


1Department of Dermatology, Faculty of Medicine Siriraj Hospital, Mahidol University, Bangkok, Thailand and 2Cutaneous Biology Research Center, Massachusetts General Hospital, Harvard Medical School, Boston, MA, USA
Topical corticosteroid delivery following fractional laser treatment is an effective means of treating hypertrophic scars. However, the relative efficacy of adjuvant corticosteroid treatment vs fractional laser monotherapy alone is unclear. The aim of this study was to compare the efficacy and safety of fractional laser-assisted topical corticosteroid delivery with fractional laser monotherapy in the treatment of hypertrophic scars. In this randomized, comparative, split-scar trial of 19 subjects, a borderline significant reduction in scar thickness was observed at 3-month follow-up in the laser+steroid group compared with laser+petrolatum (p = 0.049). However, no significant long-term difference in scar flattening was observed between the 2 groups. Patient and Observer Scar Assessment Scale scores showed significant improvement in scar appearance from baseline without significant differences between treatment groups. In conclusion, fractional laser monotherapy is an effective treatment for hypertrophic scars, and the application of topical corticosteroid provides no long-term synergistic effect to fractional laser monotherapy.
Key words: hypertrophic scar; fractional laser; laser-assisted drug delivery; corticosteroid.
Accepted Feb 25, 2021; Epub ahead of print Mar 9, 2021
Acta Derm Venereol 2021; 101: adv00416.
doi: 10.2340/00015555-3781
Corr: Woraphong Manuskiatti, Department of Dermatology, Faculty of Medicine Siriraj Hospital, Mahidol University, 2 Wanglang Road, Bangkok 10700, Thailand. E-mail: Woraphong.man@mahidol.edu
The efficacy of topical steroid delivery immediately after fractional laser irradiation compared with fractional laser monotherapy in the treatment of hypertrophic scar remains unclear. A split-scar, double-blind comparative study was conducted among 19 patients with hypertrophic scar to compare the efficacy and safety of fractional laser-assisted topical corticosteroid delivery with fractional laser monotherapy. However, no clinically significant difference was found between the 2 groups in the long term. Therefore, prospective studies are recommended to further evaluate the benefit of fractional laser-assisted steroid delivery in the treatment of hypertrophic scars.
Keloid and hypertrophic scars (HTS) represent an abnormal variant of normal wound healing, characterized by fibroblast hyperproliferation and excess collagen formation (1). Hypertrophic scarring can occur in all patients, but darker-skinned individuals are more susceptible, with an incidence of 6–16% in populations of African descent (2). Individuals with darkly-pigmented skin have a greater propensity to form hypertrophic scars and keloids in response to trauma compared with Caucasians, with a relative ratio of 5:1 to 15:1, depending on ethnic background (3). In addition to the physical discomfort of HTS, the aesthetic dimensions of scarring can affect the patients’ quality of life due to perceived stigma and psychological distress (4). Current available treatment modalities include the application of topical and intralesional steroids, silicone gels sheets, compression therapy, cryotherapy, laser therapy, radiation, and surgical excision, each with varying degrees of success (5, 6).
Intralesional corticosteroid injection remains one of the most widely used first-line monotherapy (1) and adjuvant treatments (7) for keloids and HTS. Corticosteroids act as potent glucocorticoids, suppressing the inflammatory response during the initial wound healing process and increasing collagenase activity by downregulating inhibitors, such as α-1-antitrypsin and α-2-macroglobulin, thereby promoting local collagen degradation (8). The current standard practice is a series of intralesional injections given every 2–4 weeks until the scar is flattened and its borders softened (5).
In a previous study, the efficacy of intralesional injection was compared with either steroid or 5-fluorouracil (5-FU) relative to pulsed dye laser (PDL) treatment for the resolution of scarring (9). While intralesional modalities provided faster resolution and better scar response compared with PDL, they were associated with a higher incidence of adverse reactions, including the development of telangiectasias, skin and subcutaneous fat atrophy, pigmentary changes (hypopigmentation and hyperpigmentation), skin necrosis, ulcerations, and Cushing’s syndrome (10). Furthermore, repeated injections are associated with significant pain, leading to poor compliance and patient retention, invariably lessening the effectiveness of the treatment (11).
Recently, fractional laser-assisted drug delivery (FLADD) following ablative fractional laser (AFXL) has been suggested as a means of combining the beneficial effects of corticosteroid delivery with the lower side-effect profile of laser treatment (12). Theoretically, generating small ablation channels through the stratum corneum provides an alternative pathway for transcutaneous drug delivery along with the therapeutic effects of creating microscopic injury zones that promote endogenous tissue remodelling. Transcutaneous delivery has the potential to overcome the side-effects of systemic delivery, while maintaining therapeutic concentrations of the drug in target tissues. Furthermore, FLADD may be used as an alternative to intralesional injections to minimize pain and decrease the incidence of adverse reactions associated with steroid administration. This study compares the efficacy and safety of fractional laser-assisted topical corticosteroid delivery with fractional laser monotherapy in the treatment of HTSs.
Subject assessment
This was a prospective, randomized, split-scar, double-blind comparative clinical study. A total of 24 female subjects, with Fitzpatrick skin types (FSTs) III–IV, diagnosed with abdominal HTS resulting from caesarean section or appendectomy, presenting at least 6 months prior to enrollment, were included. The study was approved by the Siriraj Institution Review Board (SIRB), Faculty of Medicine Siriraj Hospital, Mahidol University, Thailand (Si 728/2013) and was registered at www.clinicaltrials.gov (NCT02487212). The study was conducted between April 2014 and January 2016. Written informed consent was obtained from all subjects prior to treatment.
All subjects received 4 treatment sessions at 2-week intervals with a fractional Er:YAG laser (XS Dynamis, Fotona d.o.o., Ljubljana, Slovenia) at a fluence of 28 J/cm2, pulse width 300 µs, and 5% density distributed over the entire scar. A commercially available air-cooling machine (Cryo 6, Zimmer Aesthetics, Germany) was used to minimize pain and discomfort.
Each scar was divided in half lengthwise and randomized. Scar segments were randomly assigned to “laser+steroid” or “laser+petrolatum” intervention groups. Randomization was carried out using a block randomization plan generated from www.randomization.com. Half of each scar was assigned to the “laser+steroid” group and received laser treatment, followed by immediate topical steroid application using clobetasol propionate 0.05% ointment (Dermovate® ointment, GlaxoSmithKline UK, Brentford) spread in a thin layer (approximately one fingerbreadth per 1 cm scar length) gently rubbed in the scar for 1–2 min. The second half, or “laser+petrolatum” group, was treated with laser monotherapy alone and topical application of petrolatum. Only the treating physician (WM) was aware of the scar assignment, while physician-observers involved in preliminary and post-treatment assessments of scars were blinded to the distribution of experimental groups.
Postoperatively, scars were occluded under a transparent film dressing (Tegaderm™, 3M Health Care, St Paul, MN, USA) left in place for at least 3 h. Subjects were instructed to apply petrolatum 4 times daily for the next 7 days.
Clinical assessment
The primary study outcome was reduction in HTS thickness perpendicular to the plane of the skin, measured with a dial caliper (Mitutoyo, Kawasaki, Japan). The mean of 3 measurements at the maximum vertical elevation of each scar segment above the normal plane of the skin was obtained before treatment and at every follow-up.
Subjective evaluation using the Patient and Observer Scar Assessment Scale (POSAS) was conducted by 2 single-blinded dermatologists and each subject (13). The assessors evaluated changes in the following parameters: vascularization, pigmentation, thickness, relief, pliability, and surface area. Vascularity was assessed by pressing a glass slide on and around each scar and evaluating capillary refill during release. To judge variation in pigmentation, scars were blanched using glass slides to eliminate the confounding effect of vascularity. In the patient portion of POSAS, parameters such as pain, itching, colour, stiffness, thickness, and relief were evaluated. The 6 items on each portion were scored numerically on a 10-step scale and together made up the total score. All assessments were conducted at baseline, 2 weeks after the 2nd treatment, and at 1-, 3-, and 6-month follow-up after the final treatment. Recovery times and adverse effects were recorded at each treatment session and follow-up visit. All clinical photographs were taken with identical camera settings, lighting, and positioning using a Canon Rebel T5i camera with a TwinFlash® RL (Can?eld Scienti?c, Inc., Fair?eld, NJ, USA).
Statistical analyses
Descriptive analysis was used for demographic data. Data was analysed using 2-sided paired t-test with a 95% confidence interval (95% CI) to assess the difference between the control and treatment groups. Repeated measure analysis of variance (ANOVA) was used to compare differences between individual split-scars. Statistical analysis was performed using statistical software (IBM SPSS version 24.0; IBM, Armonk, NY, USA) with a p-value of < 0.05 considered significant.
Nineteen of 24 subjects (79.2%) successfully completed the study protocol and were included in the final analysis. Five subjects withdrew from the study due to scheduling conflicts or were lost to follow-up. The mean age of the study subject was 34 years (range 24–45 years) and the majority had FST IV (89.5%). The median scar duration was 10 months (range 6–50 months).
Hypertrophic scar thickness
There were no significant differences between mean scar thickness between the 2 treatment groups at baseline (p = 0.314). In both laser+steroid and laser+petrolatum branches, the mean scar thickness showed significant improvement compared with baseline at all timepoints with p = 0.009 and p = 0.001, respectively. However, no significant difference in HTS thickness was present between the 2 experimental groups at all follow-up visits (Table I and Fig. 1).
Table I. Hypertrophic scar thickness assessment from baseline to all follow-ups
Fig. 1. A 1-year-old hypertrophic appendectomy scar of a 30-year-old patient with FST IV. (a) Before treatment; (b) 6 months after 4 treatments.
Mean differences in HTS thickness between baseline and follow-ups are shown in Fig. 2. At 3-month follow-up, there was a significant mean difference in reduction from baseline between the laser+steroid (0.42 mm) and laser+petrolatum (0.32 mm) experimental groups (95% CI 0.001–0.21; p = 0.049). At 6-month follow-up, there was continued improvement in the mean difference on both segments (0.45 and 0.35 mm); however, the difference between experimental groups was not statistically significant (95% CI –0.03–0.22; p = 0.123).
Fig. 2. Mean difference of scar thickness from baseline.
Patient and Observer Scar Assessment Scale
Prior to treatment, the observer portion of POSAS showed no significant difference between the 2 treatment segments at baseline (Table II). The mean POSAS scores in both laser+steroid and laser+petrolatum branches showed significant improvement compared with baseline (p < 0.001) No significant differences between experimental and paired control groups were present at the final follow-up.
The patient portion of POSAS showed no significant difference between the 2 treatment segments at baseline (Table II). The mean POSAS scores in both laser+steroid (p < 0.001) and laser+petrolatum (p = 0.001) branches showed significant improvement compared with baseline. No significant differences were observed between experimental groups at any follow-up visit.
Table II. Patient and Observer Scar Assessment Scale assessment from baseline to all follow-ups
Recovery times and adverse effects
Differences in microscopic scabbing between laser+ steroid (6.26 ± 2.6 days) and laser+petrolatum (and 6.10 ± 2.5 days) experimental groups were not statistically significant (p = 0.331). In addition, there was no statistically significant difference (p = 1.000) between the mean durations of erythema in the laser+steroid and laser+petrolatum groups (2.52 ± 1.7 and 2.53 ± 1.6 days, respectively). No adverse effects were reported at any follow-up visit. Telangiectasias, dyspigmentation, skin atrophy, and acneiform eruption were not observed in any participants.
The use of ablative fractional laser treatment in combination with topical corticosteroid application, known as FLADD, is posited to provide efficient drug delivery through the microscopic channels created by laser ablation (12). Previous studies have established the benefit of both non-ablative (14, 15) and ablative (16, 17) monotherapy fractional laser techniques for the treatment of HTSs and keloids. Thermal energy delivered by fractional laser devices produces a controlled microwounding within hypertrophic scars, thereby inducing wound remodelling leading to clinical improvement (18). The remodelling process is hypothesized to be primarily mediated by an increase in TGFβ3/type III collagen as seen in early wound healing and scarless fetal healing; however, a complex cascade of collagenases and the modulation of fibrotic pathways have complicated this picture (19). In terms of long-term clinical outcomes, fractional laser treatment is superior to other available treatment modalities, wherein the scars often recur or clinical improvement stops after treatment discontinuation (1, 20). Histological analysis of post-fractional laser treatment shows normal-appearing collagen, an increase in the number of blood vessels with improved vascular function, and the reappearance of a papillary (rather than effaced) epidermis (19, 21).
A number of recent studies have attempted to combine the effects of fractional laser therapy with transcutaneous drug delivery to alter the inflammatory pathways at play and increase the clinical efficacy of treatment. Waibel et al. (22) demonstrated a mean overall improvement of 2.73 on a 0–3 scale of HTSs using fractional ablative CO2 laser treatment coupled with immediate post-operative topical application of a triamcinolone acetonide suspension (concentration 10 or 20 mg/ml) in 15 patients. Similarly, Cavalie et al. (23) conducted a single-arm study of 23 patients with 70 keloids, showing a 50% improvement in scar appearance after 9 sessions of ablative fractional erbium laser treatment integrated with topical betamethasone cream under occlusion twice daily. Park et al. (24) compared the efficacy of fractional Er:YAG laser-assisted topical desoxymethasone ointment delivery with fractional laser treatment of HTSs followed by intralesional triamcinolone acetonide (10 mg/ml) injections. The results showed significant improvement in the Vancouver Scar Scale (VSS) scores compared with baseline; however, no significant differences were noted between 2 treatment modalities (24). Finally, Sabry et al. (25) weighed the relative benefits of verapamil and 5-FU FLADD against fractional CO2 laser monotherapy for the treatment of HTSs and keloids, finding that combination therapy (CO2+verapamil and CO2+5-FU) showed greater improvement over the laser monotherapy in all scar characteristics, except improvement in pigmentation, which was equally poor in all experimental groups.
With the exception of Sabry et al. (25), whose sample size for each intervention was only 10 subjects per group, the aforementioned studies uniformly failed to directly compare the effects of FLADD and laser monotherapy. Previous investigations of FLADD have not adequately dissociated the therapeutic effects of laser monotherapy, therapeutic agent, and their combination. We believe that the split-scar experimental model used in the current study overcomes the shortcomings of the earlier studies and effectively differentiates the effects of laser monotherapy and FLADD.
While multiple single-armed clinical studies promote the use of fractional laser-assisted corticosteroid delivery for the treatment of HTSs and keloids, the current study did not demonstrate a clinically significant difference between FLADD and laser monotherapy in the long term (22–24). Although the laser+steroid branch exhibited a borderline significant improvement in scar flattening over the laser+petrolatum branch at 3-month follow-up (95% CI 0.001–0.21; p = 0.049), differences were not significant at later follow-up visits. Furthermore, the POSAS scores did not demonstrate significant differences between experimental groups at any follow-up assessment. HTSs continued to improve over the period of at least 3–6 months after treatment discontinuation, similar to previous observations (14, 16, 26).
Shortcomings of this study include uncertainty in the ability of fractional Er:YAG laser to deliver a sufficient amount of clobetasol ointment to obtain an optimal therapeutic effect. While statistically significant differences attributable to steroid treatment were observed between experimental groups at 3-month follow-up, the application of fractional lasers as a drug delivery pathway requires optimal treatment parameters to achieve the ideal balance of fluence, treatment density, healing time and adverse effects. In FLADD, optimal drug concentration, drug vehicle, application time and duration remain inconclusive (12, 27). While the intent of this study was not to limit the participants to a single sex, all recruited subjects were female. This may reflect differential sex-based social pressures leading to scar revision on the abdominal wall. However, there is currently no reason to suggest that sex plays a role in hypertrophic scarring or response to laser treatment.
Previous in vitro trials documented that fractional laser pretreatment enhanced drug penetration, including both lipophilic and hydrophilic drugs with low molecular mass (< 500 Da) (12, 28). Clobetasol propionate, the agent used in the current study, is a lipophilic molecule with a molecular weight (MW) of 467 Da, consistent with the parameters used in prior in vitro FLADD trials (22, 23, 25, 29). As maximum medication uptake occurs within the first 30 min of laser exposure, the current study applied steroid treatment immediately after laser irradiation (30). Since previous studies demonstrated that once the stratum corneum is disrupted there is no further benefit to creating deeper ablative columns (31, 32), we used a fractional Er:YAG laser with fluence of 28 J/cm2 and pulse widths of 300 µs, creating a mean vaporization depth of 80 µm and mean coagulation depth of 150 µm (33).
In addition, the efficacy of other methods for facilitating the diffusion of drugs through fractional laser-induced micropores remain untested. While this study relies on manual hand massaging to increase drug diffusion, acoustic pressure ultrasound is emerging as a promising and more efficacious alternative (34–36). Further randomized controlled trials are recommended to determine the optimum conditions for the transcutaneous delivery of corticosteroids in the treatment of HTS, such as the density and depth of microscopic ablation zones (MAZs), the formulation of the drug being delivered, etc.
In summary, the current study found no long-term clinical benefit of applying topical clobetasol ointment immediately after fractional Er:YAG laser treatment for HTSs. However, steroid treatment in combination with monotherapy may significantly improve the short-term appearance of hypertrophic scars within 3 months of follow-up. While FLADD is increasingly applied to clinical practice as a means of enhancing medication uptake through the skin and improving treatment of cutaneous disorders, additional trials are warranted to prove its safety and efficacy over the existing fractional laser monotherapy.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize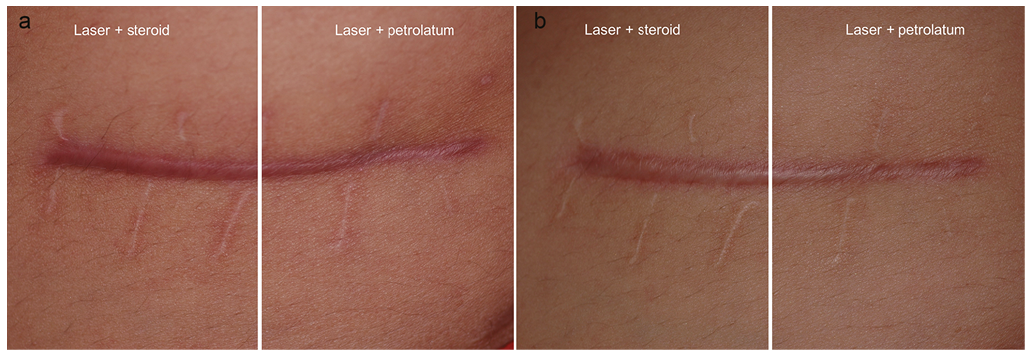 Click to show fullsize
Click to show fullsize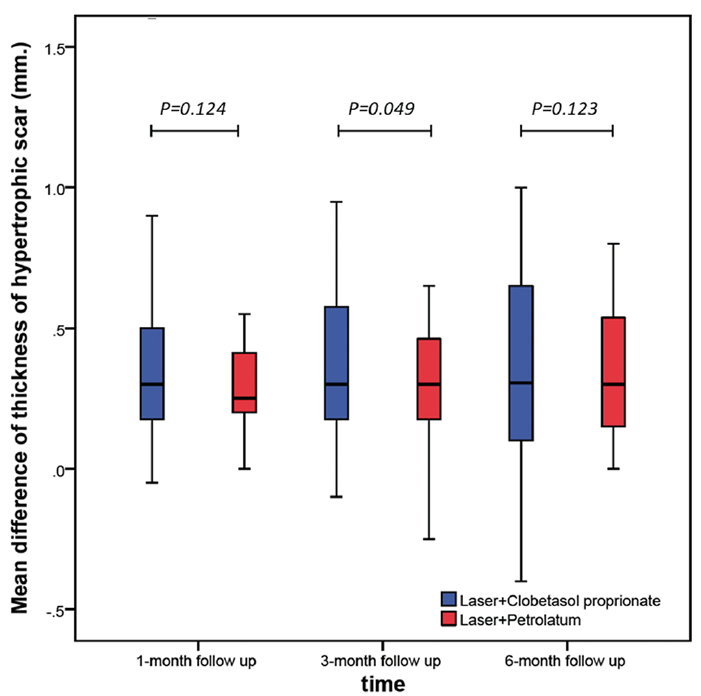 Click to show fullsize
Click to show fullsize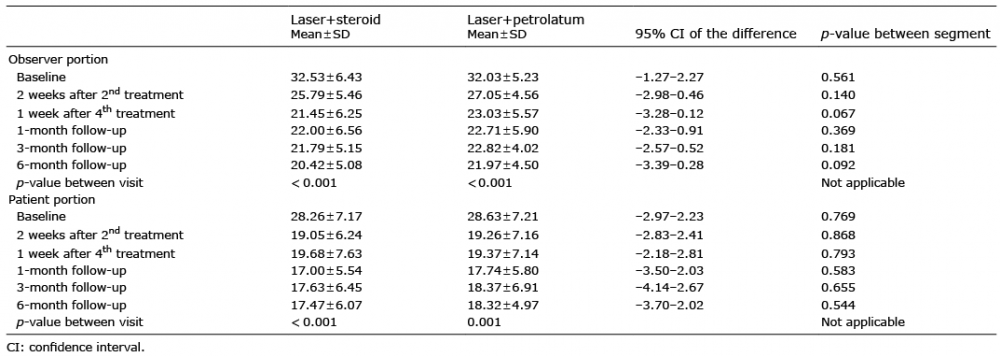 Click to show fullsize
Click to show fullsize