


Department of Dermatology, Kagoshima University Graduate School of Medical and Dental Sciences, 8-35-1 Sakuragaoka, Kagoshima 890-8520, Japan. E-mail: kazfujii@m2.kufm.kagoshima-u.ac.jp
Accepted Mar 17, 2021; Epub ahead of print Mar 18, 2021
Acta Derm Venereol 2021; 101: adv00436.
doi: 10.2340/00015555-3792
Microcystic adnexal carcinoma (MAC) commonly manifests as a solitary plaque located on the face, including the upper or lower lips (1). This neoplasm is locally aggressive with deep infiltration and is characterized by frequent recurrence. Pathologically, MAC displays both eccrine and follicular differentiation, and is thought to originate from pluripotent adnexal keratinocytes. The superficial lesion is composed of numerous keratinous cysts, and small islands or cords of basaloid and squamous epithelium with ductal differentiation. The deeper part of the tumour consists of small nests and strands of cells. Those components are surrounded by a dense collagenous stroma (2).
An 85-year-old Japanese woman was referred to our clinic with a 10-year history of slowly progressing yellowish and firm nodule and plaques (up to 1.5 cm) on her left mandible (Fig. 1). The lesions were asymptomatic and irregularly distributed. No lesions were observed on her oral mucosa and her cervical lymph nodes were not palpable. Yellowish xanthomatous lesions were seen only on the mandible, and no xanthomatous lesions were observed on other skin areas. Histopathological examination of the central and largest nodule revealed a relatively well-circumscribed neoplastic lesion with keratin-filled cysts and keratinizing nests and cords of epithelial cells in the superficial dermis, duct-like structures, and clear cells resembling sebaceous cells in the deep dermis (Fig. 2a–c). All histopathological features were suggestive of MAC. Further analysis revealed that many foamy cells infiltrated the superficial dermis and admixed with keratinizing nests (Fig. 1b, d). Perineural invasion was not observed. The epithelial cells were positive for cytokeratin AE1/AE3 and negative for the epithelial cell adhesion molecule Ber-EP4, the carcinoembryonic antigen (CEA), and epithelial membrane antigen (EMA), whereas the foamy cells were positive for CD68 (Fig. 2e, f) and negative for AE1/AE3. Abundant small lymphocytes were also observed around the cords. Histological analysis of the yellowish plaque surrounding the central nodule also showed keratinizing nests and cords of epithelial cells with foamy cell infiltration beneath the epidermis. Levels of serum lipids, including triglycerides, and total and low-density lipoprotein (LDL) cholesterol, were within normal limits. Chest radiography and computerized tomography of the head and neck did not reveal any abnormalities. Hence, the diagnosis of MAC with xanthomatous inflammatory reaction was made. She underwent a wide local excision, but the tumour recurred locally without distant metastasis 6 months after the surgery. She lived with the disease for 1.5 years after her first visit.
Fig. 1. Clinical presentation. A yellowish tumour abutting on the lower lip with adjacent small and yellowish papules. Yellowish plaques surround the tumours.
Fig. 2. Histological findings. Histopathological analysis of a skin biopsy revealed (a: haematoxylin–eosin, ×12.5) a dense infiltration in the dermis (b: haematoxylin–eosin, ×100) with numerous keratinous cysts and follicular differentiation, and (c: haematoxylin–eosin, ×200) with cords of basaloid epithelium with ductal differentiation. In addition, infiltrations of foamy cells were observed (d: haematoxylin–eosin, ×200; f: CD68, ×200) admixed with the tumour cells and (e: CD68, ×200) under the epidermis.
Among its characteristic clinical and histopathological features, the patient had multiple skin lesions and xanthoma cell infiltrations. Xanthoma cells were identified within the reticular dermis, which might have contributed to the yellowish colour of the tumours, but also in the deep dermis admixed with epithelial cells. There was no direct proof that macrophages affected the tumour formation; however, it is very rare for xanthomatous lesions to be found only on the mandible, where MAC occurred. Therefore, it was reasonable to assume that MAC and xanthoma were causally related rather than that they randomly developed in the same area. Xanthoma cells are often associated with cancer after the administration of chemotherapy (3), but they are rarely observed in untreated cases, such as the patient studied. To date, MACs with xanthomatous infiltration have not been reported. Since the patient did not receive any chemotherapy and many inflammatory lymphocytes were observed within the tumour mass, xanthoma cell infiltration could be attributed to the inflammatory reaction of the host against the tumour cells. Lipid-laden macrophages, such as xanthoma cells, can release epithelial growth factors in metabolic disorders (4) and induce epidermal hyperplasia with eventual malignant transformation (5). Therefore, it is possible that xanthoma cells contributed to tumour growth. Given that these lesions existed for 10 years, we speculate that the prolonged presence of MAC cells induced inflammatory reactions, which, in turn, promoted xanthoma cell infiltration and further growth of this rare cancer.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize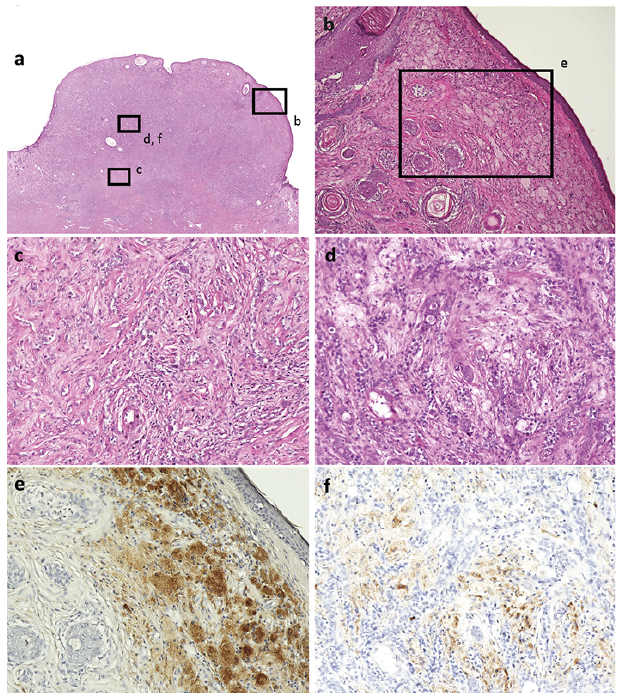 Click to show fullsize
Click to show fullsize