


1Department of Dermatology and Vener?ology and 2Department of Clinical Pathology, Acibadem City Clinic Tokuda Hospital, 51B Nikola Vaptsarov Boulevard, BU-1407 Sofia and 3Section of Dermatovenereology, Trakia University, Stara Zagora, Bulgaria. *E-mail: darlenski@abv.bg
A 54-year-old female Caucasian patient presented with a history of recurrent asymptomatic eruption on her trunk and extremities. She reported concomitant severe asymmetrical ankle pain and swelling, and a fever of up to 39.5°C during episodes. She had no further history of present or previous skin or systemic diseases.
Clinical examination revealed sharply demarcated gyrate erythematous bands, forming a wood-grain appearance, localized on her trunk and the lower extremities (Fig. 1). Histopathological examination of a skin biopsy is depicted in Fig. 2. Laboratory studies were performed, including: complete blood count, blood biochemistry, serological tests (anti-T. pallidum, viral hepatitis, anti-Echinococcus, anti- B. burgdorferi, anti-H. pylori, anti-Coxiella burnetii), microbiological examination of throat swab, blood, urine and faeces, antinuclear antibody, rheumatoid factor, computed tomography (CT) scan of the chest, abdomen and pelvis with contrast, full-body magnetic resonance imaging (MRI), fibrogastroscopy and colonoscopy. All tests were within normal ranges, except for increased IgG antibodies for C. burnetii and elevated erythrocyte sedimentation rate (ESR).
Based on the patient’s clinical history and the laboratory findings, a diagnosis of chronic Q fever was made. Therapy with doxycycline (200 mg/daily) for 14 days and methylprednisolone (40 mg/daily) led to temporary resolution of the rash and fever. Control serology tests for C. burnetii were negative. The skin rash and arthritis relapsed, Methylprednisolone (24 mg daily, with a weekly reduction in the dose) was continued for 45 days. This resulted in complete clearance of the skin lesions and considerable relief of the joint pain. Follow-up after 6 months found no recurrence of the skin symptoms, although mild arthritis symptoms were still present and were controlled by non-steroid anti-inflammatory agents.
What is your diagnosis? See next page for answer.
Fig. 1. Concentric erythematous rings resembling a wood-grain appearance on the patient’s trunk.
Fig. 2. Histopathology (haematoxylin and eosin stain) of a skin lesion biopsy revealed hyperkeratosis, atrophic epidermal layer (a; magnification ×10), oedema in the dermis, dilated vessels and perivascular lymphocytic infiltrate (b; magnification ×40).
Acta Derm Venereol 2021; 101: adv00380.
Diagnosis: Eythema gyratum repens associated with no malignancy but with chronic Q fever
Erythema gyratum repens (EGR), generally perceived as paraneoplastic dermatosis, is a rare reactive clinical pattern of figurate skin erythema (1). In more than 80% of cases, EGR is associated with an underlying malignancy, and in 80% of cases the eruption appears prior to the neoplastic disease (2). EGR has been described in association with non-neoplastic diseases, such as tuberculosis, drug use (azathioprine and pegylated interferon alpha), hypereosinophilic syndrome, and autoimmune conditions (rheumatoid arthritis and CREST syndrome (calcinosis, Raynaud’s phenomenon, oesophageal dysmotility, sclerodactyly and telangiectasia)) (3).
There are 3 hypotheses regarding the pathogenesis of EGR: (i) cross-reacting tumour antigens that cause an inflammatory skin response; (ii) transformation of normal skin proteins by tumour, thus making them antigenic; (iii) deposition of immune complexes with tumour antigens at the basement membrane zone (BMZ) and induction of inflammation (2, 3).
Arthritis is a rare symptom of chronic Q fever, despite the fact that infection with C. burnetti can trigger an intense immune response and the formation of immune complexes as an integral part of the pathogenesis (4). In the current case, we consider that EGR and the associated arthritis are reactive conditions, due to concomitant infection with C. burnetii Q fever in the chronic phase.
As far as we are aware, this is the first reported association of EGR and Q fever. Successful treatment of the infection resulted in resolution of the reactive skin symptoms.


 Click to show fullsize
Click to show fullsize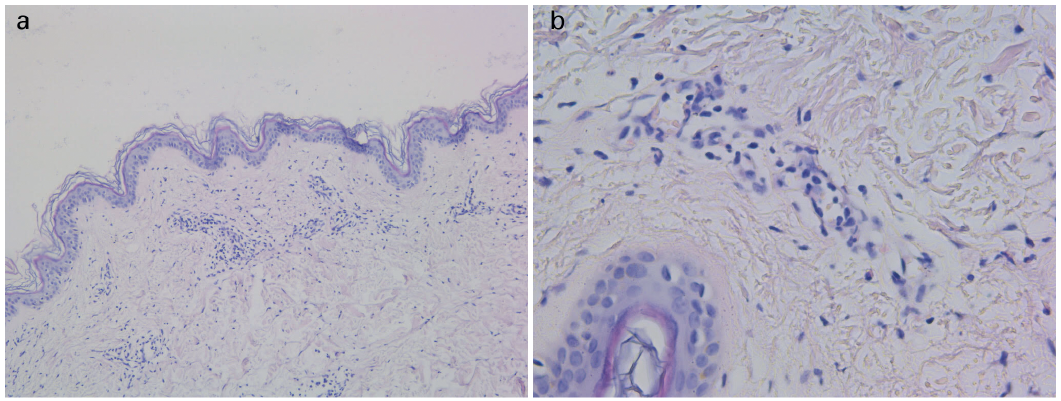 Click to show fullsize
Click to show fullsize