


1Department of Dermatology and Allergy, University Hospital, Ludwig Maximilian University Munich, Frauenlobstraße 9–11, DE-80337 Munich, Germany and 2Dr Phillip Frost Department of Dermatology and Cutaneous Surgery, Miller School of Medicine, University of Miami, Miami, FL, USA. *E-mail: markus.reinholz@med.uni-muenchen.de
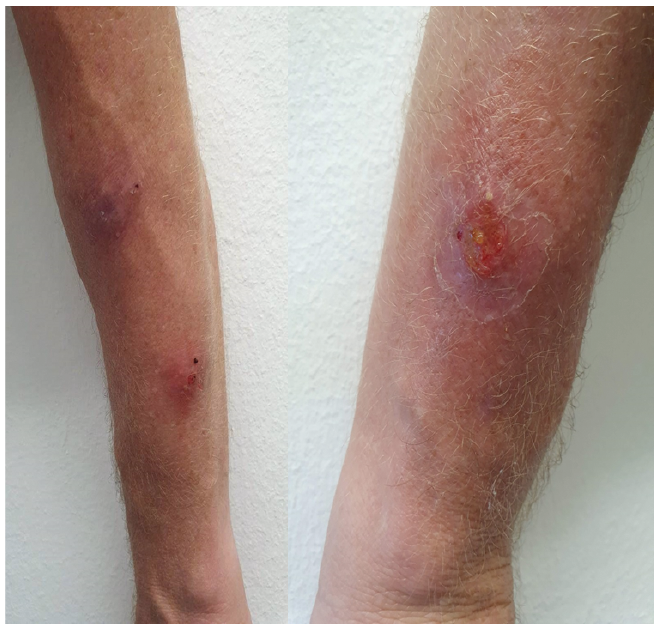
A 49-year-old Caucasian man presented to the dermatology department of Ludwig Maximilian University (LMU), Munich, Germany, with non-itchy, nodular lesions on his neck, arms and gluteus, which had persisted for over 10 years and intermittently healed spontaneously with scar formation (Fig. 1). He reported having had homosexual intercourse with changing partners in the last decade. The patient had been admitted in 2013 due to these lesions with a diagnosis of prurigo nodularis. Due to his recent holiday in Thailand and the distribution of the lesions on his forearms, a diagnosis of sporotrichosis was made by his general practitioner. He initiated a 7-day antibiotic treatment with amoxicillin/clavulanic acid (875 mg/125 mg) twice daily, with no clinical response.
On further detailed enquiry, the patient reported having been diagnosed with syphilis in 2013 by his general practitioner; however, the time of initial infection might have been in approximately year 2000.
What is your diagnosis? See next page for answer.
Fig. 1. Reddish-scaly nodules up to 4 cm in diameter with superficial ulceration, draining a putrid secretion on both forearms.
Acta Derm Venereol 2021; 101: adv00432.
Diagnosis: Gummatous syphilis and latent neurosyphilis
Clinical examination revealed isolated nuchal ulcerated plaques, nodules and scarification. Post-inflammatory hyperpigmented maculae were present on the gluteus. On both forearms, the patient had reddish-scaly nodules, up to 4 cm in diameter, with superficial ulceration, draining a putrid secretion, but no further lesions on the rest of his body.
Blood analysis revealed only slightly elevated levels of liver enzymes and a C-reactive protein (CRP) of 1.1 mg/dl (normal range: < 0.5 mg/dl). HIV serology was negative. A Treponema pallidum particle agglutination (TPPA) test was reactive (1:1280) and Treponema pallidum-IgG positive. Microbiological and mycological examinations of the lesions were negative. Culture for mycobacteria was negative.
Histology of a completely excised nodule from the forearm showed a plasma cell-rich, partially chronically fibrosing, mixed-cell dermatitis, possibly due to an intolerance reaction or infection. No acid-resistant rods were found. T. pallidum PCR from the FFPE material was negative (Fig. 2).
Transthoracic echocardiography showed no pathological findings.
Cerebrospinal fluid analysis found elevated levels of intrathecal T. pallidum antibody-index (ITpA-index): 7.62 (ref. 0.50–1.50), suggesting an acute or resolved neurosyphilis.
A diagnosis of a gummatous syphilis and latent neurosyphilis was made (stage IV syphilis).
Intravenous therapy with penicillin G (10 mio IU, 3 times daily) for 14 days was initiated. In advance, the patient received oral Jarisch–Herxheimer reaction prophylaxis with 100 mg prednisolone. The therapy resulted in an improvement in skin findings, followed by almost complete healing of the nodules with partial scarring (Fig. 3). Follow-up was scheduled every 3 months during the first year after ending the treatment.
To detect syphilis, the T. pallidum haemagglutination assay (TPHA) is used for screening. To monitor the course of disease and verify the success of treatment, the Venereal Disease Research Laboratory (VRDL) tests and the Rapid Plasma Reagin (RPR) tests should be used. T. pallidum-specific IgM antibodies might also be detected and can be used for follow-up after treatment (19S-immunoglobulin M-fluorescence-treponema-antibody-absorption-test, immunoglobulin M enzyme immuno assay, and IgM-immunoblot) (1).
If a late stage of infection is suspected, more comprehensive tests are indicated, such as cardiovascular and neurological examination, including cerebrospinal fluid analysis to exclude mesaortitis luetica and neurosyphilis.
This case report highlights the current relevance of a century-long known disease, and emphasizes the importance of identifying and treating the infection stage-appropriately.
The steadily increasing number of new infections and complicated disease course of syphilis highlights the continuing relevance of this disease. Approval of pre-exposure prophylaxis (PrEP) for HIV infection was granted by the US Food and Drug Administration (FDA) in 2012, and, with its increasing use worldwide, new challenges arise regarding the increase in other sexually transmitted infections (STIs), including syphilis. The rate of primary and secondary syphilis has increased compared to previous data up to 70%, with up to 58% of cases ocurring occurring in men who have sex with men (MSM) (2), emphasizing that syphilis is not just an “old companion”, but a very current one. On the other hand, quarterly screenings, which are recommended during use of PrEP, allow early diagnosis and therapy for STIs (3).
It is vital to raise awareness amongst medical practitioners regarding the importance of a comprehensive knowledge of syphilis and its varying clinical appearances. As this case report shows, a thorough patient history is essential, regarding not only the time of infection, but also the previously performed diagnostics and therapy. A diagnosis of syphilis should always lead to a sufficient, stage-appropriate therapy with consecutive follow-up.
Fig. 2. Histology of a completely excised nodule showing a chronically fibrosing dermatitis with a plasma cell and eosinophilic infiltration. Hematoxyllin eosin staining: left 4x, right 10x.
Fig. 3. Almost complete, partially scarred, healing of the nodules on the forearms after antibiotic therapy.


 Click to show fullsize
Click to show fullsize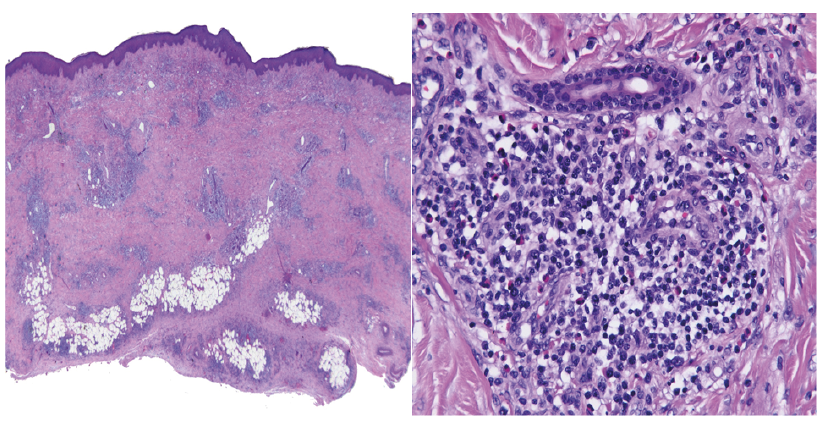 Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize