


Department of Dermatology, Aarhus University Hospital, Aarhus, Denmark
Pyoderma gangrenosum is an uncommon ulcerative neutrophilic dermatosis. Clinical presentation, location and associated diseases are diverse. Treatment of pyoderma gangrenosum includes treating the underlying comorbidity supplemented with topical and/or systemic agents. However, treatment is often challenging. The aim of this study was to explore the diversity of pyoderma gangrenosum and its treatments. A total of 64 patients with pyoderma, at the Department of Dermatology, Aarhus University hospital, Denmark, were included in the study. The patients’ records were reviewed over a 6-year period for clinical presentation, associated diseases, treatments and response to treatment, time to mortality after diagnosis and prednisone dose over time. A variety of accompanying comorbidities were found, including a possible association with diabetes. Tumour necrosis α inhibitors were used as third- or fourth-line therapy, but showed the shortest time to remission, and use of prednisone was associated with a higher mortality rate. These findings are discussed in relation to future approaches to treatment of pyoderma gangrenosum.
Key words: pyoderma gangrenosum; comorbidity; immunosuppressants; prednisone; mortality rate.
Accepted Feb 23, 2021; Epub ahead of print Mar 9, 2021
Acta Derm Venereol 2021; 101: adv00431.
doi: 10.2340/00015555-3776
Corr: Louise Schøsler, Palle Juul-Jensens Blvd. 99, DK-8200 Aarhus, Denmark. E-mail: louischo@rm.dk
Pyoderma gangrenosum is a challenging skin condition to identify and treat. It often lacks response to treatment and is associated with underlying diseases. This study included 64 patients with pyoderma gangrenosum, aiming to explore the diversity of the disease, its treatments and response. A variety of accompanying diseases were found, including a possible association with diabetes. The first-line drug of choice was prednisone, which was associated with a higher mortality rate. Tumour necrosis factor α inhibitors were used as third- or fourth-line therapy, but showed the shortest time to remission, and should be considered in future treatment approaches.
Pyoderma gangrenosum (PG) is an uncommon ulcerative neutrophilic dermatosis. Its classic clinical presentation is ulceration with several variants (bullous, pustular and superficial granulomatous), which differ in their clinical presentation, location and associated diseases. Diagnosis of PG is usually based on clinical changes supported by histological examination of skin biopsy specimens from the margin of typical clinical ulcers (1). However, new diagnostic criteria have been proposed recently, based on a Delphi process (2). Some patients with PG have associated systemic diseases, such as inflammatory bowel disease (IBD), rheumatological and haematological conditions.
Treatment of PG includes treating the underlying comorbidity supplemented with topical or/and systemic agents. PG can be treated topically by applying steroids, either to the wound margin or to the entire wound bed. Calcineurin inhibitors may also be used topically (3). For systemic treatment of PG, prednisone is first-line therapy. Prednisone treatment may be combined with other immunomodulatory agents, such as cyclosporine (CsA), methotrexate (MTX), mycophenolate mofetil or azathioprine. Occasionally, dapsone is used for treatment of PG and may also be combined with prednisone and/or one of the above-mentioned immunomodulatory agents. Finally, tumour necrosis factor (TNF)-α inhibitors or interleukin 1 inhibitors may be used for PG treatment, usually in combination with prednisone (3).
The study was approved by the Danish Data Protection Agency as a retrospective study. In Denmark, diagnoses are coded according to the modified Danish version of the International Classification of Diseases (ICD-10). Patients were identified using the ICD-10 for PG, DL889, and chronic ulcer, DL984. All patient records with a diagnosis of chronic ulcer were manually reviewed to check if the patients had PG. A study population was established of all patients, > 18 and < 100 years of age, with new-onset PG or untreated PG relapse, diagnosed at the Department of Dermatology, Aarhus University Hospital, Denmark. Patient records were read from November 2011, when the records became electronic (the Danish midt-EPJ) to November 2017; a 6-year period.
A total of 64 patients were identified who met all the pyoderma criteria established by Daniel Su et al. (1). The criteria of Maverakis et al. (2) were proposed after these patients were diagnosed. The diagnosis was established using a combination of the following: histological findings with neutrophilic infiltrate, clinical characteristics with violaceus borders, cribriform scarring and typical localization, reports of either spontaneously debut or pathergy, comorbidities such as rheumatoid arthritis (RA)/IBD/hematological disease together with response to prednisone. Other differential diagnoses, such as infection, vasculitis and malignancy, were excluded. Patients with an uncertain diagnosis were evaluated by a specialist in dermatology to verify the PG diagnosis. Through the EPJ, data about PG cause, localization, comorbidities, biochemistry, body mass index (BMI), smoking habits, histology, treatments and response, time to mortality after diagnosis and prednisone dose over time were retrospectively and manually collected. A case group was established with mortality within 1 year after diagnosis and concurrent prednisone treatment. Furthermore a control group was established within the PG patient group who survived the first year after PG diagnosis. The controls were matched to the PG cases (mortality within first year after PG diagnosis) by age, severity of comorbidities and weight. By comparing the cases and controls, the current study aimed to verify whether prednisone dose was related to mortality. Prednisone dose was determined by tracking medicine prescriptions as well as data in the patient records.
The number of simultaneous treatments was registered during the most active wound phase. Treatment response was recorded as full remission, partial remission, or disease progression. Patient comorbidity was registered by ICD-10 diagnoses during the whole period until 2017, or until death. All data were recorded in an electronic table and statistically analysed using Excel (Microsoft Office 2016).
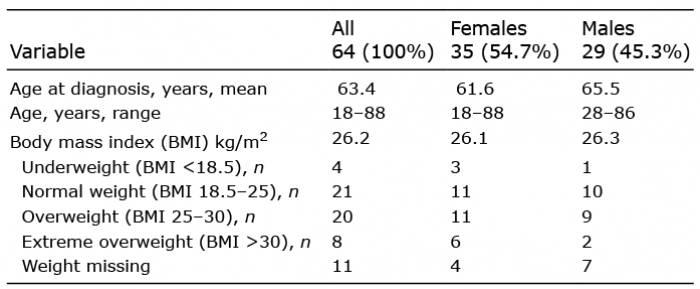
Data from 64 patients with PG as a primary diagnosis were analysed. The female-to-male ratio was 54.7/45.3%. The age range was 18–88 years, with a mean of 61.6 years for women and 65.5 years for men. The BMI was evaluable in 53 patients, whose mean BMI was 26.2 kg/m2 (range 15.8–41.8). The range of BMI was similar between the sexes (Table I).
Table I. Demographics: patient characteristics
Clinical and histological findings
The most common localization of PG lesions was the lower limbs (57.8%), followed by hands (6.2%) and genitals (6.2%). Less frequent locations included the abdomen (4.7%), the back (3.1%), followed by the buttocks (1.6%) and the upper limbs (1.6%). In 18.8% of cases, PG occurred simultaneously in at least 2 separate anatomical sites (Fig. 1). PG can be divided into several types, in the current study 85.9% had ulcerative form, 3.1% bullous form, 6.3% peristomal, 3.1% vegetative and 1.6% pustular form (Fig. 2).
Fig. 1. Pyoderma gangrenosum lesion localization by body area.
Fig. 2. Types of pyoderma gangrenosum.
The cause of PG was known in 51 out of 64 patients. Spontaneous development of PG was the most common cause (49%), followed by minor trauma (27.5%) and larger surgery/pathergy (17.6%) (Table II). C-reactive protein (CRP) values were available for 58 patients, with 56.9% having elevated levels. Smoking habits were known in 63 patients. Active smoking/nicotine consumption was documented in 15.9% of patients, former consumption in 28.6%, and no consumption in 55.5%.
Twenty-one patients (32.8%) died within the study follow-up period. Although there are no pathognomic histological findings, this study examined the histopathological descriptions available for 56 patients. Of this total, 16 patients had immunomodulatory therapy before biopsy and 5 of these had a neutrophilic infiltrate. Biopsy in the remaining 40 patients showed a neutrophilic infiltrate, early abscess formation, or inflammation around hair follicles in 26 patients (65%).
Table II. Cause of pyoderma gangrenosum lesion in 51 out of 64
Comorbidities
The most common comorbidity was IBD (28.1%). Diabetes mellitus (DM) type II, diagnosed before PG, occurred in 21.9%; of which only one patient had prednisolone-induced diabetes. Diseases of the cardiovascular system (stroke, cardiac failure, ischaemic heart disease (IHD), and arteriosclerosis with bypass procedure) were detected in 20.3% of the patients. Some of the patients with PG had endocrinological diseases (12.5%), haematological diseases (7.8%) or rheumatoid arthritis (RA) (12.5%). A total of 6.3% of the patients had malignancy before PG was diagnosed, whereas 14.1% of the patients developed malignancy after the PG diagnosis had been established (Table III).
Table III. Comorbidities
Therapy and follow-up data
Topical agents were used as single treatment in 8 patients. These 8 patients showed full remission of PG, with a mean progression-free survival of 7.3 months. The remaining 56 patients were treated with a combination of topical agents and systemic therapy. Systemic corticosteroid treatment was the most frequently used therapy (91.1%), followed by MTX (44.6%) and CsA (32%) (Table IV). Among the 56 patients who received combination therapy with topical and systemic therapy, 32.1% were treated with single-agent systemic therapy (Table V). Prednisone was first-line therapy in 15 patients (26.8%), 12 of whom experienced complete remission (80%). Overall, patients treated with monotherapy had a mean time to remission of 9.9 months (Fig. 3). In patients treated with 2-drug therapy, 14 out of 16 had complete remission (87.5%), with a mean time to remission of 13.9 months.
Table IV. Systemic therapy in pyoderma gangrenosum patients
Table V. Systemic therapy in pyoderma gangrenosum patients
Fig. 3. Systemic therapy related to time to remission of pyoderma gangrenosum lesions.
The most common 2-drug therapy combination was prednisone and MTX. This combination was given to 37.5% of the patients (Table VI). Complete remission was seen in 83.3% of the patients who were treated with prednisone and MTX, whereas all patients (100%) treated with the 2-drug combination of prednisone and CsA experienced full remission (Table VI). Time to remission was shortest for the combination of prednisone and the TNF-α inhibitor infliximab. Three-drug therapy with immunomodulatory agents was used in 13 of 56 patients. Nine of these patients had complete remission, 1 patient had partial response, and 3 of these patients had disease progression. Mean time to remission was 20.3 months for patients on 3-drug therapy (Fig. 3). The most common combination of 3-drug therapy was prednisone, MTX and a third immunomodulatory agent (Table VI). Nine patients were treated with +4 drug therapy, and 4 of these still had progression at the end of follow-up (2017), 2 patients had partial response, and 3 patients had full remission. Patients treated with +4 drug therapy had a mean time to disease remission of 24.7 months. The most common combination was prednisone, MTX and CsA combined with other immunomodulatory agents. Time to remission related to PG type showed a mean time to remission of one month in bullous types, 11 months in peristomal, 16.9 months in ulcerative, 25 months in pustular, and 46 months in vegetative types (Fig. 4).
Time to remission related to nicotine consumption was 18.7 months in active consumption, 10.1 months in former consumption, and 18.8 months in no consumption.
Table VI. Therapy combinations related to time to remission in months
Fig. 4. Time to remission related to pyoderma gangrenosum type.
Prednisone related to mortality
This study identified patients who were treated with prednisone and died within the first year after their PG diagnosis. Six patients met these criteria; 5 men and 1 woman. Their age range was 63–86 years. Of these, 14.3% were active smokers, 28.6% were former smokers, and 57.1% were non-smokers. All patients who died within the first year of PG diagnosis had the ulcerative type of PG.
The cumulative dose of prednisone administered to each of these patients was 25.9 mg daily during the first 0–3 months, 16.1 mg daily after 3–6 months, 29.0 mg daily after 6–9 months, and 23.2 mg daily after 9–12 months. Only one patient was alive after 9 months. A control group was identified within the total study population. The controls had to be treated with prednisone and to survive the first year after their PG diagnosis. The controls were matched to the cases with respect to age and weight. The prednisone dose for controls was 18.1 mg daily after 0–3 months, 11.7 mg daily after 3–6 months, 18.9 mg after 6–9 months and 29.7 mg after 9–12 months (Figs 5 and 6).
Fig. 5. Cumulative prednisone dose over time.
Fig. 6. Weight-adjusted cumulative prednisone dose over time.
This study confirms that PG is a disease characterized by a heterogeneous clinical presentation, and that patients with PG have a wide range of comorbidities. Whether the comorbidities identified are truly associated with PG or simply co-exist with PG remains a matter of discussion (4–6). In addition, this study found great variation in treatment approaches to PG, even within a single department of dermatology (3, 7).
Clinical findings
This study showed that slightly more women (54.7%) than men (45.3%) presented with PG. Mean age at PG diagnosis was 61.6 years for women and 65.5 years for men, which is in line with the findings of other studies (5, 8). Histological examination of perilesional biopsy specimens was available in 56 of the 64 patients; 40 patients were without prior immunomodulatory therapy; in 65% of these, a neutrophilic infiltrate, early abscess formation or inflammation around hair follicles was found. This finding underlines that PG may exist without specific histopathological changes. Even so, a neutrophilic infiltrate in the dermis is part of the diagnostic criteria of PG according to Maverakis et al. (2).
Comorbidities
Table III presents the comorbidities observed in the current study population. The most frequent comorbidity was IBD (Crohn’s disease and ulcerative colitis), which is similar to data reported by Kridin et al. (9). IBD was found in 28.1% of study patients. DM type II was found in 21.9% of patients with PG, and cardiovascular disease (stroke, cardiac failure, IHD and arteriosclerosis with bypass procedure) in 20.3% of patients. These findings are unsurprising, and are supported by other studies, except for the relatively high prevalence of DM type II (10, 11). To our knowledge, the relatively high occurrence of DM type II has been described only a few times before, varying between 25.1% and 28.6% of PG cases (5, 8, 10). Jockenhöfer et al. (8) showed that 94.8% of patients with PG had signs of metabolic syndrome, including obesity and dysfunction of lipid metabolism, which can be correlated with the finding from the current study of a mean patient BMI of 26.2 kg/m2. Compared with the Danish population, in which 4.6% of all citizens have DM type II (data from the Danish register of chronic diseases, RUKS), patients with PG have a much higher prevalence of diabetes. This may partly be explained by the pathophysiology of both diseases, as both diabetes and PG are thought to be caused by an autoinflammatory process (12, 13).
Causes of pyoderma gangrenosum
Table II outlines the causes of PG in the study patients. In 25 out of 51 patients, PG wounds occurred without any skin-related cause; and in 3 patients, infection preceded onset of PG. Trauma or surgery was reported in 23 of 51 patients. The latter may be related to the pathergy phenomenon described in PG (14, 15). Pathergy should be kept in mind in all pyoderma cases in which surgery is considered, because surgery can lead to aggravation of pyoderma, development of pyoderma or even mimic necrotising fasciitis (15).
Treatment
Tables IV and V show the treatments given to the study patients with PG. The majority of patients (91.1%) were treated first line with prednisone. In 26.8% of the included PG patients, prednisone was used as monotherapy. However, the majority of patients were treated with additional drugs: in 28.6% of PG patients, 2-drug therapy was used; and in 23.2%, a 3-drug therapy was applied. In 16.1% of cases, a 4+ therapy was given. The majority of PG patients (87.5%) were treated with systemic drugs, further supporting the severity of PG in the current study population. Table VI outlines the different PG treatment regimens used in our department. In the literature, prednisone combined with CsA is the most frequently used treatment combination for PG (3, 16, 17). In contrast, the most frequently used treatment combination in our department was prednisone combined with MTX. TNF-α inhibitors were also used for treatment of PG in our study population (Table VI). However, TNF-α inhibitors were used as third- or fourth-line drugs. The addition of TNF-α inhibitors led to further improvement in PG. Recently, the literature has been reviewed with respect to TNF-α inhibitors (18), and it was found that these relatively new drugs are useful in the treatment of PG. This review shows that there is no significant difference between the effectiveness of infliximab, adalimumab and etanercept. Other case reports and reviews have also focused on the use of biologics in PG (17, 19–21) and found that biologics are efficacious and safe in the treatment of PG. Biologics may therefore be prioritized in future treatment of PG, and considerations may be made that TNF-α inhibitors may be used as second-line (or even first-line) therapies in order to avoid prednisone-related morbidity and mortality. However, controlled clinical studies are needed to support this assumption.
Prednisone and mortality
Figs 5 and 6 show that the use of prednisone was associated with a higher mortality rate in PG cases than in the matched control group. In patients with RA, Saag et al. (22) showed a dose-response relationship between prednisone and sepsis as an adverse effect (AE), with a mean prednisone dose in the 10–15 mg/day range being correlated with development of an AE. This observation raises concerns about high-dose prednisone treatment in PG and other skin diseases. The observed prednisone-related mortality underlines that steroid-sparing treatment should be instituted shortly after diagnosis of PG.
Conclusion
This study confirms that PG is characterized by a heterogeneous clinical presentation and a variety of associated comorbidities. The study data demonstrate a possible association with DM type II, which should be taken into consideration in patients with newly diagnosed pyoderma.
Prednisone dose was associated with a higher mortality rate. This encourages us to initiate steroid-sparing treatment as soon as possible after diagnosis of PG. TNF-α inhibitors were used as third- or fourth-line treatments in the current study. Even so, TNF-α inhibitor treatment showed the shortest time to PG remission. Consequently, TNF-α inhibitors might be considered first- or second-line therapies in future treatment of PG.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize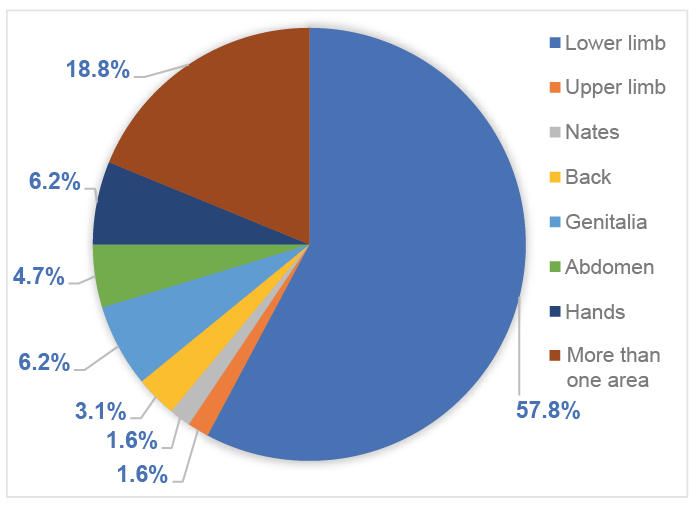 Click to show fullsize
Click to show fullsize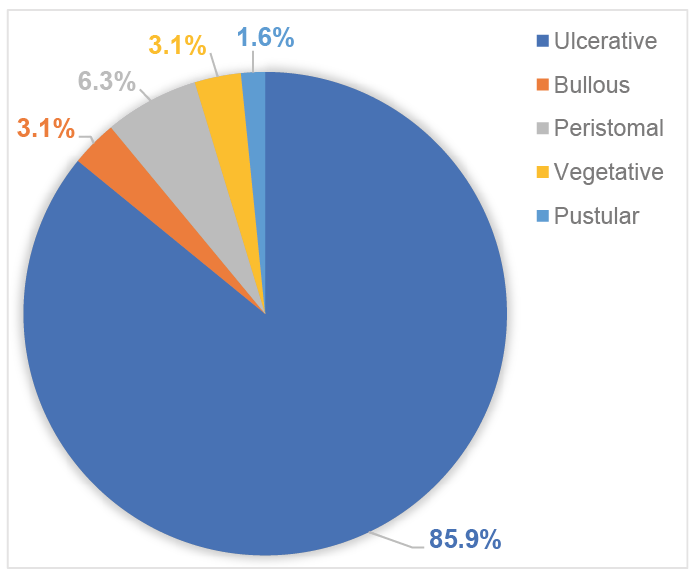 Click to show fullsize
Click to show fullsize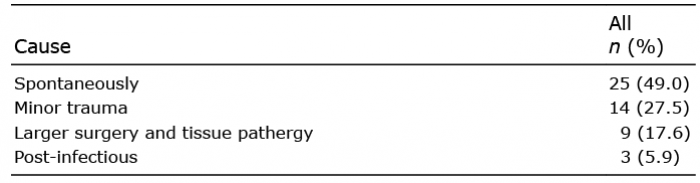 Click to show fullsize
Click to show fullsize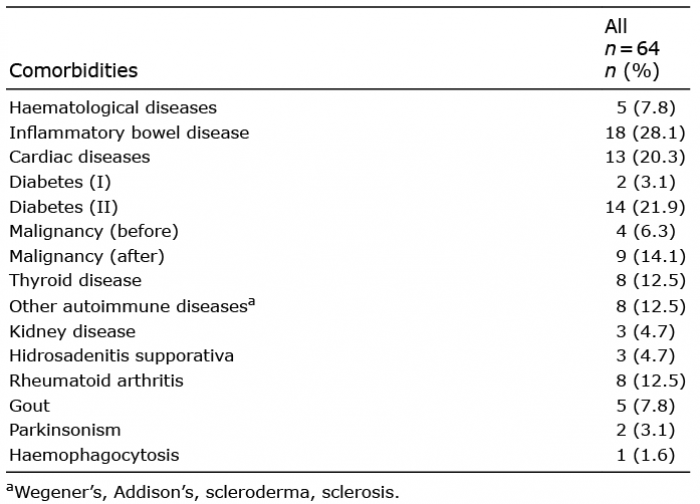 Click to show fullsize
Click to show fullsize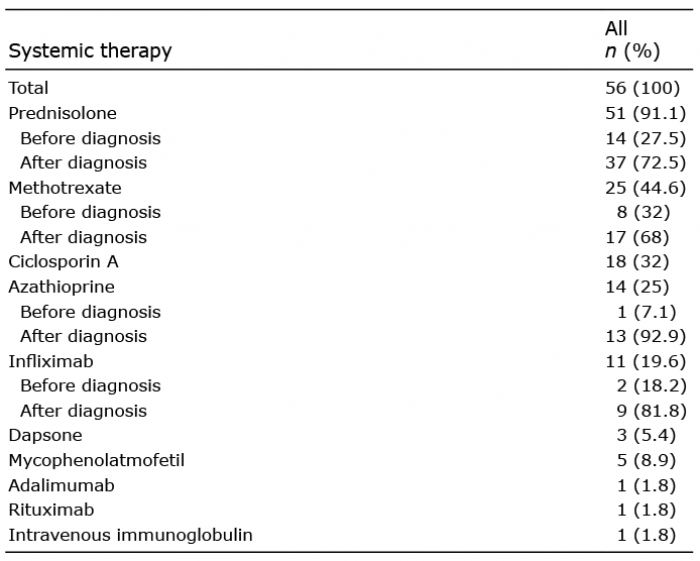 Click to show fullsize
Click to show fullsize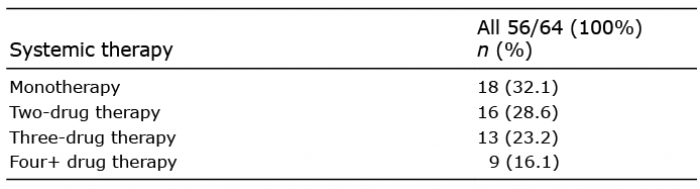 Click to show fullsize
Click to show fullsize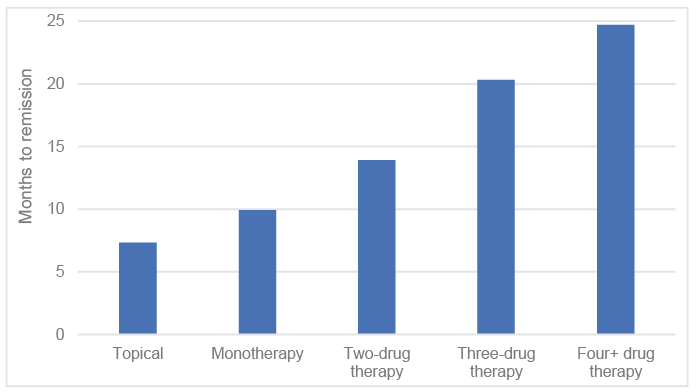 Click to show fullsize
Click to show fullsize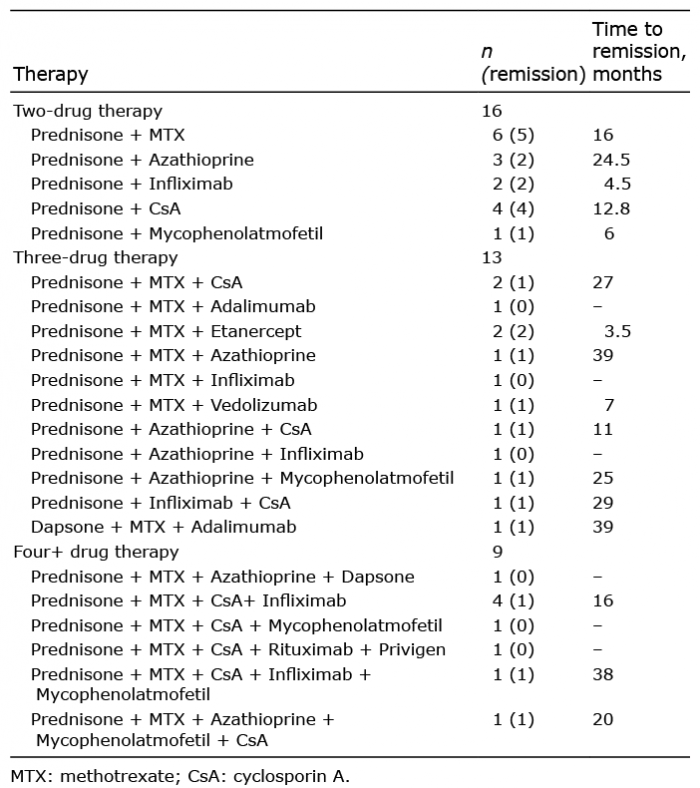 Click to show fullsize
Click to show fullsize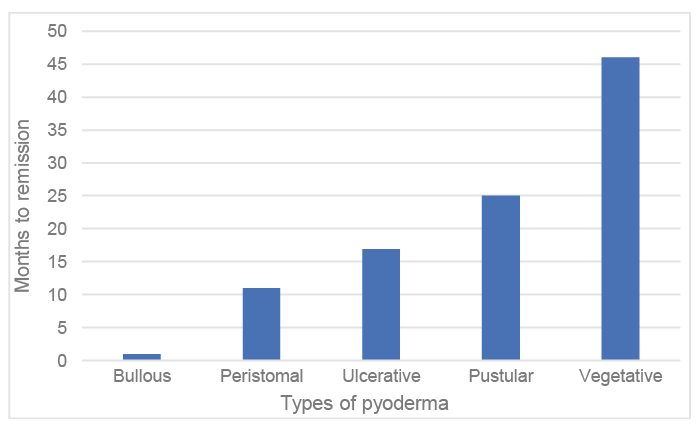 Click to show fullsize
Click to show fullsize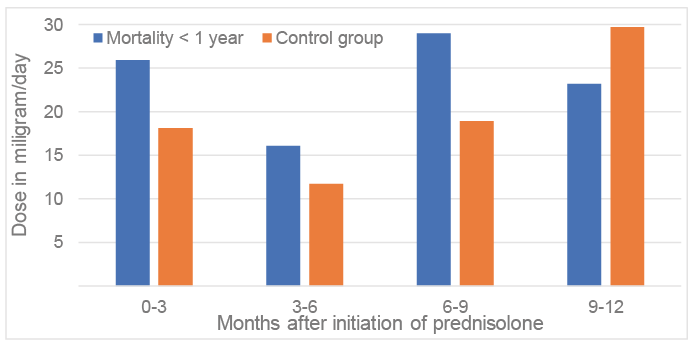 Click to show fullsize
Click to show fullsize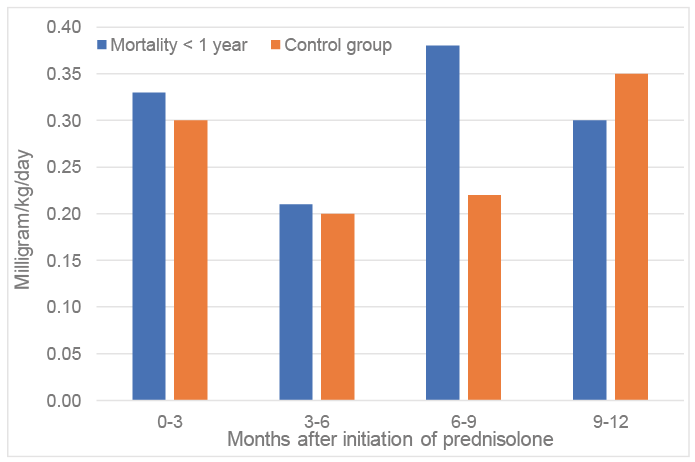 Click to show fullsize
Click to show fullsize