


Department of Dermatology and INSERM 1098 RIGHT, University Hospital, 3 Bd Fleming, FR-25030 Besançon, France. *E-mail: francois.aubin@univ-fcomter.fr
Accepted Feb 23, 2021; Epub ahead of print Mar 9, 2021
Acta Dermm Venereol 2021; 101: adv00451.
doi: 10.2340/00015555-3779
Idiopathic facial aseptic granuloma (IFAG), also called cold pyoderma, was first described in 1999 as a chronic, inflammatory, painless facial nodule similar to a cold abscess in children (1). Regarding the pathophysiology, IFAG is considered as a part of the spectrum of granulomatous rosacea in childhood (2–5). Chalazions are induced by inflammation and obstruction of Meibomian glands, which are located inside the eyelid tarsus. We report here 6 children with lower eyelid nodules and discuss the diagnosis of IFAG or chalazion (6).
Patient A. A 6-year-old girl, without relevant medical history or treatment, consulted our dermatology clinic, referred by ophthalmologists, with 2 asymptomatic bilateral and symmetrical sub-palpebral nodules, that had developed over several weeks (Fig. 1A). Local treatment with warm/hot moist compresses and oral amoxicillin was ineffective. The diagnosis of IFAG of the lower eyelids was suggested, and treatment with josamycin propionate for 30 days and topical 3% metronidazole preparation for 6 months resulted in clinical improvement within 30 days and total disappearance of the lesions within 3 months. Patient B. An 11-year-old girl, presented with an inflammatory, painless and chronic nodule of the left lower eyelid (Fig. 1B). Ultrasonography revealed a hypoechoic lesion located in the dermis, with intralesional blood flow, without any calcification. A diagnosis of IFAG was made and a treatment with josamycin propionate was effective within 2 months. Patient C. A 3-year-old girl presented with a characteristic IFAG lesion of the left cheek associated with bilateral and symmetrical nodules of the eyelid (Fig. 1C). Treatment with clarithromycin and topical 3% metronidazole preparation resulted in clinical improvement within 3 weeks. Patient D. A 5-year-old girl presented with bilateral and symmetrical subpalpebral nodules evolving for 8 weeks (Fig. 1D). Diagnosis of IFAG was made. The clinical course was spontaneously favorable in 5 weeks without any treatment. Patient E. A 3-year-old girl presented with a subcutaneous, inflammatory, painless nodule located on the left lower eyelid (Fig. 1E). The lesion had been evolving for several months without any healing tendency, despite antibiotic treatments with roxithromycin followed by amoxicillin-clavulanic acid. Ultrasonography showed an ovoid poorly echoic lesion located in the dermis with perilesional blood flow. No calcification was observed. A diagnosis of IFAG was made. The clinical course was favourable with a 1.5% azithromycin ophthalmic solution 3 days in a row, every 15 days for 3 months. Patient F. A 5-year-old girl presented with a chief complaint of a 3- to 4-day history of right eyelid swelling, pain, and redness. Clinical examination showed a well-delimited warm and tender nodule of the right eyelid (Fig. 1F). Diagnosis of chalazion was made. Treatment with warm compresses and topical mupirocin resulted in clinical improvement in a few days.
Fig. 1. Nodules of the eyelids and cheek diagnosed as idiopathic facial aseptic granuloma in patients A, B, C, D, and E and as chalazion in patient F. Permission is given to publish these photos.
We report here 6 children with lower eyelid nodules, which may be suggestive of IFAG or chalazion. Chalazion commonly presents as a nodule of an eyelid. It arises from inflammation and obstruction of the sebaceous Meibomian glands of the eyelid tarsal plate. Inferior tarsus is a thin, elongated plate of dense connective tissue, approximately 2.5 cm in length, with a vertical diameter of approximately 5 mm. Although asymptomatic chalazion may resolve spontaneously, treatments of chalazion include moist hot compresses, and topical antibiotics and/or steroids (7). Excision under local anaesthesia may be required in case of persistence or recurrence. An alternative to surgery involves administering a steroid intralesional injection into the affected gland to reduce the inflammation.
In contrast, IFAG represents a unique paediatric dermatological entity (Table I) related to childhood rosacea (2, 5, 7), which should be recognized and managed non-aggressively (2). Although partial improvement may be observed after topical and/or oral macrolide therapy, the evolution of IFAG is usually spontaneously favourable, without scarring and relapse within a few months (2–4, 8, 9). The link between IFAG, childhood rosacea and ophthalmological damage, including recurrent chalazia, is now well established (3–5, 8, 10). In a retrospective observational case-control study (10), rosacea was found as a statistically significant risk factor of chalazion (odds ratio (OR) 2.9). In a previous study (3) including 38 IFAG, 42% of patients had a final diagnosis of childhood rosacea with ocular rosacea in 75% of cases. It was remarkable to notice that among them, 50% had a history of recurrent chalazions. This association was confirmed in different cases reports (4, 8, 9).
Table I. Differential diagnosis between idiopathic facial aseptic granuloma (IFAG) and chalazion
Furthermore, extra-tarsal chalazia have been reported (11, 12), as well as the location of IFAG lesions on the eyelids (2, 3). Altogether, these results emphasize the difficulty of differentiating IFAG from chalazion when inflammatory nodules are localized in a peripalpebral area (6, 13). However, medical history, clinical course, ultrasound imaging, and histology may be helpful (Table I).
In the series reported here, patients C and D had clinically compatible lesions with chalazia because of the proximity to the lower tarsus. However, in patient C, the association with a cold pyoderma lesion of the left cheek led to the diagnosis of IFAG of the lower eyelid. Patients A, B and E presented with nodules of the lower eyelids developed at distance from the tarsus, and were therefore rather suggestive of IFAG.
Ultrasound imaging and histology have been proposed to differentiate IFAG from chalazion (4, 14). IFAG lesion demonstrates a well-delimited hypoechoic structure of the superficial and deep dermis with a small amount of vascularity and the lack of calcium deposits. Skin biopsy of IFAG shows consistent histology of folliculitis and perifolliculitis with well-demarcated granulomas with palisading histiocytes, scattered foreign body giant cells, neutrophils, lymphocytes, and some plasma cells, further supporting the hypothesized relationship between IFAG and granulomatous rosacea (4, 8). Histologically (15), a chalazion is characterized by the formation of granulomas, each with a central clear space representing lipid globules, which are composed of epithelioid cells and lipid-filled, Touton-type multinucleated giant cells intermixed with acute and chronic inflammatory cells. A pseudocapsule of connective tissue often forms around the lesion.
Chronic subepidermal eyelid nodules resembling chalazion or skin abscess should alert clinicians to a diagnosis of IFAG. Because IFAG may resolve spontaneously or with oral macrolides, unnecessary surgical intervention should be avoided. Furthermore, regular clinical follow-up of these children in ophthalmology and dermatology is essential, with the aim of early diagnosis and treatment of ocular rosacea.
The authors thank the patients and Elisabeth Homassel for her technical assistance.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize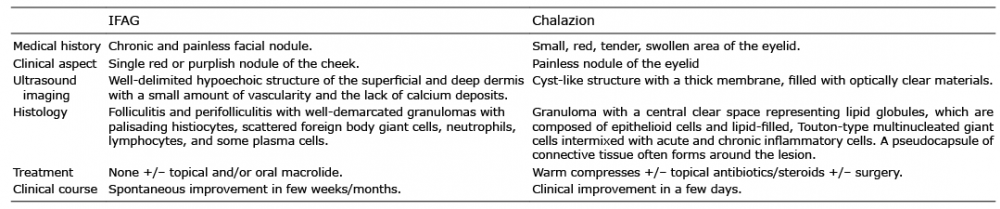 Click to show fullsize
Click to show fullsize