


Departments of 1Dermatology and 4Pathology, Instituto Valenciano de Oncología, ES-46009 Valencia, Departments of Dermatology, 2Hospital Universitario Virgen de la Macarena, Seville and 3Hospital Universitario Miguel Servet, Zaragoza, Spain. E-mail: elisariosvi@hotmail.com
Accepted Mar 17, 2021; Epub ahead of print Mar 18, 2021
Acta Derm Venereol 2021; 101: adv00429.
doi: 10.2340/00015555-3791
Conventional chemotherapy agents commonly cause infusion-site lesions, such as chemical cellulitis due to drug extravasation and evanescent eruptions (1–7). One of the most characteristic (although perhaps little-known) local cutaneous adverse reactions to chemotherapy is the so-called localized epidermal necrolysis (EN) at the infusion site (8). This reaction has also been described as persistent erythema multiforme (EM)-like eruption (8), fixed drug eruption (FDE) (9), fixed erythrodysaesthesia plaque (10), and persistent serpentine supravenous hyperpigmentation/eruption (PSE) (8, 11–14). Although localized EN was initially regarded as a hypersensitivity reaction, subsequent reports have confirmed its cytotoxic nature (8, 9, 12).
The classification of cytotoxic chemotherapy-related skin reactions has been historically confusing (1, 3–5), until the introduction of the term “toxic erythema of chemotherapy” (TEC): a unifying terminology that includes overlapping clinical entities characterized by skin lesions associated with chemotherapy cytotoxicity (1). However, localized EN has not yet been studied in depth in the literature. In order to better characterize this entity, a review was carried out of all cases of localized EN evaluated in the Department of Dermatology of Fundación Instituto Valenciano de Oncología and a thorough literature search performed. A simplified nomenclature is proposed for this reaction, including it within the TEC spectrum.
A retrospective observational study of 45 patients was performed, all of whom were diagnosed with injection-site lesions consistent with localized EN at Instituto Valenciano de Oncología in Valencia, Spain between 1998 and 2019. Descriptive statistical analysis was performed using IBM-SPSS 25.0. A systematic review of the available literature was conducted in the PubMed Meta Search Engine, identifying a total of 34 cases. Publications including cases with an unclear aetiology or with a definition that did not correspond to the features of localized EN were discarded. The study was approved by the ethics committee of the Department of Dermatology of Fundación Instituto Valenciano de Oncología, and all patients provided informed consent.
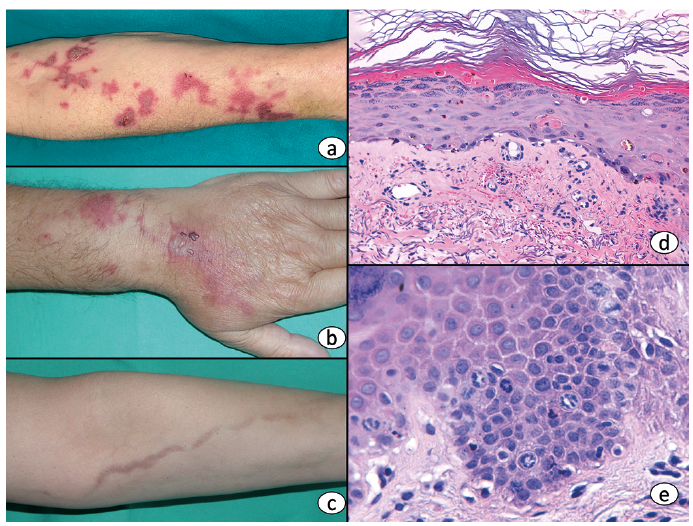
All cases developed skin lesions overlying the infusion vein, which appeared without previous drug extravasation or chemical phlebitis. They were associated with itching and tenderness on palpation. All cases could consistently be classified into 3 distinct clinical patterns: (i) EM-like lesions, consisting of erythematosus, oedematous macules. These symptoms have previously been described in the literature as localized EN or EM-like lesions (8); (ii) FDE-like lesions, consisting of 1 or 2 inflammatory plaques at the infusion site, sometimes with an associated blister. Similar lesions have previously been described as chemotherapy-related FDE (10); (iii) PSE, consisting of erythematosus, scaly macules, that resolve leaving a characteristic post-inflammatory linear hyperpigmentation (Fig. 1). These lesions have previously been described as persistent supravenous erythema or persistent serpentine supravenous erythematous eruption (acute), and serpentine supravenous hyperpigmentation (chronic) (11–15).
Fig. 1. Clinical features and histological features. (a) Erythema multiforme (EM)-like presentation: erythematous macules and papules with vesicular changes, following a linear path along the affected vein. (b) Fixed drug eruption (FDE)-like presentation: localized erythematous, inflammatory plaques at the infusion site, also showing vesicular changes. (c) Persistent serpentine supravenous hyperpigmentation/eruption presentation: non-inflammatory, linear hyperpigmentation following the infusion vein. (d) Mild interface dermatitis with basal vacuolar degeneration, and scattered necrotic keratinocytes (haematoxylin-eosin, 200× original magnification). (e) Mitotic retention figures scattered in supra-basal layers (haematoxylin-eosin, 400× original magnification).
The most common clinical presentation in the series described here was an EM-like eruption (n = 18, 40%), followed by PSE (n = 14, 31% of cases). However, PSE was the most frequently reported presentation in the literature (n = 17, 50%), followed by FDE (n = 11, 32%). Vinca alkaloids and taxanes were the most common culprit drugs in our series (14 and 15 cases, respectively). Continuous 5-fluoruracil (5-FU) infusion was mainly associated with both acute and chronic PSE (6 out of 7 cases). In the literature, taxanes were the most frequently reported culprit drug (9 cases), followed by vinca alkaloids and 5-FU (5 cases each). Three of the cases associated with 5-FU were clinically compatible with PSE. The patients in our series developed lesions after a median of 3 treatment cycles, and 5 patients developed them after the first cycle. The skin reaction appeared within 24–96 h of the infusion session and healed after several weeks, sometimes leaving post-inflammatory hyperpigmentation. The patients described in the literature developed lesions within 1–7 days of drug administration. All the localized EN lesions occurred at the injection site, and the most common location in our series was the forearm (n = 21, 47%). Interestingly, one patient developed a lesion on the chest, secondary to infusion through a central venous line. Recurrences were reported in 16% (n = 7) of patients.
A skin biopsy was performed in 12 of the patients. The histological findings for all 3 clinical patterns were similar to those described for the general spectrum of chemotherapy-related epidermal cytotoxicity: interface dermatitis, hydropic degeneration of the basal layer, alterations in keratinocyte maturation and keratinocyte necrosis of varying degrees (Fig. 1). Eccrine squamous syringometaplasia was observed in 4 cases. The clinical and histological features are summarized in Tables SI and SII, while literature cases are depicted in Table SIII.
Since it was first described, localized EN has been referred to by varying terms, rendering its identification challenging (8–10, 12). Although initial agreement on the pathogenesis of this eruption was lacking, it now seems clear that it represents a cytotoxic reaction (8, 12–14). The findings of the current study further support this pathogenic mechanism, since the lesions appeared without prior sensitization in 5 cases, did not always reappear in successive treatments, and had histopathological features of direct epidermal cytotoxicity. Thus, localized EN shares clinical and histological features with other cytotoxic reactions regarded as TEC, and we believe that this entity should also be included in the TEC spectrum. We propose using the term “localized injection-site TEC” to designate localized EN and its 3 main clinical variants (EM-like lesions, FDE-like lesions, and PSE).
Despite the scarcity of available data, a thorough literature review suggests that localized injection-site TEC is a relatively common chemotherapy-related reaction (8–10, 13, 15). The true incidence of localized injection-site TEC is unknown. An increase in cases was observed several years ago with the widespread introduction of drugs such as docetaxel and vinorelbine in oncological practice, but the increasing use of central venous lines in more recent years has probably led to a reduction in cases.
The results of this study show that localized injection-site TEC lesions are much more likely to appear when small distal vessels are used for chemotherapy infusion, where part of the infused chemotherapeutic drug could potentially pass through the vascular endothelium and reach high concentrations in the overlying skin, exerting its cytotoxic effect. This hypothesis is supported by the fact that local skin reactions are very rare when large vessels (central lines) are used for infusion (3). In the current series, only one patient developed localized injection-site TEC after the administration of chemotherapy through a central line.
The differential diagnosis of localized injection-site TEC should include other infusion-site lesions, such as doxorubicin-related evanescent supravenous erythema and extravasation reactions (3). Localized injection-site TEC characteristically occurs after an uneventful chemotherapy session and resolves over a few weeks (8, 9, 11, 13, 14). Changes to the frequency of drug injection or the use of Y-type administration sets could prevent the reappearance of lesions in subsequent cycles (3).
The erratic historical characterization of localized injection-site TEC has rendered its identification as a cytotoxic reaction to chemotherapy difficult, as was previously the case for many chemotherapy-related skin reactions. In our opinion, referring to this entity as “localized injection-site TEC” would further contribute to standardization of the description of chemotherapy cutaneous adverse effects and facilitate its recognition and management by clinicians.
In conclusion, localized injection-site TEC is a direct injection-site cytotoxicity phenomenon caused by chemotherapy, probably resulting from high concentrations of the cytostatic drug in the infusion vein. The most common associated drugs are vinca alkaloids, taxanes and 5-FU. Although its incidence has probably declined due to increased use of central venous lines, localized injection-site TEC is a characteristic skin reaction to chemotherapy that requires correct identification and management.


 Click to show fullsize
Click to show fullsize