


1Department of Dermatology, Zealand University Hospital, Roskilde, 2Department of Clinical Medicine, University of Copenhagen, Copenhagen, 3Department of Dermatology and Allergy Centre, Odense University Hospital, 4Clinical Institute, University of Southern Denmark, Odense, 5Department of Dermatology and Allergy, Herlev and Gentofte Hospital, Copenhagen, 6Trial Nation, governmentally funded association advancing clinical trials in Denmark, 7Department of Dermatology, Aarhus University Hospital, Aarhus, 8Department of Dermatology, Bispebjerg Hospital, DK-2400 Copenhagen NV, and 9Department of Clinical Medicine and Department of Biomedical Sciences, University of Copenhagen, Copenhagen, Denmark. *E-mail: simonfrancisthomsen@gmail.com
#These author share senior authorship equally.
Accepted Apr 14, 2021; Epub ahead of print Apr 15, 2021
Acta Derm Venereol 2021; 101: adv00461.
doi: 10.2340/00015555-3800
Clinical trials are essential for the advancement of medical knowledge; they have revolutionized treatment options (1). Although the cost of conducting clinical trials has risen in recent years (2), they are considered the gold standard for advancing patient care. Patients who choose to participate may find the frequent study visits demanding, but they also benefit from participating in clinical trials. They often receive a higher degree of attention to symptoms. Patients are also provided access to new treatments not yet available to the general public, and in the process of trial participation, they often gain a deeper understanding of their disease (3, 4). In spite of such tangible benefits, recruitment to clinical trials often proves difficult.
Studies have reported patient recruitment to be less than half of the pre-specified number in clinical trials (5, 6). Consequences of poor patient recruitment include underpowered studies, which, in turn, may necessitate a costly extension of the trial (7). In addition, recruitment from specific patient groups or regions may prove difficult, potentially complicating the generalizability of the results of the trial (8). Successful recruitment of patients is therefore considered one of the most challenging aspects of conducting clinical trials (9).
To date, recruitment of patients for clinical trials has been based mainly on physicians’ spontaneous recruitment during routine work, e.g. in a busy clinical setting. Commercial patient recruitment programmes have also been initiated, but alternatives to this process are still needed to improve the selective recruitment processes in future clinical trials.
We report here the Trial Nation database, a nationwide database recently established to enhance recruitment to clinical trials in dermatology in Denmark. Trial Nation is a public-private partnership that provides a single, national entry point for life science companies, patient organizations and clinical researchers who wish to sponsor, participate in, or conduct clinical trials in Denmark (www.trialnation.dk; accessed 12 September 2020). The aim of the Trial Nation database is to create an easily accessible registry of patients who have expressed an a priori interest in clinical trials, i.e. a registry of potential volunteers for trial participation.
Dermatology patients are invited to join the volunteer database by a healthcare professional during routine visits to hospital. Those who decide to join the registry will receive an electronic informed consent form and questionnaire about their skin disease. Patients with psoriasis and atopic dermatitis have been included initially. Future initiatives include expanding recruitment to patients with other dermatological diseases.
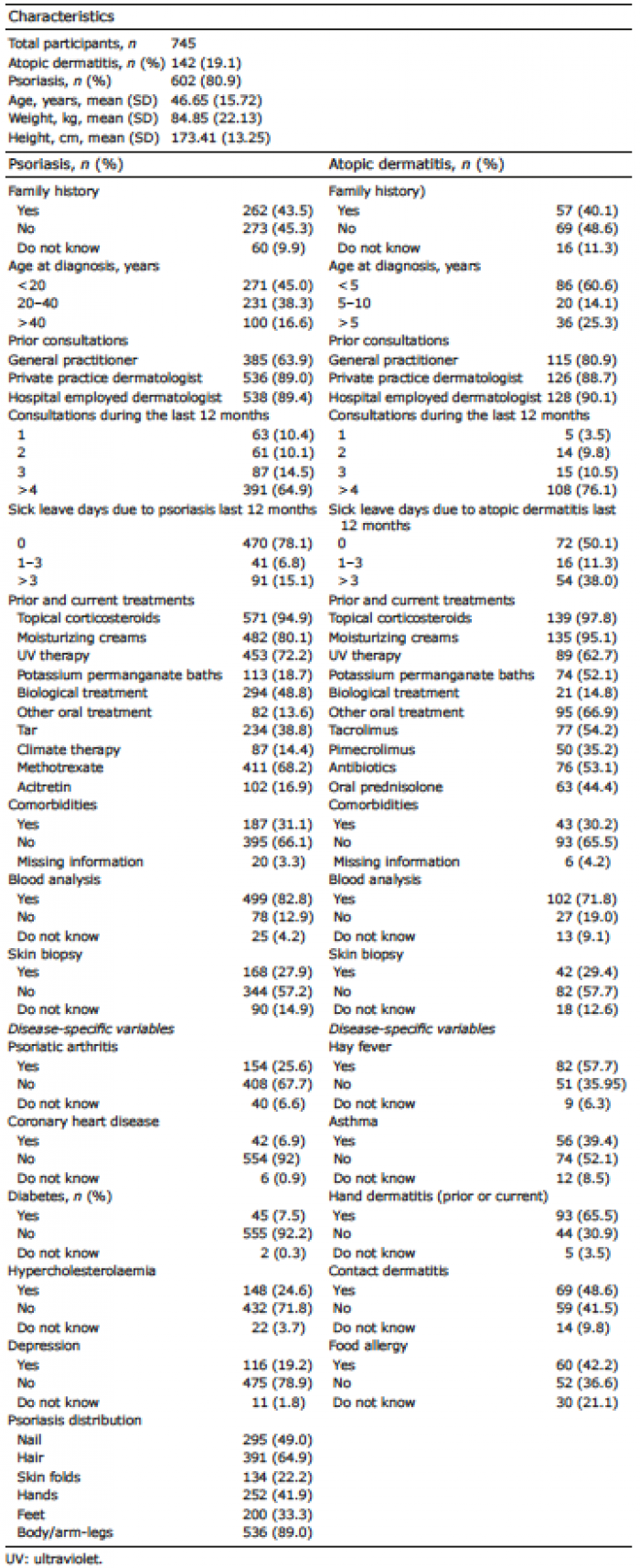
The questionnaire includes a selection of relevant variables reflecting selection criteria for prototypes of clinical trials on these indications. The demographics of the patients in the database are shown in Table I. The variables include disease distribution, current and prior treatments, and presence of relevant comorbidities (arthritis, asthma, diabetes, coronary heart disease and hypertension). Information regarding prior skin biopsies and blood analysis are also obtained.
Other technical solutions and alternative trial designs have been proposed, but several studies highlight the advantages of investing in maintaining and creating a cross-organizational and national recruitment database (10–13). The Trial Nation database includes an increasing number of potential research volunteers who can easily be contacted and contribute to the advancement of patient care and medical knowledge.
Table I. Demographics of patients in the Trial Nation database
The authors thank OPEN, Open Patient data Explorative Network, Odense University Hospital, Region of Southern Denmark.
Conflicts of interest: AB has been a speaker for LEO Pharma and Abbvie and involved in research with Shire/Takeda. LS has been a paid speaker for AbbVie, Eli Lilly, Novartis, and LEO Pharma, and has been a consultant or has served on Advisory Boards with AbbVie, Janssen Cilag, Novartis, Eli Lilly, LEO Pharma, UCB, Almirall, Bristol-Myers Squibb, and Sanofi. She has served as an investigator for AbbVie, Sanofi, Janssen Cilag, Boehringer Ingelheim, AstraZenica, Eli Lilly, Novartis, Regeneron, and LEO Pharma, and has received research and educational grants from Novartis, Sanofi, Bristol-Myers Squibb, Janssen Cilag, and LEO Pharma. LI served as a consultant and/or paid speaker for and/or participated in clinical trials sponsored by: AbbVie, Almirall, Amgen, Astra Zeneca, BMS, Boehringer Ingelheim, Celgene, Centocor, Eli Lilly, Janssen Cilag, Kyowa, Leo Pharma, MSD, Novartis, Pfizer, Regranion, Samsung, UCB. MH reports grants from Leo Pharma, grants from Procter and Gamble, non-financial support from Cherry Imaging, non-financial support from Cynosure-Hologic, grants and non-financial support from Lutronic, grants and non-financial support from Mirai Medical, grants and non-financial support from Novoxel, non-financial support from Perfaction Technologies, outside the submitted work. GBE Jemec has received honoraria from AbbVie, Chemocentryx, Coloplast, Incyte, Inflarx, Novartis, Pierre Fabre and UCB for participation on advisory boards, and grants from Abbvie, Astra-Zeneca, Inflarx, Janssen-Cilag, Leo Pharma, Novartis, Regeneron, Sanofi and UCB for participation as an investigator, and received speaker honoraria from AbbVie, Boehringer-Ingelheim and Galderma. He has also received unrestricted departmental grants from Abbvie, Leo Pharma and Novartis. SFT has received research support, been a speaker and served on advisory boards for Abbvie, Janssen, Novartis, Sanofi and UCB. DB and MKS have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize