the questionnaires. The study was approved by the Institutional Ethical Committee.
Collected data
For each patient, demographic and clinical data were collected. For the purpose of this study, the following variables were used: sex, age (< 60, 60–74, ≥ 75 years), education (junior high school, high school, university), phototype, smoking status, localization of the lesion (head/neck, trunk, arms/legs), previous KC, diameter of tumour at resection (< 0.5, 0.5–1.5 mm, > 1.5 mm), disease onset (0–3 and ≥ 4 months), number of comorbidities (hypertension, diabetes, heart disease, thyroid disease, chronic obstructive pulmonary disease, other). KC was classified as either low or high risk, according to the National Comprehensive Cancer Network Guidelines for BCC and SCC (25, 26). The clinical risk factors considered for this classification of KCs are: location/size, borders, primary vs recurrent, immunosuppression, site of prior radiotherapy or chronic inflammatory process, rapidly growing tumour, and neurological symptoms. Histopathological risk factors for “high risk” are: subtype, degree of differentiation, thickness or level of invasion, and perineural, lymphatic, or vascular involvement. Severity was also evaluated by the patients using the Patient’s Global Assessment (PtGA) based on a 5-point scale: very mild, mild, moderate, severe, and very severe.
Outcome measures
Generic HRQoL was measured using the self-administered 12-item Short Form Health Survey (SF-12) (27, 28). SF-12 consists of 12 questions with responses that are either dichotomous (yes/no), or ordinal (excellent to poor), or expressed by a frequency (always to never). Scores from the different answers are summarized into 2 scales: Physical Component Summary (PCS) and, Mental Component Summary (MCS). The higher the score, the better the health status.
The Skindex-29 (29) was used to evaluate skin-related QoL on 3 scales: symptoms, emotions and functioning. Answers are given on a 5-point scale (0: never; 1: rarely; 2: sometimes; 3: often; 4: always), with higher scores indicating a higher effect of skin disease on QoL.
The 12-item General Health Questionnaire (GHQ-12) (30) is a self-administered questionnaire, which allows patients to be defined as having possible non-psychotic, minor psychiatric disorders (i.e. GHQ cases). For this purpose, scores given on a 4-point scale were computed by collapsing adjacent responses to obtain a dichotomous scoring (0-0-1-1). The scores of each question were added together in order to obtain a total score (possible range: 0–12). Patients scoring 4 or more were operationally defined as GHQ-12 cases (31).
Data were summarized as mean values for SF-12 PCS and MCS scale scores, and for the Skindex-29, and as percentage of cases for the GHQ-12. Both SF-12 scales and GHQ-12 scores were compared between men and women in different levels of demographic and clinical variables. For each level, mean values were compared using Student’s t-test and analysis of variance (ANOVA), and percentages using the χ2 test. Skindex-29 scale scores and single items were compared between men and women using Student’s t-test. Skindex-29 scores were transformed into a 0–100 scale.
In order to test the possible determinants of health status, and in particular to test the association with sex, PCS and MSC were used in multivariable linear regression models as dependent variables. Variables significantly associated with PCS or MCS in univariate analyses were included in the models as independent variables. For PCS those variables were: sex (0 = female, 1 = male), age (continuous), educational level (0 = junior high school, 1 = high school, 2 = university), smoking (0 = no, 1 = yes), number of comorbidities (continuous), and disease onset (0 = 0–3 months, 1 = ≥ 4 months). For MCS independent variables were: sex (0 = female, 1 = male), age (continuous), disease onset (0 = 0–3 months, 1 = ≥ 4 months), PtGA (continuous), GHQ-12 (0 = non case, 1 = case).
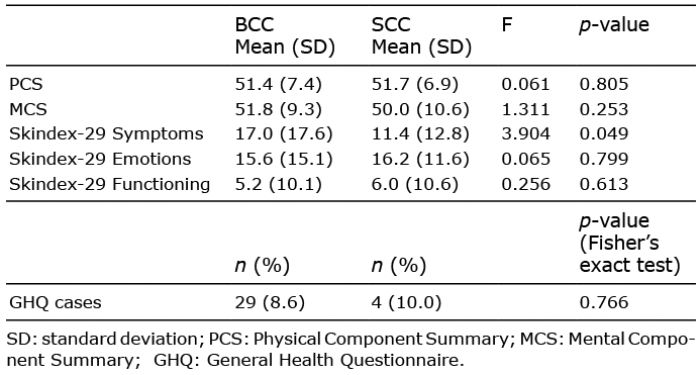
Out of 389 recruited patients, 364 completed the SF-12, 375 the Skindex-29, and 379 the GHQ-12 questionnaires. Of these, 59.9% were men, and the mean (standard deviation; SD) age was 65.9 (13.4) years. Mean scores of all QoL measures (i.e. SF-12, Skindex-29 and GHQ-12) were not significantly different between patients with SCC and BCC (Table I) Due to this lack of distinctive features, in addition to the relatively small number of patients with SCC (n = 43), BCC and SCC were grouped together. Table II describes the demographic and clinical characteristics of the 364 patients for whom data on all the questionnaires were complete. The same table reports the mean scores of the PCS and MCS scales of the SF-12 and the percentage of GHQ cases according to the different variables, separately for men and women. Concerning the physical component (i.e. PCS), women reported a lower QoL compared with men in the following subgroups: age from 60 to 74 years, no smokers, and with previous KC. For the mental component of the SF-12 (i.e. MCS), with a few exceptions, women had significantly lower scores compared with men. The percentage of GHQ cases was higher in women than in men in the subgroups of high educational level, phototype 3–4, localization of the lesion on head/neck, and high disease severity. Skindex-29 mean score was higher in women than in men for the emotions scale (Table III). Among the Skindex-29 single items, women, compared with men, reported significantly higher worry that the disease could get worse and of developing scars, and more depression. On the other hand, men reported lower quality of sleep. The items most often reported by both men and women were worry that the disease might be serious and worsen, and, among symptoms, itch. The results of the multivariable linear regression model with PCS as the dependent variable are shown in Table IV. Sex was significantly associated with the physical component, with a lower QoL in women compared with men. Other significant variables were: age (QoL decreasing with increasing age), smoking (worse QoL in smokers), number of comorbidities (worse QoL for more comorbidities), and disease onset (better QoL for less recent onset). In a separate multivariable linear regression model, sex was also significantly associated with the MCS (Table V) with a lower QoL in women. The association of age and disease onset with MCS was similar to that observed for the PCS. In addition, a worse mental score was associated with higher disease severity according to the PtGA, and in GHQ cases.
Table I. Comparison of quality of life instruments’ scores in patients with basal cell carcinoma (BCC) and squamous cell carcinoma (SCC)
Table II. Mean 12-item Short Form Health Survey (SF-12) Physical Component Summary (PCS) and Mental Component Summary (MCS) scores and percentage of 12-item General Health Questionnaire (GHQ-12) cases according to demographic and clinical variables in males and females with keratinocyte carcinomas
Table III. Mean values of the Skindex-29 scales scores and their single items in men and women
Table IV. Results of the multivariable linear regression model with Physical Component Summary (PCS) of the 12-item Short Form Health Survey (SF-12) as dependent variable
Table V. Results of the multivariable linear regression model with Mental Component Summary (MCS) of the 12-item Short Form Health Survey as dependent variable
In this study, women with KC reported a lower HRQoL than men, both in the physical and the mental component. In other dermatological conditions, when a sex difference in QoL was observed, it was generally related to a higher impairment in female patients. For example, this was reported in studies on patients with psoriasis (22), acne (32), and alopecia (33). QoL is an important outcome in the evaluation of a condition, of its changes over time, and thus of the effectiveness of a treatment. In particular, such indicator is essential when a disease is not life-threatening. This is the case in KCs, and in particular in BCC, in which mortality rate has been found as not statistically significantly different than controls (34), and even lower than the general population (35). However, KC may affect appearance, when it develops in visible body areas, and patients may have symptoms, such as pain and bleeding. Moreover, patients may experience aesthetic consequences of surgery, functional impairment, and anxiety regarding cancer recurrence. More than the comparison with the general population and other skin conditions, it may be interesting to analyse QoL in subgroups of patients with KCs. In particular, the aim of the present study was to investigate sex differences, as only a few studies are available on this subject. Abedini et al. (23) did not find any significant difference in mean Dermatology Life Quality Index (DLQI) scores for men and women. However, some dimensions of the questionnaire, such as personal relationships, work and school, and treatment were more severely impaired among men. In another study (12), in which the EQ-5D-5L Index was used, men reported a worse QoL than women. This difference was not observed using the other component of the instrument, i.e. the EQ VAS. On the other hand, the study from Harlow et al. (24) reported a higher DLQI (i.e. higher impact) in women than in men, in particular for embarrassment, self-consciousness, and influence of skin disease on choice of clothes. Results are thus discordant, probably due to the different instruments used. In the current study, we chose to use a generic QoL instrument (the SF-12), a dermatology-specific one (the Skindex-29) and an instrument concerning psychological aspects (the GHQ-12), to evaluate QoL in men and women with KCs. The 3 instruments were concordant in pointing out a higher emotional and psychological impact of KC in women than in men. For MCS, this was observed in almost all the subgroups of patients according to demographic and clinical variables. In addition, this difference was significantly higher in the items of the Skindex-29 concerning worry and depression. These results are in the same line as previous studies, in which it appeared that men and women were generally sensitive to different aspects of QoL. In fact, men are generally more impaired in social life and work (23), and women in emotions, such as embarrassment and self-consciousness (24).
Overall, in the current study, the items of the Skindex-29 with the highest mean values concerned worry. Women were particularly concerned with seriousness and worsening of the condition and with having scars. In line with the present study, worry and appearance of the condition were the problems most often reported in a previous study on patients with skin cancer where the Skindex-16 was used (36). Even though KCs are generally considered as not serious conditions, it is possible that patients experience cancer-related worry, especially immediately after the diagnosis.
The SF-12 also evidenced a higher physical impact of KC in women than in men, even after adjusting on the number of comorbidities in the multivariable model. Generic and dermatology-specific questionnaires have been used also in previous studies on patients with KC. In a study on non-melanoma cervicofacial skin cancer (37), the authors used the SF-36; however, they did not perform a specific analysis on sex. The SF-12 was used in a study on the evaluation of patients’ satisfaction after treatment for NMSC (38). In various studies, dermatology- specific questionnaires have been employed, such as different versions of the Skindex (11, 36, 39, 40), or the DLQI (8, 41). However, most of these studies evaluated changes in QoL after treatment and did not focus on sex differences.
The use of a generic health status instrument, such as the SF-36 or -12, or the EQ-5D, has the limitation of not evaluating specific aspects due to the skin condition. However, it has the advantage of allowing comparisons with other conditions, also non-dermatological, and with the general population. In order to minimize the effect of other medical conditions and of age, which are the main determinant of health status, those variables were taken into account in the analyses, and the difference between men and women in QoL impact was confirmed. The Skindex-29, which is specific for skin conditions, confirmed the stronger emotional impact of KC on QoL in women than in men, and, by the analysis of its items, allowed to shed further light on specific aspects. A limitation of the study is that cancer-specific and skin-cancer specific QoL questionnaires were not used. However, in a recent position paper on QoL measurement in skin cancer patients, the authors also recommended the use of dermatology-specific questionnaires in order to specifically assess skin-related problems (42).
The sex differences in impact on QoL observed in patients with KCs should be taken into consideration by clinicians in the management and treatment of these conditions. In particular, worry about the disease, which we found to be significantly increased among women, should be addressed to avoid unnecessary anxiety, and to increase awareness of the need for adherence to photoprotection and to attend regular follow-up visits for early detection of new or recurrent KCs.
This work was supported, in part, by “Progetto Ricerca Corrente” of the Italian Ministry of Health, Rome, Italy.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize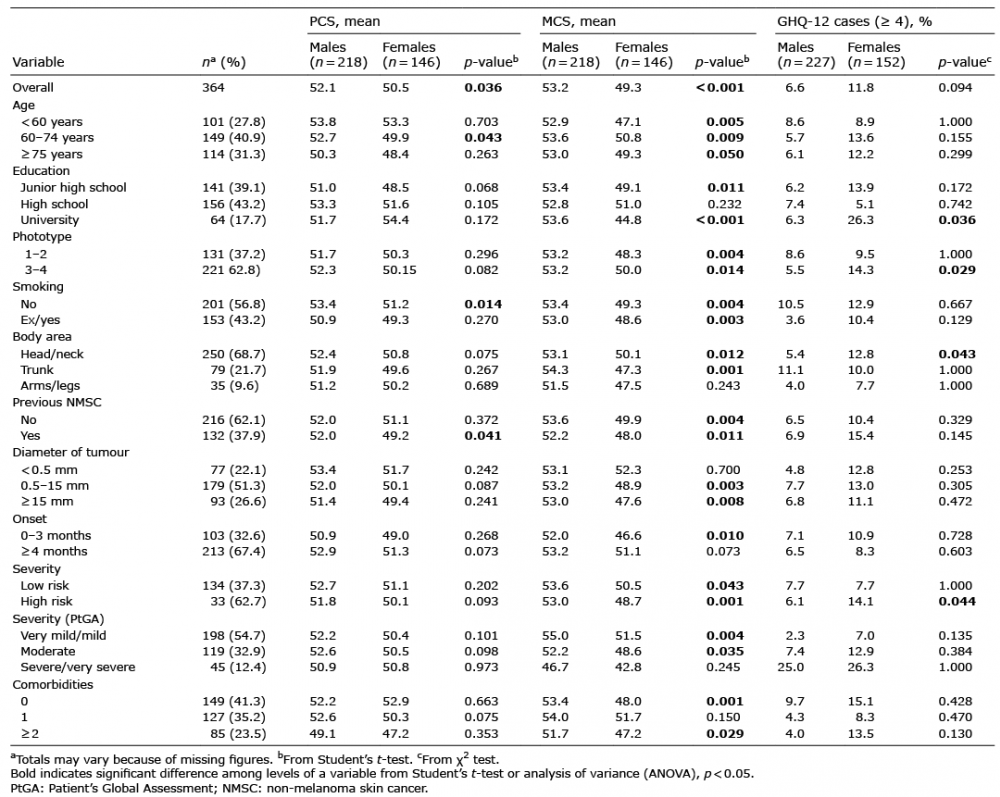 Click to show fullsize
Click to show fullsize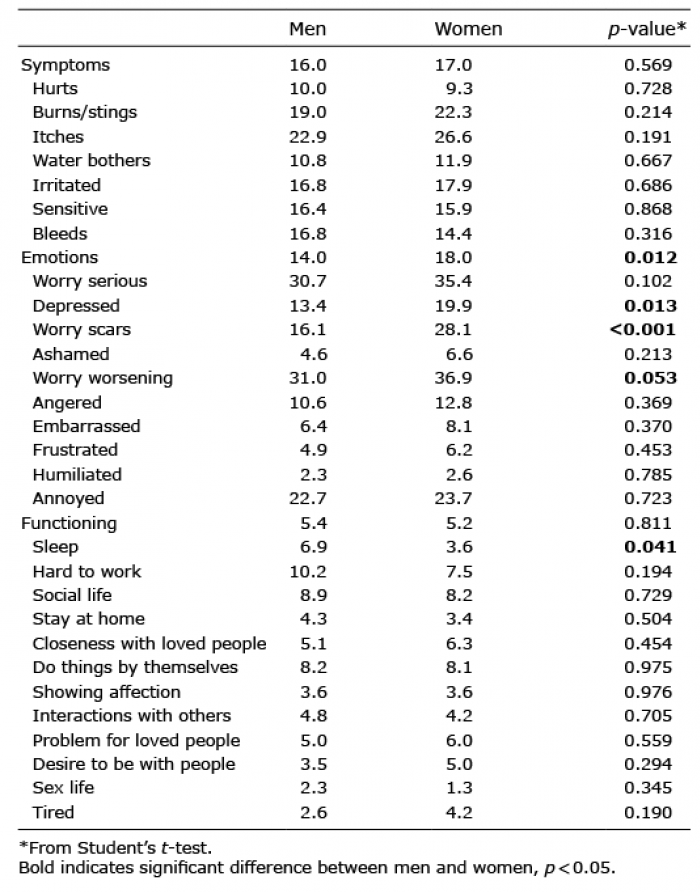 Click to show fullsize
Click to show fullsize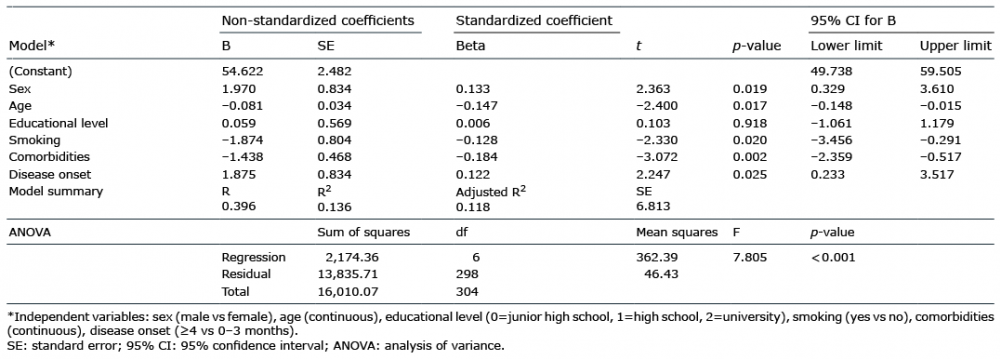 Click to show fullsize
Click to show fullsize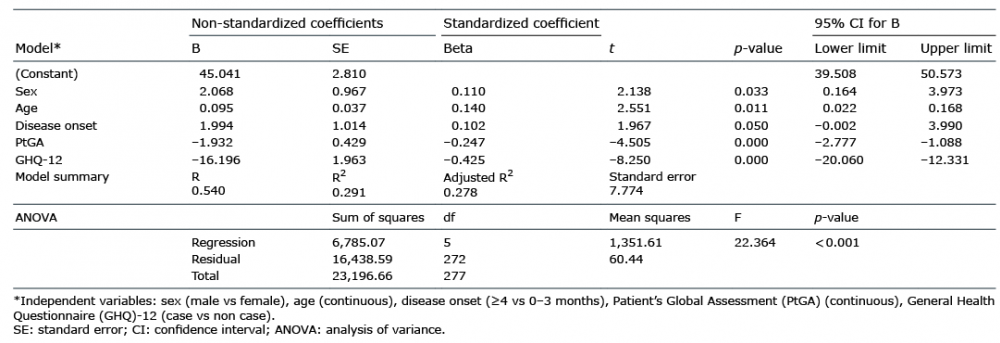 Click to show fullsize
Click to show fullsize