


1Department of Dermatology and Allergic Diseases and 2Institute for Pathology, University Hospital Ulm, Albert-Einstein-Allee 23, DE-89081 Ulm, Germany. E-mail: karin.scharffetter-kochanek@uniklinik-ulm.de
Accepted Apr 26, 2021; Epub ahead of print Apr 27, 2021
Acta Derm Venereol 2021; 101: adv00457.
doi: 10.2340/00015555-3812
Chronic leg ulcers have numerous causes and may pose a diagnostic challenge. Martorell hypertensive ischaemic leg ulcer (HYTILU) is a very rare disease, which is often missed in differential diagnosis. We report here a case of painful, initially unilateral, and subsequently bilateral, leg ulcers, which were misdiagnosed initially as pyoderma gangrenosa. This case report highlights the importance of histopathological diagnosis.
A 56-year-old man presented with painful ulcers on his right lower dorsal leg for 12 months. He noticed recently rapidly evolving new erosions on the left lower leg. Phlebological examination was normal. An external dermatological doctor´s office performed biopsy showed necrotizing vasculitis of the small and middle sized arterial vessels. Based on the clinical findings and pathology, the patient was diagnosed and treated for microscopic polyarteritis of the skin. Previous systemic prednisolone therapy, starting at 30 mg, tapered over weeks, and systemic antibiotic therapies had had no effect on the ulcerations.
The patient presented with a history of arterial hypertension for years, dyslipidaemia, obesity and coronary heart disease, treated with bisoprolol 2.5 mg 1-0-1, aspirin 100 mg 1-0-0 and atorvastatin 20 mg 0-0-1.
From the clinical viewpoint, differential diagnosis of pyoderma gangrenosum was considered. Medical examination did not show involvement of any internal organs, such as the kidneys. Anti-neutrophil cytoplasmic antibodies, anti-nuclear antibodies and a Magnet resonance-angiography of the legs and pelvis were normal. The systemic steroid dosage was reduced, while a concomitant azathioprine therapy was started and adapted to the tolerability and weight of the patient. However, even during treatment with azathioprine, 200 mg daily for more than 2 months, no improvement was observed. Azathioprine was withdrawn and exchanged for mycophenolatmofetil.
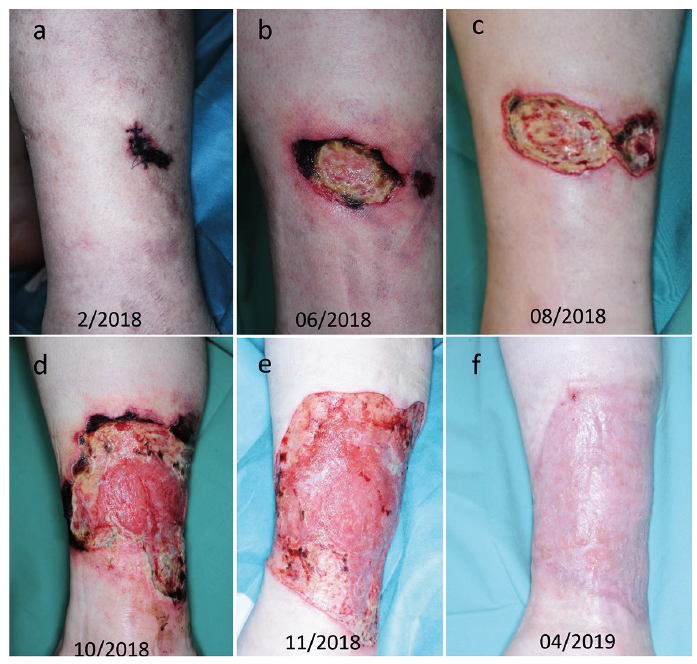
Despite immunosuppression, subcutaneous heparin, compression stockings, and suitable wound therapy, the ulcers increased in size and depth, especially on the left, previously mildly affected, leg (Fig. 1). To re-evaluate the diagnosis, another deep elliptical biopsy specimen down to the fascia was obtained. For the first time in the current patient, histopathology showed occluded vessels, intima hyperplasia, and media calcifications, supporting the suspicion of Martorell HYTILU (Fig. 2). A spacious operative necrosectomy and debridement of the involved tissue and affected margins and a vacuum therapy were applied; the latter was not tolerated for more than 4 days because of severe pain. In the meantime, immunosuppression was withdrawn. Another operative necrosectomy was needed 14 days after the first because the patient’s skin condition deteriorated, with the appearance of new necrotic margins. Split-skin grafts were administered. The patient reported significantly reduced pain after each operation, and long-lasting relief after the second intervention (initial pain medication tramadol, 50 mg at night; metamizole, 4 times/day; naloxone/oxycodone 10 mg/20 mg 1-0-1; additional tramadol and oxycodone if necessary; and subsequent metamizole 500 mg 2-2-2-2 and hydromorphone 16 mg 1-0-1-2, the latter tapered over time). In addition, blood pressure medication was optimized with additional ramipril 2.5 mg 1-0-0, and the patient was assigned to wear compression stockings daily. Six weeks after split-skin application a wound infection with multi-resistant Pseudomonas aeruginosa was apparent, which was treated with daily antiseptic wound dressings, ciprofloxacin thereafter due to persistence of Pseudomonas aeroginosa with meropeneme refraining from any occlusive dressing. A further necrosectomy was required approximately 8 weeks after the first operation; at this point the patient only needed metamizole, 500 mg 4 times daily.
At 4-month follow-up, the patient’s wounds had almost healed (Fig. 1F, G). To date, the patient has been pain-free for more than 12 months, with no new ulcerations.
Fig. 1. Clinical course of disease on the left lower leg. (a) Clinical photograph of left lower leg revealing haemorrhagic necrosis. (b) Increase in ulcer size, with necrotic borders, after 4 months. (c) After 6 months. (d) After 8 months. (e) After necrosectomy and split-skin grafting. (f) Fourteen months after first admission.
Fig. 2. Histopathological finding in deep elliptic biopsy of representative area. (a) Haematoxylin and eosin stained section of a deep elliptic excisional biopsy from the left lower leg (as shown in Fig. 1d; x 12.5). E: epidermis; D: dermis; SC: subcutaneous fat tissue; UR: ulcer edge; U ◊: ulcer. Black rectangles indicate location of magnified areas within the ulcer. (b) Superficial areas of the ulcer with neutrophil accumulation (×200). (c) Calcium deposits in the media (MC) and concentric intima hyperplasia (*) of an arteriole in the deep subcutaneous fat tissue (×400).
HYTILU is a rare entity, with peak of disease onset in advanced life (mean 74.5 years in some example cohorts), which typically manifests in patients with long-term arterial hypertension (1). Initially, haemorrhagic bullae can appear, transforming into necrotic ulcers (2). Wound margins are typically necrotic, with a peripheral growth pattern (3, 4). Compared with patients with other ulcers, those with HYTILU appear to show an inadequate pain level for the size and extent of the ulcers (4). At least half of affected individuals show a bilateral manifestation in the course of the disease (5).
It is thought that long-term hypertension with or without diabetes induces the typical ischaemic arteriosclerosis of small subcutaneous vessels (5, 6). It is also possible that the physiological vasodilating reflex at distal arterioles of the obstructed region is disrupted, further decreasing tissue perfusion (7). The characteristic histological findings usually include thickened vessel walls, narrowed vessel lumen, arteriolar thrombosis, and miniaturized Mönckeberg’s medial calcinosis (8).
Therapy usually consists of a combined regimen, including antihypertensive treatment, i.e. calcium channel blockers or angiotensin-converting enzyme inhibitors, surgical treatment, pain control, and potentially additional anticoagulation, preferably not with vitamin K antagonists (8). Furthermore, reports have described the potential benefits of supplementary hyperbaric oxygen therapy or negative-pressure wound therapy, prostaglandin E1 infusions, although with limited evidence (9, 10).
Correct differential diagnosis between HYTILU and pyoderma gangrenosa (PG) is a clinical challenge, and patients with HYTILU may be misdiagnosed with PG (11). Therapy for these conditions is crucially different, with HYTILU needing rapid surgical intervention and no immunosuppression. The histopathology of HYTILU shows characteristic patterns in the subcutis, which may not manifest if samples are taken too superficially. In the dermis, neutrophils may manifest in the same way as in PG, which further favours misdiagnosis (6).
We report here a case of non-healing leg ulcers in a 56-year-old man with a prolonged course of disease. Once the correct diagnosis of HYTILU was made, he underwent an excellent response to surgical treatment and split-skin grafts.
This case report highlights the importance of taking HYTILU and its complex symptoms into consideration in patients with chronic ulcers who show pyoderma gangrenosum-like lesions, especially in those with cardiovascular risk factors, as diagnosis is still likely to be less frequent than actual incidence (some authors report an incidence of 5–15% of all lower extremity ulcers) (4).
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize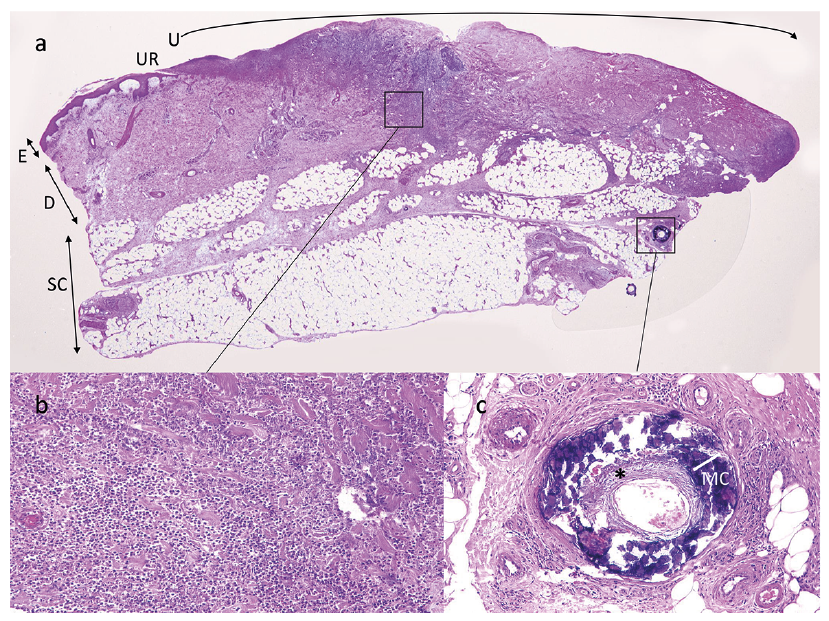 Click to show fullsize
Click to show fullsize