


1Department of Dermatology, Kyoto University Graduate School of Medicine, Kyoto, 2Department of Dermatology, Hamamatsu University School of Medicine, 1-20-1, Handayama, Higashi-ku, Hamamatsu, Shizuoka, 431-3192, 3Department of Dermatology, Kagawa University Faculty of Medicine, Kagawa, Japan and 4Singapore Immunology Network (SIgN) and Skin Research Institute of Singapore (SRIS), Agency for Science, Technology and Research (A*STAR), Singapore, Singapore. *E-mail: hontetsu@hama-med.ac.jp
Accepted Feb 16, 2021; Epub ahead of print Feb 19, 2021
Acta Derm Venereol 2021; 101: adv00411.
doi: 10.2340/00015555-3773
Autoantibodies against bullous pemphigoid (BP)180, a transmembrane glycoprotein, are a hallmark of BP and play critical roles in blister formation in patients with BP. However, marginal elevation of serum anti-BP180 antibody can occasionally be detected in other patients with inflammatory skin diseases, such as atopic dermatitis (AD) and lichen planus (1). We report here a case of AD with very high serum levels of anti-BP180 antibody and development of dyshidrosiform BP-like blisters on the palms and soles.
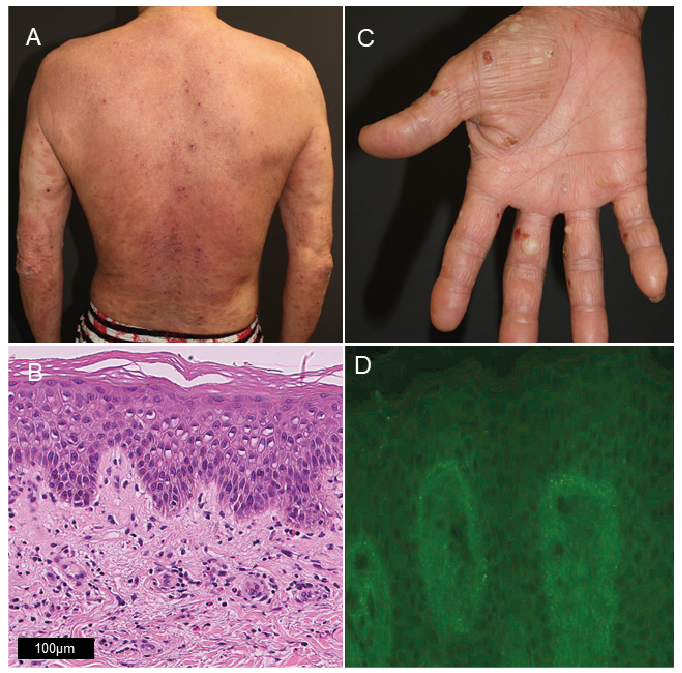
A 44-year-old man presented to our hospital with generalized pruritic eruption. He had been diagnosed with AD at approximately 17 years of age. The patient had no other atopic history including asthma, rhinoconjunctivitis, and food allergies, and no family history of atopy. He had received intermittent treatment with topical steroids at nearby clinics. The patient exhibited pruritic papules and erythema with lichenification on the trunk and extremities (Fig. 1A). Laboratory tests revealed mild eosinophilia (4,000/ml; normal 30–500/ml), and elevated lactate dehydrogenase (484 U/l; normal 124–226 U/l), thymus and activation-regulated chemokine (222,000 pg/ml; normal < 450 pg/ml), and IgE (16,000 pg/ml; normal 0–99 pg/ml). Histological examination of the papules from the left arm revealed spongiosis of the epidermis and infiltration of eosinophils and lymphocytes at the borders of epidermis and dermis and around blood vessels (Fig. 1B). The patient was diagnosed with severe AD (Eczema Area and Severity Index: 48), and was started on topical steroid therapy (clobetasol propionate ointment). Three weeks later, blisters appeared on the patient’s palms and soles, with no triggers, such as concomitant medication and physical stress on the palms and soles (Fig. 1C). An increase in serum anti-BP180 antibody titre (> 1,000 U/ml; normal < 9 U/ml) was observed (Chemiluminescent Enzyme Immunoassay, MBL MEBLux, Nagoya, Japan). However, direct immunofluorescence (DIF) of the biopsy sample from a red papule on the left upper arm showed no deposition of IgG or IgE, despite faint granular deposition of C3, in the basement membrane zone (Fig. 1D). Treatment with oral prednisolone (15 mg/day) was added for one week, which controlled the blisters well. Oral prednisolone was tapered off over 2 weeks. Serum anti-BP180 antibody levels also decreased after the therapy (318 U/ml at one month later, and 47 U/ml at 6 months later). The erythema and papules repeated the remissions and exacerbation; however, neither blisters nor elevation of serum anti-BP180 antibody recurred.
Fig. 1. Clinical and histopathological findings. (A) Erythema and papules on the trunk and extremities. (B) Haematoxylin and eosin-stained section of papules on the right forearm. Spongiosis in epidermis with infiltration of eosinophils at the dermo–epidermal border. (C) Pompholyx-like blisters on the right palm. (D) Direct immuno?uorescence (DIF), showing granular C3 deposition in the basement membrane zone. Original magnification: x20.
Another case with coincidence of AD and BP has been reported (2). Because of extremely high serum levels of anti-BP180 antibody with blisters on the palms and soles in the current case, we considered the possibility of AD concurrent with dyshidrosiform BP, a rare variant of localized BP characterized by persistent and recurrent vesicular or bullous eruption localized on the soles and/or palms (3). However, the blister formation was transient and the DIF showed only granular deposition of C3 at the basement membrane, which is an atypical staining pattern of BP and can be seen non-specifically in other skin diseases (4). Based on these findings, the anti-BP180 antibody in this patient was considered non-pathogenic, and a diagnosis of AD with dyshidrosiform blisters limited to the palms and soles with high serum levels of non-pathogenic anti-BP180 antibody was made. It is not clear why anti-BP180 antibody was produced in this patient, but destruction of basement membrane zone due to severe inflammation in epidermis may have led to the production of anti-BP180 antibodies.
Although no deposition of IgG or IgE was observed in the basement membrane zone, it is possible that the anti-BP180 antibody in this patient has a pathogenic role. Further research, such as co-incubation of affinity-purified anti-BP180 antibodies from the patient with keratinocytes, and subsequent examination of the internalization of BP180, would be useful to examine the pathogenicity of the antibody.
To the best of our knowledge, this is the first case of a patient with AD with dyshidrosiform blisters limited to the palms and soles together with high serum levels of anti-BP180 antibody. It would be of interest to study the prevalence of anti-BP 180 antibody presence in patients with AD, especially in those with pompholyx. The current case suggests that high levels of serum anti-BP180 antibody can be observed in AD with vesicle or blister formation. In such cases, histological analysis using DIF can be useful for diagnosis and treatment planning.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize