


1Oslo Centre for Biostatistics and Epidemiology, Department of Biostatistics, Institute of Basic Medical Sciences, University of Oslo, 2Department of Research, Cancer Registry of Norway, 3Oslo Centre for Biostatistics and Epidemiology, Oslo University Hospital, Oslo, Norway, 4Department of Population Health, QIMR Berghofer Medical Research Institute, Brisbane, Australia, 5Cancer Research UK Manchester Institute, University of Manchester, Manchester, UK, 6Department of Community Medicine, Faculty of Health Sciences, University of Tromsø, The Arctic University of Norway, Tromsø, Norway, and 7International Agency for Research on Cancer, Lyon, France
Patients’ phenotypic characteristics might be associated with melanoma aggressiveness, but the evidence is scarce. This study examined the associations be-tween pigmentary characteristics, naevi and melanoma thickness. Data from the Norwegian Women and Cancer (NOWAC) study were analysed. By 2014, 1,243 women were diagnosed with a primary melanoma, and 1,140 had information on thickness. Using ordinal logistic regression models, the probability of being diagnosed with a specific thickness category was calculated by pigmentary score and naevi. Fair pigmentary score was associated with thinner trunk melanomas (probabilities of being diagnosed with a tumour ≤1.0 mm thickness were 74%, 66%, and 51% for fair, medium and dark pigmentary scores, respectively), but not the other sites. High number of naevi was associated with thicker nodular melanoma (NM) but not with super-ficial spreading melanoma. These findings suggest the need for greater overall vigilance and skin checks among women with fair pigmentary score. The association between naevi and NM suggest possible biological mechanisms.
Key words: cohort study; pigmentary characteristics; mela-noma; prognosis; tumour thickness; naevi.
Accepted Apr 19, 2021; Epub ahead of print Apr 21, 2021
Acta Derm Venereol 2021; 101: adv00446.
doi: 10.2340/00015555-3806
Corr: Reza Ghiasvand, Department of Research, Cancer Registry of Norway, PB 5313 Majorstuen, NO-0304 Oslo, Norway. E-mail: reza.ghiasvand@kreftregisteret.no
The associations between pigmentary characteristics, naevi and melanoma thickness were examined. Data from the Norwegian Women and Cancer (NOWAC) cohort study, with 1,243 women diagnosed with a primary melanoma by 2014, were analysed. Fair pigmentary score was associated with thinner trunk melanomas (probabilities of being diagnosed with a tumour ≤ 1.0 mm thickness were 74%, 66%, and 51% for fair, medium and dark pigmentary scores, respectively). High number of naevi was associated with thicker nodular melanoma. These findings suggest greater overall vigilance among women with fair pigmentary score, and underscore the advice that women with many naevi should undergo routine skin examinations.
The associations between paler pigmentary characteristics, high numbers of melanocytic naevi and increased risk of melanoma are well-established (1, 2). However, little is known about the possible association between these characteristics and melanoma aggressive-ness. Vertical tumour thickness is the most important prognostic factor in localized primary melanoma (3, 4) and, in general, patients diagnosed with thinner tumours have longer survival than those with thicker tumours (3, 5). Tumour thickness is also the most reproducible histopathological factor in clinical reports (6).
Patients’ characteristics and their skin-awareness and healthcare use have also been linked to thickness of tumour at diagnosis (7–9). It has been hypothesized that high-risk phenotypes, such as fair complexion, might be associated with genetic determinants of more aggressive melanoma and a higher risk of thicker melanoma (10, 11). Conversely, having a high-risk phenotype might also be associated with greater skin awareness and early detection, and thus thinner melanomas at diagnosis (7).
A few studies have investigated the associations between phenotypic characteristics and melanoma thickness, with inconclusive results, but they were not population-based and they did not examine associations of skin type by melanoma site or subtype (10, 11). The aims of the current study were to investigate the associa-tion between pigmentary characteristics and naevi and overall melanoma thickness at diagnosis, as well as by body site and for the 2 most common subtypes of mela-noma, superficial spreading melanoma (SSM) and nodular melanoma (NM). Data from the Norwegian Women and Cancer (NOWAC) study, a prospective population-based cohort that is representative of Norwegian women, were analysed.
NOWAC cohort
The NOWAC study was established in 1991, and by 2007, 171,725 women (response ~54%) aged 30–75 years had completed and returned the questionnaire and given informed consent to participate. Details on the NOWAC cohort have been published (12). The unique identity number of Norwegian citizens was used to link NOWAC to the Cancer Registry of Norway (CRN) for follow-up of cancer incidence and vital status (alive, emigrated or dead) until 31 December 2014. The Norwegian Data Inspectorate and the Regional Committee for Medical Research Ethics approved the study.
Assessment of outcome
Primary tumour site and subtype are registered according to the International Classification of Diseases for Oncology, Seventh Edition (ICDO-3). Site was categorized as head/neck (190.0), trunk (190.1/190.7), upper limbs (190.2), lower limbs (190.3/190.4) and other (other (190.5/190.6/190.8)/skin not otherwise speci-fied (190.9)), and subtypes as SSM (87433), NM (87213), lentigo maligna melanoma (LMM; 87423) and other (acral lentiginous melanoma (87443)/melanoma unspecified (87203)/other (87453/87803/87613)). The Norwegian Malignant Melanoma Registry (NMMR) was established under the CRN in 2008, and information on tumour thickness for incident cases since 2008 was obtained from the NMMR. For melanoma cases before 2008, information on thickness was extracted manually from histopathological reports by experienced melanoma registrars in the CRN. Melanoma thickness was categorized into 4 T categories according to the 8th edition of the American Joint Committee on Cancer (3) (T1: ≤ 1.0; T2: > 1.0–2.0; T3: > 2.0–4.0; T4: > 4.0 mm). Through December 2014, 1,243 women were diagnosed with a primary invasive melanoma. Tumour thickness was unspecified for 103 women; hence the current study sample consisted of 1,140 women with primary invasive melanoma.
Assessment of phenotypic characteristics
The participants reported hair colour (dark brown/black, brown, blond/yellow, red), eye colour (brown, blue, grey/green/mixed) and their untanned skin colour (recorded by a 1×9-cm colour scale graded from 1 (very fair) to 10 (dark brown)). Skin colour was categorized as dark (grades 7–10), medium (grades 4–6), or light (grades 1–3). The participants also reported the number of asymmetrical naevi > 5 mm on arms (from armpit to fingers) or on the legs (from toes to groin) (0, 1, 2–3, 4–6, 7–12, 13–24, ≥ 25; categorized as 0, 1, ≥ 2), and freckling when sunbathing (yes, no). A colour brochure with pictures of 3 examples of asymmetrical naevi was enclosed with the questionnaire to increase accuracy of reports. Subsamples of the cohort were asked about the number of small symmetrical naevi on arms and on the legs (0, 1–10, 11–50, ≥ 51) and skin reaction to acute (brown, red, red with pain, red with pain and blisters) and chronic (deep brown, brown, light brown, never brown) sun exposure. Reproducibility has been studied for freckling when sunbathing (kappa = 0.77), number of small symmetrical naevi on the arms (weighted kappa = 65) and the skin colour scale (intraclass correlation = 0.59) (13).
Statistical analysis
A pigmentary score was constructed by summing the values of skin colour (dark = 0, medium = 1, light = 2), eye colour (brown = 0, blue = 1, grey/green/mixed = 2), hair colour (dark brown/black = 0, brown = 1, blond/yellow = 2, red = 3), and freckling when sun-bathing (no = 0, yes = 1) and categorized as dark (score < 3), medium (scores 3–5) and fair (scores 6–8) pigmentary score. The association between T category and phenotypic characteristics was examined by ordinal logistic regression and estimated odds ratios for higher (thicker) vs lower (thinner) T categories with 95% confidence intervals (CIs) (14). Then, from the specified ordinal logistic regression models, the probability of being diagnosed with each specific tumour thickness category was calculated for 1 unit change in the characteristics with significant association with tumour thickness, while holding all other covariates constant. To assess effect modification, the pigmentary score was dichotomized as darker (score < 5) and fairer (score ≥ 5), and the number of small symmetrical naevi as ≤ 50 and ≥ 51, and constructed a 4-category variable. The proportional odds assumption was checked using Brant test. Models were adjusted for age at diagnosis (continuous), birth-cohort (1927 to 1943, 1944 to 1948, 1949 to 1953, 1954 to 1965), place of residence (northern, central, southwestern and southeastern Norway), education (≤ 10, 11–13, ≥ 14 years), site of melanoma and subtype. In addition, analyses were conducted by body site and the 2 most common subtypes of melanoma (SSM and NM), associated with different biological behaviour (15, 16). Multiple imputations with chained equation were used, imputing 20 data sets to evaluate whether missing information influenced the estimates. Stata, version 15 (Stata Corp. College Station, TX, USA), was used for all analyses.
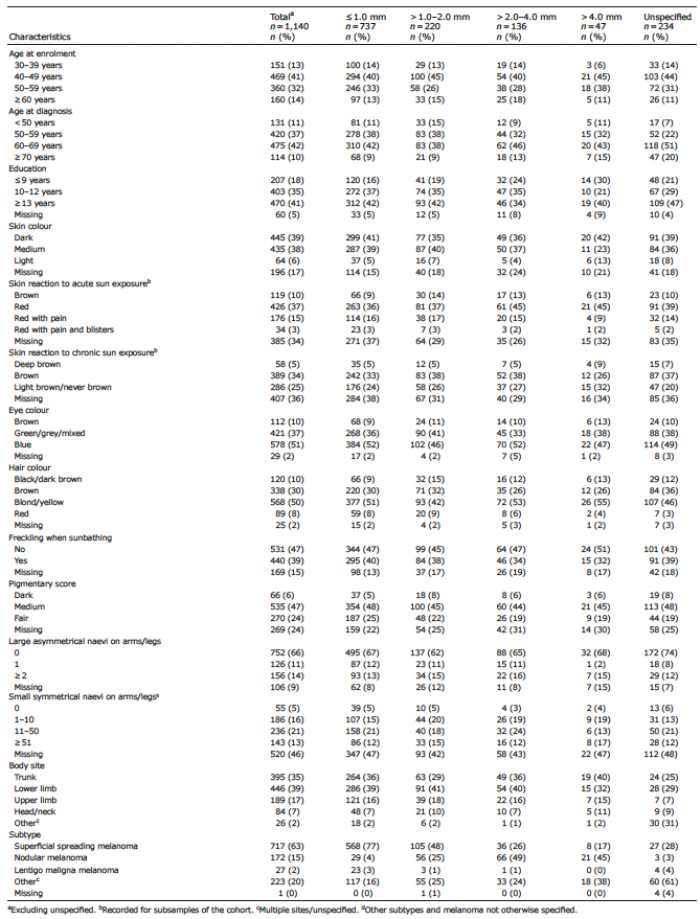
Among 1,140 patients, 737 (65%) were T1, 220 (19%) T2, 136 (12%) T3, and 47 (4%) T4 (Table I). The majority of cases were SSM (n = 717), followed by NM (n = 172), LMM (n = 27), and other (n = 224). Patients with thicker melanoma tended to be older at diagnosis, less educated, and NMs tended to be thicker at diagnosis (Table I).
Table I. Host and tumour characteristics in women with incident primary melanoma in the Norwegian Women and Cancer (NOWAC) cohort according to T category
After adjustment for age at diagnosis, birth-cohort, place of residence, education, body site and subtype, a significant inverse association was found between tumour thickness and pigmentary score and a positive association with small symmetrical naevi on arms/legs, but not large asymmetrical naevi on arms/legs (Table SI). The probability of being diagnosed with T1 melanoma was 56%, 67% and 68% for patients with dark, medium and fair pigmentary score, respectively (Table II). Furthermore, while women with no small symmetrical naevi on their arms/legs had 73% probability of being diagnosed with a T1 melanoma, the corresponding probability was 59% for women with ≥ 51 small symmetrical naevi. When combining small symmetrical naevi and pigmentary score, patients with darker pigmentary score had a lower probability of T1 melanoma when they had ≥ 51 small symmetrical naevi compared with having < 50 naevi, though the test for interaction was not significant (49% for ≥ 51 naevi vs 67% for <50 naevi; pinteraction = 0.20). Results from multiple imputation analyses were comparable with complete-case analysis (Table SI), suggested no bias due to missing; thus the presented probabilities are from complete case analyses.
Table II. Estimated probabilitya of being diagnosed with melanoma by T category for the association between phenotypic characteristics and T category in women with incident primary melanoma in the Norwegian Women and Cancer (NOWAC) cohort
In analysis by body site, fair pigmentary score was significantly associated with higher probability of being diagnosed with T1 melanoma on the trunk (74% for fair and 51% for dark pigmentary score), but no other sites (Table III and Table SII). Significantly lower probability of T1 melanoma in patients with ≥ 51 small symmetrical naevi vs < 50 naevi was found only for the upper limbs (41% and 64% probability of being diagnosed with a T1 melanoma, respectively). Here, no significant interaction was found between pigmentary score and small symmetrical naevi (0.15 ≥pinteraction ≤ 0.97; Table SII).
Table III. Estimated probability (Pr)a and 95% confidence interval (95% CI) of melanoma diagnosis in different sites by phenotypic characteristics and T category in women with incident primary melanoma in the Norwegian Women and Cancer (NOWAC) cohort
Fair pigmentary score was associated with thinner SSM (probability of being diagnosed with T1: 85% for fair vs 67% for dark pigmentary score), but not NM (probability of being diagnosed with T1: 17% for fair vs 16% for dark pigmentary score; Table IV). Compared with patients with < 50 small symmetrical naevi on arms/legs, patients with ≥ 51 naevi had higher probability of thicker NM (T1: 6% for ≥ 51 naevi vs 16% for < 50 naevi; Table IV). No significant interaction was found between pigmentary score and small symmetrical naevi in the analysis by subtype (pinteraction ≥ 0.60; Table SIII).
Table IV. Estimated probability (Pr)a and 95% confidence interval (95% CI) for diagnosis of superficial spreading melanoma (SSM) and nodular melanoma (NM) by phenotypic characteristics and T category in women with incident primary melanoma in the Norwegian Women and Cancer (NOWAC) study
This study provides new evidence on the association be-tween phenotypic characteristics and melanoma thickness. On overall analysis fair pigmentary score was associated with thinner melanomas. In site-specific analysis, fair pigmentary score was associated with thinner melanomas on the trunk, but no other sites. Moreover, fair pigmentary score was associated with thinner SSM, but not NM, while having ≥ 51 small symmetrical naevi on arms/legs was significantly associated with thicker melanomas overall, thicker melanomas on the upper limbs, and thicker NM, but not SSM.
Results of the only 2 published studies on sensitivity of the skin to ultraviolet (UV) radiation and melanoma thickness were inconsistent (11, 17). In a single-centre cross-sectional study, having a fairer skin type was associated with thicker melanoma at diagnosis (17), while in a cohort study, no associations were found between hair colour, sunburn susceptibility, and tanning ability and melanoma thickness (11). These studies were not population-based and they did not conduct analysis of skin type by melanoma site or subtype. The melanocortin-1 receptor gene (MC1R) is the key regulator of phenotypic traits, such as red hair, fair skin, freckles and skin sensitivity to UV radiation (18). Inherited variation in MC1R is associated with increased risk of melanoma (19); however, the studies that examined the association between MC1R and melanoma thickness reported no association (20–22), or a weak inverse association between MC1R gene variants and melanoma thickness (23). In the current study, patients with fair pigmentary score were more likely to be diagnosed with a thinner SSM, but not NM, and thinner melanoma on the trunk, but not other body sites.
The current study found that having ≥ 51 small symmetrical naevi on arms/legs was associated with thicker NM, but not SSM. The association between number of naevi and melanoma thickness has been studied previously, but with inconclusive results (24). In a cohort study, higher risk of thicker melanoma was associated with higher numbers of naevi among men, but not women (11). Conversely, other studies (10, 25) reported thinner melanoma in patients with many naevi. Similarly, a survey (26) found that, in patients < 60 years, a high total naevus count (> 50 naevi) was associated with thinner melanoma, but having > 5 atypical naevi was associated with thicker melanoma. It is proposed that thinner melanoma in patients with high naevus counts could be due to skin awareness and screening, since people with many naevi are recommended to have regular skin checks (7, 27). However, the current study finding does not support the hypothesis of thinner melanoma associated with high naevus count, and suggests possible underlying biological mechanisms that remain to be discovered.
Since melanoma incidence has increased rapidly in the past decades in most fair-skinned populations, early diagnosis has been a public health priority. Melanoma screening programmes encourage high-risk groups to have regular skin checks (20) and these efforts appear to be associated with a decrease in the thickness of SSM, but not NM (17), and with no reduction in melanoma mortality (29–31). NM is responsible for a large proportion of thick melanomas (32, 33), and the majority of deaths due to melanoma when excluding melanoma not otherwise specified (16, 34). A recent study in Australia reported more common skin checks among fair-skinned and sun-sensitive people (35). The finding in the current study of the thinner SSM, but not NM, at diagnosis among women with fair pigmentary score supports other reports (36, 37) that the challenge of early diagnosis of NM persists.
Large sample size in a prospective population-based study and the linkage to the CRN are important strengths of the current study. Reporting of incident cancers to the CRN is compulsory in Norway, and 99.9% of melanomas are morphologically verified (38). Results from multiple imputation analyses suggested no bias, due to missing data influenced the associations. This study is subject to some limitations. Phenotypic characteristics were self-reported, and some misclassification probably occurred. Also, histopathological misclassification of thick (> 2 mm) SMM as NM is possible; however, 84% of all melanomas, and 50% of NMs in the current study were thin melanomas (≤ 2 mm). Only half of the cohort was asked about the number of small symmetrical naevi on arms/legs, giving lower statistical power for this subsample and also in some of the sub-group analyses. Information on participants’ skin checks and skin cancer knowledge was also lacking. Thus, the findings should be interpreted considering these limitations.
In conclusion, this study found that fair pigmentary score was associated with thinner melanoma overall and SSM, but not NM. Importantly, ≥ 51 small symmetrical naevi on arms/legs was associated with thicker melanoma overall and NM. These findings underscore the public health advice that women with many naevi should under-go routine skin examinations. That thinner SSM, but not NM, are diagnosed on the trunk among women with fair pigmentary score is probably due to greater vigilance and skin checks among these women, although possible biological mechanisms remain to be explored.
Where authors are identified as personnel of the International Agency for Research on Cancer/World Health Organization, the authors alone are responsible for the views expressed in this article and they do not necessarily represent the decisions, policy or views of the International Agency for Research on Cancer/WHO.
This work was supported by the Norwegian Cancer Society [grant number 6823329].
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize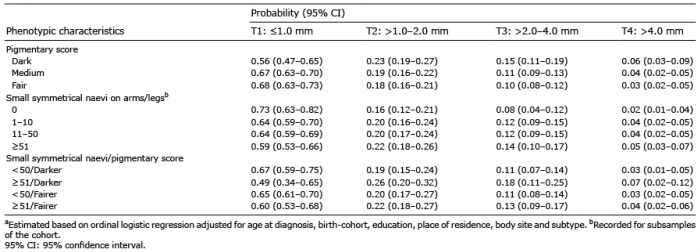 Click to show fullsize
Click to show fullsize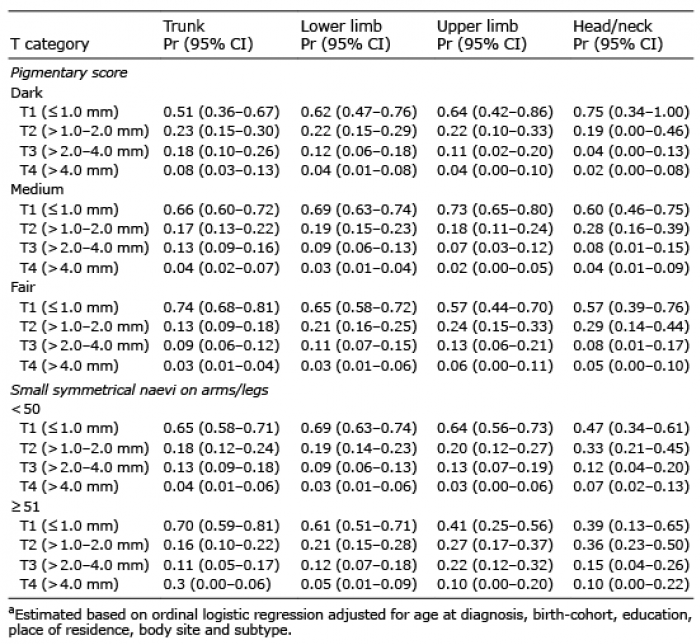 Click to show fullsize
Click to show fullsize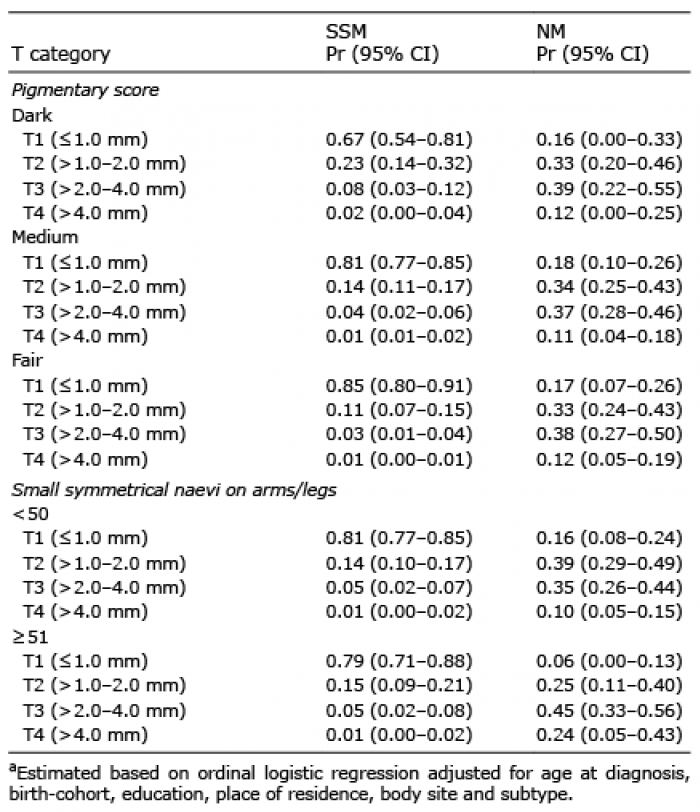 Click to show fullsize
Click to show fullsize