


Scrotal calcinosis (SC) is a rare and benign condition characterized by multiple, calcified, usually asymptomatic, nodules in the scrotal skin (1). SC often appears in adolescence or early adulthood and may cause embarrassment (1, 2). The standard therapeutic approach is surgical excision of the affected skin (3, 4). We report here 2 cases of SC treated successfully with carbon dioxide (CO2) laser, enabling precise removal of the cysts, while sparing the surrounding tissue. To our knowledge, there are no previous reports in the literature describing treatment of SC with CO2 laser.
Case 1. A 37-year-old man presented with a 10-year history of multiple nodules on his scrotum. There was no family history of a similar condition. The patient denied a history of scrotal trauma and, apart from an acoustic neuroma, his medical record was unremarkable. Laboratory evaluations, including serum calcium, phosphorus, parathyroid hormone and 25-hydroxyvitamin D levels, were within normal ranges.
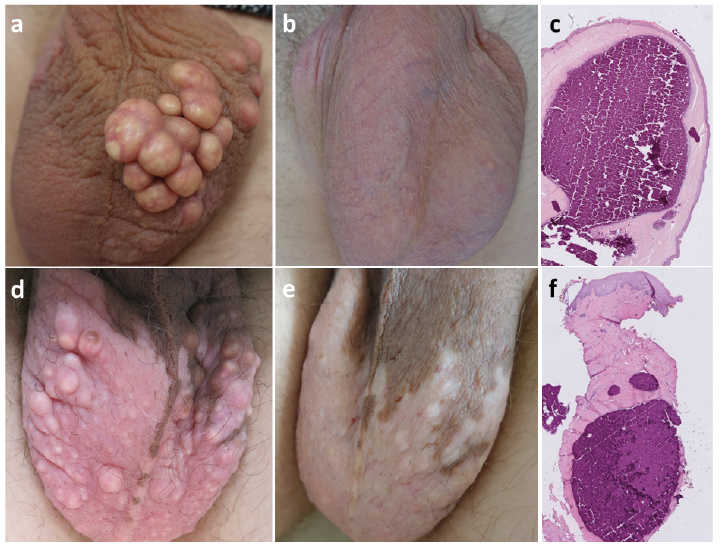
Physical examination revealed an area 15 cm in diameter with multiple, up to 3–4-cm, firm, yellowish nodules, mostly on the left side of the scrotum and one on the dorsum of the penis shaft (Fig. 1a). The patient was treated in one session with the SmartXide carbon dioxide (CO2) laser and focal 7” handpiece (Deka Laser, Florence, Italy), during which all the nodules were removed under local anaesthesia. The CO2 laser was used in continuous wave mode at a power of 5–6 W. Large cysts were excised by cutting and small ones were vaporized until fully ablated to minimize tissue loss. Hydrogen peroxide cream (1%) and surgical dressings were applied post-operatively for the first few daysdays. The wounds healed by secondary intention. Recovery time was 1.5 months and the patient reported no complications. Post-operative follow-up 1.5 years later showed no recurrence and the patient was very satisfied with the result (Fig. 1b).
Fig. 1. Clinical photographs and histology of 2 cases of scrotal calcinosis. (a–c) Case 1: (a) before, and (b) 1.5 years after carbon dioxide (CO2) laser treatment. (c) Histology section stained with haematoxylin and eosin (H&E). (d–f) Case 2: (d) before and (e) 5 months after the second CO2 laser treatment. (f) Histology section stained with H&E. Original magnification 40x.
Histological examination of a nodule revealed a dermal homogeneous basophilic calcium deposit intensively stained with haematoxylin-eosin, with no signs of epithelial lining. A foreign body reaction was seen around this large calcium mass, together with inflammation and fibrosis (Fig. 1c).
Case 2. A 26-year-old man presented with a 3-year history of an increasing number of nodules on his scrotum. The lesions caused embarrassment and had occasionally been inflamed, but were otherwise asymptomatic. He denied any scrotal trauma, and there was no family history of a similar condition. Except for vitiligo his medical record was unremarkable. Laboratory evaluation, including serum calcium, phosphorus, parathyroid hormone and 25-hydroxyvitamin D levels, showed no abnormalities.
Physical examination revealed multiple white-yellowish cysts, varying in size between 1 and 7 mm, distributed bilaterally on the scrotum (Fig. 1d). The patient was treated in 2 sessions with CO2 laser under local anaesthesia, using the same technique as described in case 1. Two cysts were sent for histological examination. Approximately 30 cysts were removed at the first visit and another 50 cysts at the second visit. The result was satisfactory and there was no sign of recurrence at follow-up 5 months later (Fig. 1e).
Histological examination demonstrated nodules, consisting of fine granular deposits, calcific spherules and larger amorphous sheets of basophilic material, in the upper and the deep part of the dermis, representing calcium deposits, with no signs of epithelial lining (Fig. 1f).The intensity of foreign body reaction was much less pronounced in this case compared with case 1.
Written informed consent was provided by both patients to publish their case details and photographs.
Scrotal calcinosis is a rare condition that presents clinically as firm yellowish nodules, varying in size from a few mm to several cm diameter, in the dermal skin of the scrotum (1, 2). The nodules are mostly asymptomatic, although some patients report itching, heaviness and discharge of chalky material (1, 2, 5). Onset is often in adolescence or early adulthood and the nodules tend to increase progressively in size and number over time (1, 6). The young age of onset and intimate location may cause embarrassment, and may result in delay in patients seeking medical attention. The 2 cases reported here both waited several years before seeking medical help.
Histopathological findings are calcium deposition within the dermis, with no systemic disorder of calcium/phosphorus balance (1). It is debated whether SC is idiopathic (1, 6) or originates from dystrophic calcification of pre-existing structures, such as epidermoid cysts, hair follicle cysts or eccrine duct milia (5, 7, 8). Recent studies support the latter theory, and suggest that the calcification is followed by rupture and destruction of the cyst wall, explaining the lack of epithelial lining in the late stage of the lesions (5, 7), as seen in the 2 cases reported here.
To our knowledge, this is the first report of CO2 laser treatment of SC. A PubMed search of the literature on 26 September 2020, using the terms “scrotal calcinosis [title]”, and “laser [title]” paired with “scrotal, scrotum or calcinosis cutis”, resulted in 155 articles. Single reports were found on the use of CO2 laser, diode laser and Nd:YAG laser for cases of scrotal cysts, but not scrotal calcinosis (9–11), in addition to a case of CO2 laser treatment for post-traumatic dystrophic calcinosis cutis of a knee (12). Only one publication reported treatment of SC with laser, using erbium:YAG laser (13).
Surgical excision of the affected area and direct closure or use of flaps/grafts is generally regarded as the standard treatment for SC, but may result in significant scarring and a reduction in scrotal volume (3, 4, 14). A less invasive technique with minimal tissue loss and excellent cosmetic outcome is thus desirable, and may be achieved using CO2 laser, which also provides immediate coagulation and haemostasis. This allows for a precise excision limited to the actual cysts, reduced bleeding with improved visual field, and very limited scarring compared with surgical excision.
We report here 2 patients with SC treated successfully with CO2 laser. The cosmetic result was equally good irrespective of the size of the cysts. In both cases the treatment was tolerable, there were no complications, and a recovery time of approximately 1–2 months was reported. The cosmetic results were excellent, with minimal or no scarring, the patients reported a high level of satisfaction, and no recurrence was observed at the follow-up visits. However, long-term recurrence remains to be evaluated.
Although the literature repeatedly describes the onset of SC at a sensitive age and a plausible impact of the condition on quality of life, self-esteem and sexual activity (3), there are no quantitative reports on health-related quality of life or stigmatization due to SC. It would be of interest to evaluate such data in future studies, as post-intervention improvements in these aspects would strengthen the value of this treatment.
In summary, due to the progressively disfiguring nature of SC, efficient treatment is important. We report here, for the first time, that CO2 laser treatment of SC provides a quick, tolerable and effective treatment with excellent cosmetic outcome and high level of patient satisfaction.
The authors acknowledge Dr Agnes Pekar-Lukacs from the Department of Pathology for her help with the histopathological analysis.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize