


1Department of Research, Cancer Registry of Norway, Institute of Population-based Cancer Research, 2Department of Dermatology, Oslo University Hospital – Rikshospitalet, Oslo, 3Department of Plastic Surgery and Burns, Haukeland University Hospital, Bergen and 4Department of Biostatistics, Institute of Basic Medical Sciences, University of Oslo, Oslo, Norway
In Norway, nodular melanoma is the most fatal melanoma subtype and superficial spreading melanoma the most common, indicating diagnostic challenges. The aim of this study was to assess the clinical suspicion sensitivity of nodular melanoma and superficial spreading melanoma, by diagnosing physician, using randomly selected 100 nodular melanomas and 100 superficial spreading melanomas from the Norwegian Melanoma Registry, diagnosed in 2014 to 2015. Information about suggested diagnoses and diagnosing physician was collected from pathology request forms. Suspicion sensitivity was defined as the proportion (%) of cases with “melanoma” as a suggested diagnosis, estimated with 95% confidence interval (95% CI). Most melanomas (74.5%) were diagnosed by non-dermatologists, with a suspicion sensitivity of 23% (95% CI 15–34) for nodular melanoma and 24% (95% CI 16–35) for superficial spreading melanoma. Corresponding estimates for dermatologists were 50% (95% CI 32–68) and 96% (95% CI 80–99), respectively (pinteraction=0.007). The low suspicion sensitivity for both subtypes among non-dermatologists calls for educational efforts.
Key words: melanoma; nodular melanoma; superficial spreading melanoma; suspicion sensitivity; population-based data.
Accepted Feb 25, 2021; Epub ahead of print Mar 9, 2021
Acta Derm Venereol 2021; 101: adv00427.
doi: 10.2340/00015555-3782
Corr: Trude E. Robsahm, Cancer Registry of Norway, Institute of Population-based Cancer Research, PO Box 5313 Majorstuen, NO-0304 Norway. E-mail: trude.eid.robsahm@kreftregisteret.no
In a population-based material of 100 superficial spreading melanoma and 100 nodular melanoma, similarly low clinical suspicion sensitivity was found for nodular melanoma (30%) and superficial spreading melanoma (42%). When separating by diagnosing physician, the suspicion sensitivity among non-dermatologists was found to be less than 25% for both melanoma subtypes, which calls for educational efforts. Among dermatologists, sensitivity for superficial spreading melanoma was high (96%) and lower for nodular melanoma (50%), emphasizing the challenge of recognizing nodular melanoma.
Norwegian mortality rates of cutaneous melanoma are the highest in Europe and are expected to increase (1). Recently, we found that Norwegian patients were diagnosed at more advanced stages than patients in other population-based registries (2), indicating a diagnostic delay. Furthermore, the proportion of nodular melanoma (NM) was high compared with superficial spreading melanoma (SSM), both in the incident and fatal Norwegian cases.
The ABCD mnemonic (Asymmetry, Border irregularity, Colour variation, Diameter > 6 mm) was introduced to educate physicians to recognize melanoma in its early clinical presentation (3). Evolution of lesions was recognized as a key sign, in particular for NMs, and the “E” for evolving was added later (4). The ABCDE criteria effectively educate about key signs of early melanoma (5) and cover the signs of SSM, the most common melanoma subtype, while NM, the second most common subtype, may fail to fulfil these diagnostic criteria (6). To our knowledge, only one study has assessed the sensitivity for diagnosis of melanoma according to melanoma subtype. The study concluded that NM is among the subtypes that are particularly difficult to diagnose (7). Furthermore, dermatologists have been found to better clinically recognize melanomas, in general, than non-dermatologists (8).
Due to the structure of the healthcare system in Norway, most melanomas are diagnosed by general practitioners (GPs). The high Norwegian rate of melanoma mortality and high proportion of NMs may reflect diagnostic challenges. Thus, the aims of this study were to examine the clinical suspicion sensitivity for NM and SSM, in general, and by diagnosing physician, and to examine the suggested diagnoses given for these subtypes.
The Cancer Registry of Norway (CRN) has recorded all cancer diagnoses in Norway since 1953, and holds complete and high-quality data (9, 10). In 2008, the Melanoma Registry (MR) was established under the CRN, with additional clinical and histopathological information for each case of melanoma.
A total of 100 NMs and 100 SSMs, diagnosed in 2014 to 2015, were selected randomly from the MR. After year 2000, 99% of melanoma cases diagnosed in Norway have been morphologically verified (9, 10), and the corresponding number for the current sample is 100%. The following data were collected: age at diagnosis (categorized as < 65 and ≥ 65 years); anatomical site of the primary tumour according to the International Classification of Diseases for Oncology, Third Edition (11) (categorized as head/neck (190.0), trunk (190.1/190.7), upper extremity (190.2), lower extremity (190.3/190.4) and unspecified (190.9)); Breslow thickness (categorized as T1: ≤ 1.0, T2: > 1.0–2.0, T3: > 2.0–4.0 and T4: > 4.0 mm (12)); and ulceration (categorized as present and not present). Because Norwegian pathologists have tended to report on ulceration only when it is present and not when absent (2), unspecified cases (n = 15) were categorized as not present.
From the pathology request forms, information about lesion colour was extracted and categorized with regard to amelanosis: yes (described as non-pigmented), no (described as pigmented) or unspecified (no information about colour). Furthermore, data about all suggested diagnoses were extracted. Diagnoses suggested < 5 times in total were categorized as “other”. Pathology request forms are non-standardized in Norway (13), information usually being automatically imported from anamneses/history. However, all include fields for date and location of lesion, and an open field for clinical description. The physician who performed the diagnostic tissue excision (the diagnosing physician), was categorized as non-dermatologist (GP, surgeon, other) or dermatologist.
Use and reporting of de-identified data from the MR and the pathology request forms is covered by the CRN’s regulations of collection and treatment of health information, and no further ethics approval was needed.
Statistical analyses
Clinical suspicion sensitivity was defined as the proportion of cases in which “melanoma” was a suggested diagnosis, regardless of its order. Power calculation was based on the Australian study, which is, to our knowledge, the only available study (p1 = 0.77 and p2 = 0.41 for NM and SSM, respectively) (7). With significance level 5% and power 90%, at least 38 patients per melanoma subtype are necessary to detect the same difference. Australian physicians diagnose more skin cancer than Norwegian physicians, hence the 2 proportions are probably lower in Norway, but we have no knowledge of whether to expect a larger or smaller difference between the 2 subtypes (e.g. p1= 0.67 and p2= 0.31 give a similar group size). To facilitate logistic regression analysis, it was decided to include 100 patients in each group. A logistic regression model can contain up to m/10 parameters, where m is the frequency of the least frequent outcome (14). With a total of 200 patients and 77+41=118 events (p1 = 0.77 and p2 = 0.41), up to 8 parameters (min(118, 82)/10=8.2) can be included in the multivariable model.
Suspicion sensitivity was calculated separately for NM and SSM and by diagnosing physician category, with 95% Wilson confidence intervals (95% CIs) (15). Logistic regression was used to study differences in suspicion sensitivity between NM and SSM in general, and by the diagnosing physicians. The study tested for interaction between sensitivity and diagnosing physician and between sensitivity and each of the clinopathological variables (sex, age at diagnosis, anatomical site, T category, ulceration and amelanosis). All p-values are 2-sided and a 5% level of significance was used. Stata, version 15 was used in all analyses.
The proportions of males and females were similar in the NM and SSM samples, while higher proportions of subjects age ≥ 65 years, head/neck site and ulceration were observed in NMs (Table I). Median Breslow thickness was 3.0 in NMs and 0.8 in SSMs. Amelanosis was described in 8 NMs and 1 SSM, although colour was unspecified in 61% of NMs and 50% of SSMs. Both NMs (74%) and SSMs (75%) were most often diagnosed by non-dermatologists (54% and 53% by GPs (who usually not use dermatoscope), respectively.
Table I. Characteristics of the nodular melanoma (NM) and superficial spreading melanoma (SSM) study samples
For 155 cases, only one diagnosis was suggested, while for 45 cases 2 (n = 38) or several (n = 7) diagnoses were suggested. Melanoma was the single suggested diagnosis in 15 of the NMs and 31 of the SSMs, and was suggested along with another diagnosis in 15 and 11 patients, respectively (Table II). Naevus was the dominant non-melanoma diagnosis suggested (29/108 for NM and 58/73 for SSM). All other non-melanoma diagnoses were more frequently suggested for NM than for SSM.
Table II. Melanoma diagnosis and non-melanoma diagnoses from the pathology request forms in the nodular melanoma (NM) and superficial spreading melanoma (SSM) study samples
Clinical suspicion sensitivity was lower for NM (30%, 95% CI 22–40) than for SSM (42%, 95% CI 33–52), although not significantly lower (p = 0.08) (Fig. 1). However, the sensitivity for NM and SSM varied by physician category (pinteraction = 0.007). Non-dermatologists had low sensitivity for both NM 23% (95%, CI 15–34) and SSM (24%, 95% CI 16–35) (p = 0.88) (Fig. 1). In dermatologists, the sensitivity for NM (50%, 95% CI 32–68) was significantly lower than for SSM (96%, 95% CI 80–99) (p = 0.004). No significant interactions were found between suspicion sensitivity and sex, age at diagnosis, anatomical site, T category, ulceration or amelanosis (0.24 ≤ pinteraction ≤ 0.91).
Fig. 1. Clinical suspicion sensitivity (%) with 95% confidence interval (95% CI) for nodular melanoma (NM) and superficial spreading melanoma (SSM) in general and by the diagnosing physician.
This first population-based study, examining clinical suspicion sensitivity of the melanomas histopathologically verified as NM and SSM, found low sensitivity for both subtypes, and, in particular, when diagnosed by non-dermatologists. Dermatologists had high sensitivity for SSM, but misdiagnosed half of the NMs.
A hospital-based Australian study, found higher diagnostic sensitivity than the current study, both for NM (41%, n = 121) and SSM (77%, n = 111) (7). They included in situ lesions (6%) and excluded pathology request forms with blank field of diagnosis (24%), which increased their diagnostic sensitivity, and dermatologists diagnosed a higher proportion of the melanomas. Moreover, the tumours were thicker than in the current study, indicating a selected patient group, as population-based Australian data show thinner melanomas at diagnosis (16) compared with Norwegian patients (2).
Low sensitivity for NM was expected in the current study, but there was a surprisingly low sensitivity for SSM among non-dermatologists. In contrast to the current results, the Australian study found a high diagnostic sensitivity for SSM among both dermatologists and non-dermatologists (82% and 78%, respectively) (7). Australian non-dermatologists and dermatologists diagnose and treat a large volume of all types of skin cancer, and this may explain the high sensitivity in both groups of physicians (17). The clinical suspicion sensitivity for NM among Norwegian dermatologists (50%) was in line with the result from the Australian study (57%), emphasizing the challenges in diagnosing NM. The Australian study also found amelanosis to be more frequent in NM than in SSM and it was significantly associated with misdiagnosis (amelanosis was assessed by patient interviews) (7). In the current study, the tumour was categorized as amelanotic only if specified as “non-pigmented” in the pathology request form, but the majority did not specify this. The high proportion of notifications without specification about colour in the current study data may indicate low attention to this factor (18). Diagnoses usually being non-pigmented (i.e. basal cell carcinoma, pyogenic granuloma, squamous cell carcinoma and haemangioma) were more often suggested in NMs, indicating more varying appearance and more amelanosis in NM. Correspondingly, naevus was suggested for a higher proportion of SSM than of NM.
An important strength of the current study is the random selection of NMs and SSMs from a high-quality population-based register. It is a weakness that the study design allowed only for estimation of diagnostic sensitivity, not accuracy including false-positives. Furthermore, we had no information about number of doctor visits prior to the resection or the physicians’ experience in diagnosing melanoma, and thus the data was not suited for examining detection delay. The current study sample size is comparable to that of Lin et al. (7), and should be sufficient for the logistic regression analyses, in which up to 3 independent variables were included in each model. Tests for interaction usually have low power, thus the absence of strong evidence that interaction was present does not imply that interaction was absent (19).
There has been a disproportionate focus on the ABCD guideline in early melanoma diagnosis. Since NM is a major contributor to melanoma death (2, 20), focus on melanoma signs should include the characteristics of NM (EFG: elevated, firm, growing) (18). The low suspicion sensitivity found for both melanoma subtypes among non-dermatologists, the main melanoma-diagnosticians in Norway, calls for educational efforts, whereof teledermatology may be a guiding support.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize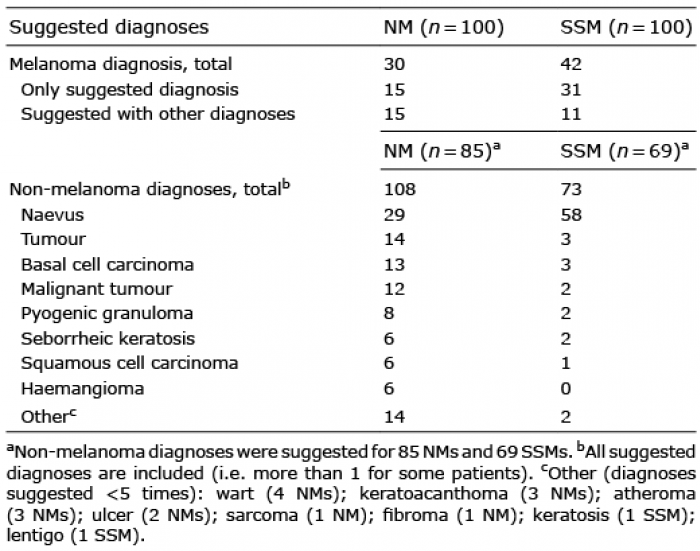 Click to show fullsize
Click to show fullsize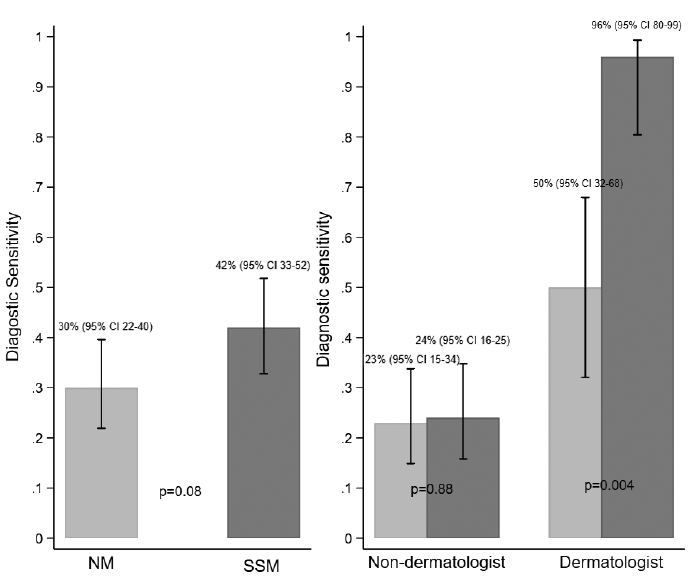 Click to show fullsize
Click to show fullsize