


1Department of Dermatology, 2Lübeck Institute of Experimental Dermatology and 3Institute for Cardiogenetics, University of Lübeck, Lübeck, Germany
In pemphigoid diseases, direct immunofluorescence can be used to differentiate 2 patterns of antibody deposition at the dermal–epidermal junction; u- and n-serrated pattern. The u-serrated pattern is found in epidermolysis bullosa acquisita, and n-serrated pattern in all other pemphigoid diseases. To determine the detection frequency of these serrated patterns and the optimal thickness of biopsy cryosections, 2 patient cohorts obtained form our routine autoimmune laboratory were analysed; a retrospective cohort (n = 226) and a prospective cohort (n = 156). In 76% (291/382) of biopsies, a pattern was recognized, of which 96% (278/291) and 4% (13/291) had an n- or u-serrated pattern, respectively. A u-serrated pattern was seen in all epidermolysis bullosa acquisita biopsies confirmed by serology. No antibodies against type VII collagen were detected in any of the sera from biopsies with n-serrated pattern. No differences between the detection frequencies of serrated pattern were seen with respect to age, sex, biopsy site, or section thickness, while the detection frequency was higher in patients with serum anti-BP180 reactivity compared with those without. In conclusion, serrated pattern analysis using direct immunofluorescence has a high detection frequency and specificity for epidermolysis bullosa acquisita and will further facilitate the diagnosis of latter disorder.
Key words: serration pattern analysis; direct immunofluorescence microscopy; pemphigoid disease; autoantibody.
Accepted Jan 21, 2021; Epub ahead of print Jan 25, 2021
Acta Derm Venereol 2021; 101: adv00410.
doi: 10.2340/00015555-3748
Corr: Enno Schmidt, Department of Dermatology, University of Lübeck, Ratzeburger Allee 160, DE-23538, Lübeck, Germany. E-mail: enno.schmidt@uksh.de
Pemphigoid diseases are blistering skin diseases. To diagnose these diseases, antibody depositions at the dermal–epidermal junction can be detected in perilesional skin biopsies. To differentiate between different pemphigoid diseases, 2 patterns of antibody deposition can be found at high magnification, namely u- and n-serrated pattern. The u-serrated pattern is found in epidermolysis bullosa acquisita, and the n-serrated pattern is observed in all other pemphigoid diseases. This study analysed 382 biopsies in order to determine the detection frequency of these serrated patterns. In 76% (291/382) of biopsies, a pattern was recognized, of which 96% (278/291) and 4% (13/291) had an n- or u-serrated pattern, respectively.
Pemphigoid diseases are characterized by circulating and tissue-bound autoantibodies against structural proteins of the dermal–epidermal junction (DEJ). Pemphigoid subtypes include bullous pemphigoid, mucous membrane pemphigoid, anti-p200 pemphigoid, linear IgA dermatosis, pemphigoid gestationis, and epidermolysis bullosa acquisita (EBA) (1). Diagnosis is based on direct immunofluorescence microscopy (DIF) of perilesional biopsies, in which linear deposits of IgG, and/or IgA, and/or C3 at the DEJ can be observed (2, 3). Clinical appearance and DIF enable the diagnosis of mucous membrane pemphigoid (with predominantly mucosal lesions) and linear IgA dermatosis (with predominantly IgA deposition at the DEJ) (2, 3). In contrast, inflammatory EBA cannot be differentiated from bullous pemphigoid and anti-p200 pemphigoid based on clinical appearance and DIF alone (4–7). This is of both prognostic and therapeutic relevance, since patients with EBA have a more protracted course and require more intensive treatment compared with patients with bullous pemphigoid and anti-p200 pemphigoid (4–8).
In 2004, the concept of serration pattern analysis was proposed, based on the observation that, in pemphigoid disorders, the linear deposits of immunoreactants at the DEJ frequently appear slightly undulated at high resolution on DIF (9). Two patterns of antibody deposition along the DEJ were differentiated; n-serrated pattern and u-serrated pattern. The u-serrated pattern is characterized by arches that are open at the top, resembling “growing grass” (Fig. 1A). The u-serrated pattern is seen only with deposition of type VII collagen-specific immunoreactants of the sublamina densa zone between the rootlets of the basal keratinocytes found in patients with EBA and bullous systemic lupus erythematosus (9). In all other pemphigoid diseases, the n-serrated pattern can be seen, characterized by arches that are closed at the top and immunodeposits above the lamina densa that follow the distribution pattern of hemidesmosomes of basal cell rootlets (Fig. 1B) (9).
Fig. 1. Serration patterns by direct immunofluorescence microscopy (DIF) of perilesional skin biopsies in pemphigoid diseases. (A) The u-serrated pattern characterized by arches that are open at the top resembling “growing grass”. This serration pattern is exclusively detected in autoimmunity against type VII collagen, i.e. in epidermolysis bullosa acquisita and bullous systemic lupus erythematosus. (B) The n-serrated pattern characterized by arches that are closed at the top. This serration pattern is seen in all other pemphigoid diseases. (C) In approximately one-quarter of biopsies, no specific serration pattern can be detected.
Serration pattern analysis is particularly helpful in EBA, since serum autoantibodies are detected in only approximately half of patients with EBA (4–6). The use of immune electron microscopy represents another useful diagnostic approach; however, it is used in only a handful of centres, as it is very costly and time-consuming and is restricted to fresh biopsies (5, 10).
The aims of the present study were to determine the percentage of perilesional biopsies that allow the identification of a specific serration pattern by DIF, and the optimal thickness of sections, based on studying 2 large cohorts of consecutive patients with different pemphigoid subtypes.
Retrospective patient cohort
Reports of 226 perilesional skin biopsies from our routine autoimmune laboratory (Department of Dermatology, University of Lübeck, Lübeck, Germany), which showed linear deposits of IgG, IgA, and/or C3 at the DEJ on DIF were retrospectively analysed for statements about the serration pattern. The cohort included 115 women and 111 men, with a mean age ± standard deviation (SD) of 73 ± 17 years (range 1–102 years). The samples had been analysed in the period from January 2014 to June 2016; each sample was analysed by 1 of 6 physicians, all of whom were trained in reading immunofluorescence slides and serration pattern analysis (11). Routine reading was performed using DIF slides of 6 µm thickness. Readings were reported as “u-serrated” (Fig. 1A), “n-serrated” (Fig. 1B), “undetermined” (neither n- nor u-serrated pattern was detected) (Fig. 1C), or “without pattern specification” (no information about serrated pattern was noted by the initial reader). All “undetermined” biopsies were then cut into 4-µm sections and re-examined using DIF. All biopsies “without pattern specification” were cut into 6-µm sections and re-examined using DIF. Biopsies that did not allow pattern recognition were cut into 4-µm sections and re-examined using DIF.
Prospective patient cohort
Between 1 July 2016 and 30 June 2017 the serration pattern was prospectively determined using DIF for all biopsies taken in our routine autoimmune laboratory that had linear deposits of IgG, IgA, and/or C3 at the DEJ (n = 156). The cohort included 83 women and 73 men, with a mean age ± SD of 75 ± 14 years (range 3–97 years). All sections were routinely cut into 4-µm sections.
In both the retrospective and prospective cohorts, biopsies from mucous membranes were excluded, as it was reported that the serration pattern is not present in these biopsies (9). Biopsy sites included the head, upper limb, lower limb, back and buttocks. In addition to immunofluorescence analysis of skin biopsies, available patient sera from both cohorts (n = 309) were subjected to the following routine diagnostic assays (12–15): indirect immunofluorescence (IIF) on salt-split human skin (for IgG and IgA reactivity), BP180-, BP230- and type VII collagen-specific enzyme-linked immunoassays (ELISAs) (Euroimmun, Lübeck, Germany), immunoblotting with extract of human dermis (for reactivity against p200 and type VII collagen), recombinant C-terminus of laminin γ1, and extracellular matrix of cultured human keratinocytes (for reactivity against laminin 332).
The study was performed according to the Declaration of Helsinki and approved by the ethics committee of the University of Lübeck (12-178).
Statistical analysis
Associations of serration patterns with serological and epidemiological characteristics and different thicknesses of sections were analysed using χ2 test.
Retrospective cohort
All biopsies collected between 2014 and 2016 with no serration pattern specification (n = 59) or an undetermined pattern (n = 24) were re-cut and re-evaluated for their serration pattern. In 8 of 59 biopsies, a pattern was recognized (all n-serrated) when re-examining the biopsies in 6-µm-thick sections. In 17 of the 75 remaining biopsies with undetermined pattern initially analysed using 6-µm-thick sections, a pattern was observed (all n-serrated) using thinner sections of 4 µm. Altogether, in 168 out of 226 (74.3%) biopsies, a pattern was recognized, comprising 159 (94.6%) with n-serrated pattern and 9 (5.4%) with u-serrated pattern (Fig. 2). The frequency of pattern detection was 74.3% and 66.8% in 4-µm and 6-µm sections, respectively. No significant difference was observed between the different section thicknesses (p = 1.0), although analysis of the thinner (4-µm) sections led to detection of the n-serrated pattern in 17 additional patients.
Fig. 2. Detection frequencies of serration pattern diagnosis by direct immunofluorescence microscopy (DIF) of perilesional skin biopsies in pemphigoid diseases.
Prospective cohort
A total of 123 out of 156 (78.8%) biopsies showed a serration pattern, of which 119 (96.7%) and 4 (3.3%) biopsies were either n- or u-serrated, respectively (Fig. 2).
Serum samples were available for 309 of 382 patients from the retrospective and prospective cohorts. By combining DIF results with the clinical picture and serology, patients were classified into different subgroups: bullous pemphigoid (n = 226); pemphigoid without serum antibodies (n = 33); anti-p200 pemphigoid (n = 15); pemphigoid with unidentified target antigen (but positive by IIF) (n = 16); linear IgA dermatosis (n = 10); mucous membrane pemphigoid or pemphigoid gestationis (n = 5); and EBA (n = 4). The pattern detection frequencies in these subgroups were: 81% (182 of 226) for bullous pemphigoid; 82% (27 of 33) for pemphigoid without serum antibodies; 67% (10 of 15) for anti-p200 pemphigoid; 50% (8 of 16) for pemphigoid with unidentified target antigen; 80% (8 of 10) for linear IgA dermatosis; 100% (4 of 4, all with u-serrated pattern) for EBA; and 60% (3 of 5) for mucous membrane pemphigoid or pemphigoid gestationis (Table I).
Table I. Pattern detection frequencies by direct immunofluorescence (DIF) in different pemphigoid diseases
When analysing the 9 retrospective and 4 prospective patients with the u-serrated pattern in detail, antibodies against type VII collagen were detected in 4 patients, 7 patients were unreactive with type VII collagen and other target antigens of the DEJ (in specific assays as well as IIF on human salt-split skin), and no serum was available for 2 patients. Regarding DIF, 11/13 patients with u-serrated pattern were specific for IgG, and 2/13 for IgA. Notably, no circulating antibodies against type VII collagen were detected by ELISA and immunoblotting in the pemphigoid patients with undetermined serration pattern and available serum (n = 67).
No significant association was observed between the detection frequency of the serration pattern, irrespective of the observed pattern, and the patients’ age (p = 0.7), biopsy site (p = 0.7), and section thickness (4 vs 6 µm; p = 1.0). The detection frequency for an n-serrated pattern was significantly higher in patients with serum anti-BP180 antibodies compared with patients without anti-BP180 reactivity (p = 0.012, 81.2% vs 67.5%). A serration pattern was recognized in 234/295 (79%) biopsies stained with anti-human-IgG, 13/19 (68%) with anti-human-IgA, and 44/68 (65%) with anti-human-complement C3 antibody.
Pemphigoid diseases are a heterogeneous group of disorders with respect to prognosis and treatment approach (1–3). The development of widely available, standardized, as well as sensitive and specific, assays for the detection of serum autoantibodies, i.e. ELISA and IIF-based tests, which apply recombinant forms of the target antigens, have enabled serological diagnosis of most pemphigoid diseases, if the clinical picture is known (2, 4–7, 11, 13, 15–18). Although standardized assays using recombinant or cell-derived forms of type VII collagen are widely available, diagnosis of EBA remains challenging, and autoantibodies can be detected in only approximately 50% of patients (5, 14, 16, 19–21). To diagnose EBA in patients without serum autoantibodies direct immune electron microcopy has been used (5, 10). However, this method has limited application in routine diagnosis due to its high costs and time expenditure (5).
Following the description of serration pattern diagnosis in Groningen, the Netherlands, in 2004 (9), the Groningen team created an online tool that provides training for serration pattern analysis in DIF samples (11). The same group showed that the u-serrated pattern occurs only in EBA and bullous systemic lupus erythematosus, and is not found in other pemphigoid diseases, such as anti-p200 pemphigoid and anti-laminin 332 mucous membrane pemphigoid (22, 23). A recent study found that routine serration pattern analysis can be established in other autoimmune laboratories with high reliability and is independent of transport medium (isotonic saline solution or Michel’s medium), mounting and cutting techniques, section thickness, and the level of experience of the investigators (24). Limitations of this last study were the relatively small sample size (20 biopsies) and its retrospective approach (24).
The aim of the current study was to determine the proportion of pemphigoid patients in whom a specific serration pattern could be identified using DIF. All pemphigoid patients identified by linear deposition of IgG, IgA, and/or C3 at the DEJ in our routine autoimmune laboratory during a specific time-period were included in the study. In both the retrospective and prospective cohorts, a serration pattern could be identified in approximately 3 out of 4 biopsies. This is comparable with the detection frequency in 3 different groups of observers who were trained in serration pattern diagnosis via an online tool with 26 DIF images: dermatology residents in training at the University Medical Center Groningen; international experts on bullous diseases; and dermatologists and pathologists who had participated in the Groningen blistering course during the past 10 years (11). However, the detection frequency was considerably lower than the 97.5% and 100% found in previous studies of 10 and 20 preselected biopsies (23, 24). In the current study, serration pattern recognition was not limited to staining of anti-human IgG, but was also observed for IgA and complement C3. No obvious differences were found in the detection frequencies of a specific serration pattern and a distinct pemphigoid disease, although sample numbers for mucous membrane pemphigoid, linear IgA disease, and pemphigoid gestationis were low.
Importantly, in all 4 patients with EBA confirmed by the presence of serum antibodies against type VII collagen, the u-serrated pattern was recognized during initial analysis, implicating that no u-serrated pattern remained undetected. In addition, none of the 7 patients with EBA with u-serration pattern in the skin, but without detectable serum antibodies against type VII collagen, showed additional autoantibodies against other target antigens of the DEJ. Equally, none of the patients with other pemphigoid subtypes who had no specific serration pattern in the skin had circulating serum antibodies against type VII collagen.
The current study also did not find any associations between the detection frequency of a specific serration pattern and patient’s age or biopsy site. In agreement with a previous report, no differences in detection frequency were observed between biopsies of different thicknesses (i.e. 4 or 6 µm) (24). The observation that patients with serum anti-BP180 reactivity are more likely to reveal a specific serration pattern on DIF compared with patients without serum anti-BP180 antibodies may indicate that BP180 contributes more strongly to the formation of n-serrated basal membrane zone-labelling than other target antigens, such as BP230, p200 antigen, and laminin 332.
To summarize, serration pattern analysis using DIF on routine perilesional biopsies from patients with non-EBA pemphigoid had a sensitivity of 75%, and from patients with EBA the sensitivity and specificity was 100%. Detection frequencies were independent from section thickness (4 µm or 6 µm). In conclusion, these results support the use of serration pattern diagnostics using DIF on perilesional biopsies in a routine setting in order to differentiate EBA from other pemphigoid diseases.
The authors thank Inge Atefi for excellent technical assistance, Manuela Pigors for critically reading the manuscript, and Christoph M. Hammers, Franziska Hübner, Michael Kasperkiewicz, Ana L. Lima, Artem Vorobyev, and Mareike Witte for reading DIF slides in our routine laboratory.
This work was supported by grants from the Deutsche Forschungsgemeinschaft through Clinical Research Unit 303 Pemphigoid Diseases (to DZ and ES) and Excellence Cluster 2167/1 Precision Medicine in Chronic Inflammation.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize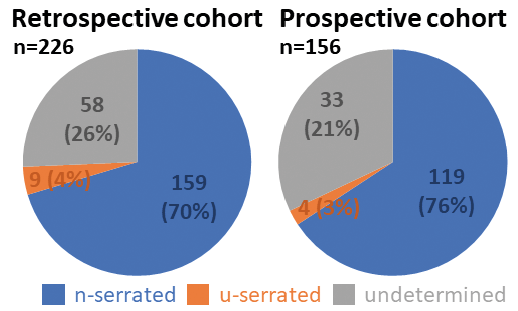 Click to show fullsize
Click to show fullsize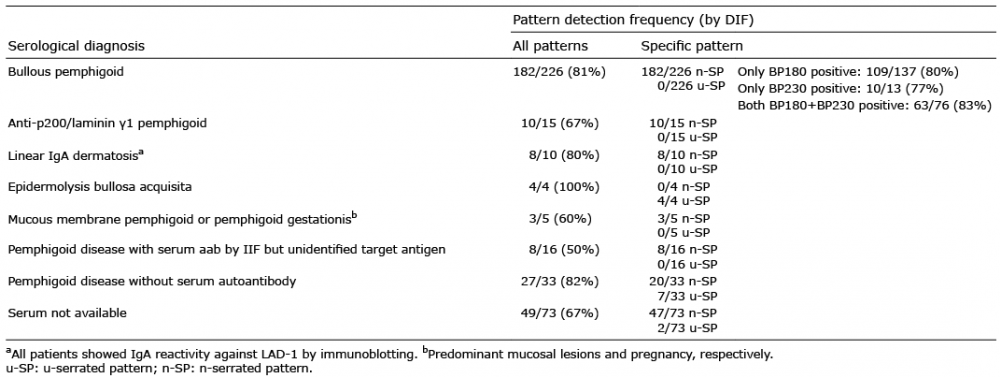 Click to show fullsize
Click to show fullsize