


1Department of Dermatology, and 2Department of Hematology, Hospital del Mar – Institut Mar d’Investigacions Mèdiques, Universitat Autònoma de Barcelona (UAB), Barcelona, Spain. *E-mail: 93702@parcdesalutmar.cat
Accepted Mar 10, 2021; Epub ahead of print Mar 16, 2021
Acta Derm Venereol 2021; 101: adv00418.
doi: 10.2340/00015555-3783
The phosphatidylinositol 3-kinase (PI3K)/protein kinase B (AKT)/mammalian target of rapamycin (mTOR) signalling pathway is one of the most frequently deregulated signalling pathways in malignant tumours (1). Likewise, the PI3K/mTOR pathway regulates both the innate and the adaptive immune response (2). Preclinical and clinical evidence have supported the principle of targeting this pathway, leading to the development of several inhibitors for the treatment of cancer.
We report here a patient under treatment with a PI3K-delta inhibitor, who presented a psoriasiform skin eruption. The rationale of PI3K inhibition is beneficial for psoriasis (2, 3) and observation of this unusual adverse event is probably a new example of an unexpected paradoxical psoriasiform reaction.
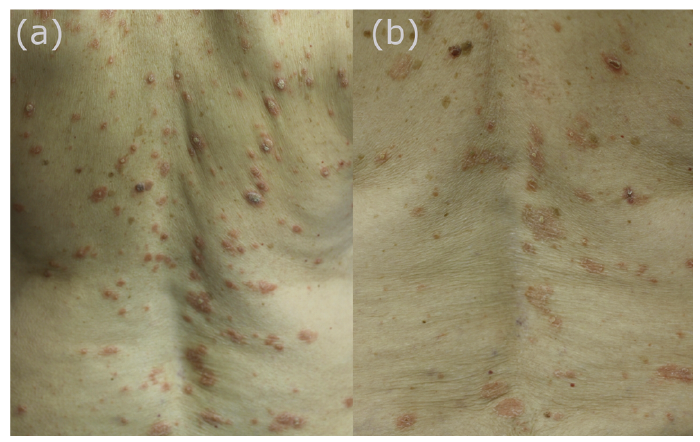
A 71-year-old woman was diagnosed with mantle cell lymphoma (stage IVB) in 2016 and treated with different chemotherapy regimens. Initially, 6 cycles of rituximab, cyclophosphamide, doxorubicin, vincristine and prednisolone (R-CHOP) were given, but, due to suboptimal response, 6 cycles of rituximab, gemcitabine and oxaliplatin (R-GemOx) were subsequently administered, followed by bimonthly rituximab maintenance in monotherapy for 2 years. The patient presented a relapse in 2019, and was then enrolled in a clinical trial to receive a PI3K-delta inhibitor. One year after initiation of this therapy, the patient presented a progressive eruption, involving her scalp, trunk and arms, of non-confluent scaly erythematous papules and plaques 0.4–2 cm in diameter (Fig. 1a). There were no other apparent triggers for the eruption or any personal or family history of psoriasis. A skin biopsy disclosed confluent parakeratosis, regular acanthosis and hypogranulosis (Fig. 2). PI3-K delta inhibitor treatment was maintained. The patient was initially on 2.5 mg/day, but after the rash, the dose was lowered to 1 mg/day. Treatment with topical corticosteroids, emollients and oral anti-histamines (triamcinolone acetonide 0.1%, and ebastine 10 mg/day) was started and, within 2 weeks, the symptoms almost cleared with only mild erythematous plaques remaining on the trunk (Fig. 1b).
Fig. 1. Clinical photographs. (a) Clinical presentation characterized by non-confluent scaly erythematous papules and plaques, 0.4–2.0 cm diameter, 1 year after initiation of PI3K-delta inhibitor therapy. (b) Close-up of the medial part of the back, showing an improvement with only some mild plaques remaining after further treatment, as described.
Fig. 2. Haematoxylin/eosin skin biopsy, revealing confluent parakeratosis, regular acanthosis, hypogranulosis, suprapapillary thinning of the epidermis and perivascular lymphocytes in the papillary dermis. Haematoxylin/eosin × 120.
The past few years have seen increasing interest in the development of PI3K-delta inhibitors, such as idelalisib and copanlisib, which have been approved for refractory follicular lymphoma and chronic lymphocytic leukaemia (4). Well-recognized side-effects of PI3K inhibitors include different infectious disorders, autoimmune diseases, neutropaenia and cutaneous reactions (4).
Cutaneous reactions to PI3K inhibitors include mild maculopapular eruptions, pruritus, and dry skin. The onset of skin eruptions is typically within the first weeks or months of treatment. Isolated cases of severe hypersensitivity reactions, erythema multiforme and toxic epidermal necrolysis have also been described (4).
We report here a patient treated with a PI3K-delta inhibitor who presented with a cutaneous eruption that was clinically and histopathologically indistinguishable from psoriasis. The eruption cleared with PI3K inhibitor dosage reduction and topical treatment. Development of such psoriasiform eruptions have rarely been reported in patients treated with PI3K-delta inhibitors (5, 6) (Table I).
Table I. Reports of psoriasiform eruptions in patients treated with phosphoinositide 3-kinases delta (PI3K-delta) inhibitors
The mechanisms leading to a psoriasiform inflammatory reaction with PI3K inhibitors are unknown. There is some evidence that PI3K/AKT signalling pathway is hyperactivated and involved in the early development of psoriatic lesions and later in an increase of Th1/Th17 responses, keratinocyte differentiation and angiogenesis (2). In fact, it has been hypothesized that PI3K inhibitors could be potential therapeutic drugs for psoriasis (2, 3) and a PI3K delta inhibitor (seletalisib) has already been evaluated in phase I studies (3). However, the PI3K pathway is also known to downregulate inflammatory cytokine responses, thus promoting the transcription of interleukin (IL)-12 and repressing the anti-inflammatory IL-10 (7). Interestingly, a paradoxical inhibition of IL-10 production by PI3K inhibitors has been reported (7). Cytokine arrays have revealed upregulation of IL-6 in PI3K inhibitor copanlisib- and duvelisib-resistant cell lines, leading to downregulation of phosphorylated (p) STAT5, AKT, mitogen-activated protein kinase, p-STAT3 and nuclear factor-κB (8). Both previous findings may also contribute to the understanding of the different mechanisms behind paradoxical psoriasiform reactions due to PI3K inhibition.
We conclude that it is possible that these cases of psoriasiform eruptions induced by PI3K-delta inhibitors are an additional example of drug-induced paradoxical psoriasiform skin reaction. These observations appear to expand the spectrum of paradoxical psoriasiform reactions known to be induced with the extended use of biologics (mainly tumour necrosis factor-α inhibitors) (9). Increased awareness among dermatologists and onco-haematologists regarding these possible unexpected side-effects is important in order to improve the management of such patients and to avoid unnecessary discontinuation of treatments.
BS-G is a consultant and/or speaker bureau for Novartis, Amgen, Alexion, Gilead, Takeda and Shire. The other authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize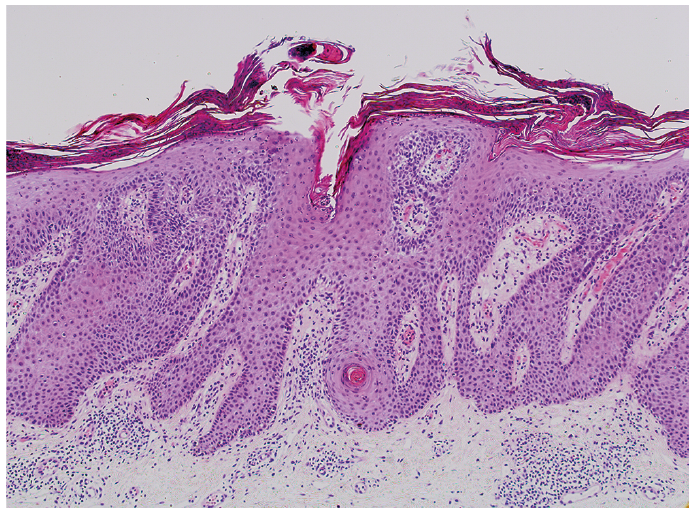 Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize