


1Department of Dermatology, University of Heidelberg, Heidelberg, 2Johannes Wesling Klinikum Minden, Minden and 3Department of Dermatology, University of Duisburg-Essen, Duisburg-Essen, Germany
The efficacy of psoriasis treatments is usually evaluated using the Psoriasis Area and Severity Index (PASI). However, there is a lack of systematic statistical assessments of PASI as a proxy for systemic disease in individual patients. Therefore, a retrospective study of 186 treatments with adalimumab, etanercept, and ustekinumab for psoriasis (341 patient-years) was performed. While PASI significantly and independently correlated with biomarkers of systemic inflammation (especially neutrophil-to-lymphocyte ratio, C-reactive protein), the strengths were only weak-to-moderate and varied considerably inter-individually. A decrease in PASI indicated a neutrophil-to-lymphocyte ratio decrease and a C-reactive protein decrease or stable low margin C-reactive protein in ≥ 80%. Sensitivity, specificity, and positive predictive value of PASI 0 and PASI 2.75 (optimal Youden Index) for low cardiovascular risk C-reactive protein were 24%, 92%, 85%, and 62%, 61%, 76%, respectively. Performance was similar using absolute thresholds and PASI 100 or PASI 75, and overall worse for low cardiovascular risk neutrophil-to-lymphocyte ratio and if psoriasis arthritis was present. In conclusion, PASI allows robust low-order estimates of systemic inflammation, but cannot substitute for laboratory biomarkers for more precise assessments.
Key words: psoriasis; biologics; biomarker; neutrophil-to-lymphocyte ratio; Psoriasis Area and Severity Index.
Accepted Apr 26, 2021; Epub ahead of print Apr 27, 2021
Acta Derm Venereol 2021; 101: adv00462.
doi: 10.2340/00015555-3814
Corr: Jochen Hoffmann, Department of Dermatology, University of Heidelberg, INF 440, DE-69120 Heidelberg, Germany. E-mail: jochen.hoffmann@med.uni-heidelberg.de
The efficacy of psoriasis treatments is usually evaluated by cutaneous response (Psoriasis Area and Severity Index; PASI). However, it is unclear how precise PASI improvements reflect systemic manifestations in individual patients. This study retrospectively analysed PASI and inflammatory biomarkers during 186 treatments (mean 22 months) of patients with psoriasis with biologics. While PASI decrease and complete cutaneous clearance indicated a decrease in inflammatory biomarkers and low cardiovascular risk levels of 1 of 2 inflammatory biomarkers, respectively, no single PASI threshold was both sensitive and specific enough for more precise assessments of systemic inflammation. Thus, further research into laboratory biomarkers as valid additional treatment goals would be desirable.
Psoriasis is a chronic inflammatory disease affecting approximately 2–3% of the population in Europe and North America (1). Relevant co-morbidities, in particular atherosclerosis and depression (”sickness behaviour”, 2), are thought to be driven by systemic inflammation, in what was coined a “psoriatic march” (3), and result in a reduction in life expectancy by up to 5 years, mainly due to cardiovascular events (4–6).
On the individual patient level in a dermatological setting, the efficacy of psoriasis treatments is evaluated mainly by cutaneous response, as Psoriasis Area and Severity Index (PASI) improvement, and, apart from arthritis, usually not by amelioration of systemic manifestations (7). While, overall, biologic treatments were shown to reduce biomarkers of systemic inflammation and are thought to reduce the excess cardiovascular risk (8), the precise relationship between PASI and biomarkers of inflammation and the worth of PASI as a proxy for systemic inflammation on an individual patient level under biologic treatment is unclear. Even though there is good evidence for a correlation between PASI and C-reactive protein (CRP) in untreated patients without arthritis, the situation is more complex under treatment (9). Indeed, different systemic therapies may differentially affect cutaneous manifestations and systemic inflammation (10, 11), and data on the association between the cutaneous response and vascular inflammation are inconsistent (12–14).
The current study presents a systematic statistical assessment of PASI as a proxy for biomarkers of systemic disease under biologic treatment on an individual patient level. A retrospective study was conducted of 186 treatment cycles with adalimumab, etanercept and ustekinumab for psoriasis. The correlation of PASI and biomarkers of systemic disease, including biomarkers for systemic inflammation and cardiovascular risk (CRP, neutrophil-to-lymphocyte ratio (NLR)), under long-term, “real-world” conditions in the general study population and on an individual patient level was analysed.
Patients
Patients with psoriasis were eligible for study participation if they were: (i) treated with adalimumab, etanercept, or ustekinumab at the University of Heidelberg, Department of Dermatology, (ii) could provide at least 1 data pair for the correlation of PASI with a routine laboratory parameter, and (iii) gave informed consent to retrospective data analysis. A total of 356 patient records were screened, and 152 patients providing 186 treatment cycles were found to be eligible. A treatment cycle encompassed the interval from initiation to termination of a specific treatment. A single patient could provide treatment cycles to different biologics. However, if a patient received more than one treatment cycle with a given biologic, only the first cycle was eligible. This study was conducted in accordance with the Declaration of Helsinki. Approval of the Institutional Review Board of the University of Heidelberg was obtained.
Standard treatment schemes and clinical status
Typically, adalimumab is administered subcutaneously (s.c.) with 40 mg every other week after an initial loading dose of 80 mg. Etanercept is administered s.c. with an initial dose of 25–50 mg biweekly or 25 mg weekly for 12 weeks, followed by biweekly administration of 25 mg or weekly administration of 50 mg following national guidelines (15). Ustekinumab is administered s.c. at weeks 0, 4, and 12-weekly thereafter at weight-adapted doses of 45 or 90 mg. Routine visits are usually scheduled every 8–12 weeks. PASI scores were accepted as baseline score only if obtained less than 30 days prior to treatment initiation.
Laboratory tests
Laboratory blood tests are routinely performed in patients with psoriasis receiving adalimumab, etanercept, and ustekinumab according to our standard operating procedures. Measurements of routine laboratory parameters were accepted as baseline values up to 30 days prior to treatment initiation, if no biologic treatment was administered during this period. The NLR and platelet-to-lymphocyte ratio (PLR) were calculated by dividing the neutrophil and thrombocyte count (numerator), respectively, by the lymphocyte count (divisor).
Statistical analysis
First, a robust Spearman’s rank correlation test was performed on a broad set of laboratory parameters and PASI to identify significant correlations. The correlation analysis was based on all available data pairs. The significance was corrected for the number of patients contributing data. The minimum effect size detectable with 80% power was calculated post-hoc with g*power (16) using the minimum number of patients contributing data (178) and α=0.05 (point biserial model). Secondly, Spearman’s correlations were calculated on an individual patient level and further assessed using a Wilcoxon signed-rank test. Finally, a partial Spearman’s correlation coefficient was calculated to compensate for potential confounding factors. Median under treatment CRP and NLR values were compared between patients who did and did not achieve an improvement of 75% and 100% (PASI 75 and PASI 100, respectively) in median over the course of the treatment using a Mann–Whitney U test. A multivariate binary logistic regression analysis was performed to identify baseline characteristics and parameters associated with a strong correlation between PASI, on the one hand, and CRP and NLR, on the other. Receiver-operating characteristics (ROC) curves were calculated to identify the optimal PASI threshold to predict lower cardiovascular risk category CRP and NLR values. Sensitivities, specificities and positive predictive values (PPV) of selected absolute and relative PASI thresholds were calculated for lower cardiovascular risk category CRP and NLR levels.
Values are presented as percentage, mean and standard deviation (SD), or median and interquartile range (IQR) as specified. p-values < 0.05 were considered significant. When Spearman’s correlation test results are reported, n denotes the number of patients contributing data that was used to calculate the p-value and not the actual number of data pairs investigated, which was usually much higher. Correlation coefficients were interpreted based on Cohen (17) to indicate weak (0.1), moderate (0.3) and strong (0.5) correlations. Statistical procedures were performed using SPSS 22.0 (IBM, New York, USA) and GraphPad Prism 6 (San Diego, CA, USA).
Significant correlation of Psoriasis Area and Severity Index with C-reactive protein, neutrophil and leucocyte count, and neutrophil-to-lymphocyte ratio
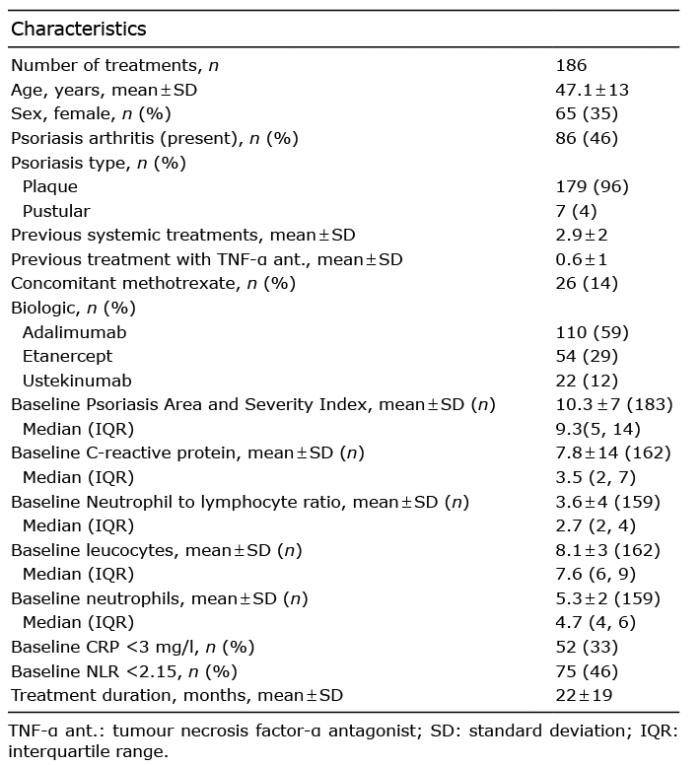
A total of 186 eligible treatment cycles, providing data over 341 patient-years, were identified. Overall patient characteristics are shown in Table I. First, the correlation between PASI and selected biomarkers was explored using a robust Spearman’s rank-correlation test. The results are shown in Table II. A significant positive correlation of PASI was found with CRP, neutrophil counts, NLR, and leucocyte counts. No significant correlation with PASI was found for the other parameters investigated, including transaminases.
Table I. Patient characteristics
Table II Spearman’s correlation coefficients between Psoriasis Area and Severity Index and selected biomarkers under biologic treatment
To arrive at a more intuitive measure of correlation, the differences between baseline and median under treatment PASI, CRP and NLR were reduced to simple ordinal classifiers (positive, equal, negative). NLR decreased in 81.3% of the patients whose PASI decreased under treatment (n = 128). CRP decreased in 55.5% and remained stable in 36.7% of the patients whose PASI decreased (n = 123). Of note, baseline CRP was already at the low margin of 2 mg/l in 97.9% of the latter patients with stable CRP. For further analyses, see Appendix S1.
Neutrophil-to-lymphocyte ratio and C-reactive protein are associated with Psoriasis Area and Severity Index independent of each other and treatment duration
NLR was significantly positively correlated with CRP and neutrophil counts (Spearman’s correlation coefficient: 0.262 and 0.629, respectively, both p < 0.001, n = 196), and negatively correlated with treatment duration (–0.167, p = 0.019, n = 196). Partial Spearman’s correlation tests between PASI and NLR were used to control for treatment duration, CRP, and neutrophil counts. The resulting partial correlation coefficients were 0.162, 0.163 and 0.112, respectively (controlled for treatment duration, CRP and neutrophil counts; p = 0.043, 0.043, 0.162; n = 157, 155, 157).
Likewise, partial Spearman’s correlation tests between PASI and CRP were used to control for NLR and treatment duration. The resulting partial correlation coefficients were 0.215 and 0.232, respectively (p = 0.007 and 0.003, n = 155 and 160, respectively). For further analyses see Appendix S1.
Inter-individual spread of the correlation of Psoriasis Area and Severity Index with neutrophil-to-lymphocyte ratio and C-reactive protein
To better account for repeated measures, Spearman’s rank-correlation analyses of PASI with CRP, neutrophil counts, and NLR were also performed for each patient individually, and the results were subsequently analysed using a Wilcoxon signed-rank test. The significant correlations of PASI with CRP, neutrophil counts, and NLR could be confirmed (median Spearman’s correlation coefficient: 0.20, 0.23, 0.21; n = 134, 174, 174, respectively; all p < 0.001). The IQRs of PASI-CRP and PASI-NLR were 0.6 and 0.6, respectively, indicating a considerable inter-individual spread of the correlations’ strengths.
Given the considerable spread, additional analyses were performed to assess whether selected baseline characteristics were associated with a strong correlation of PASI with CRP and NLR as potential confounding factors. The results are presented in Table III (PASI-NLR) and Table SI (PASI-CRP). While a higher baseline PASI and NLR and treatment with tumour necrosis factor (TNF)-α antagonists showed a trend to predict a strong NLR to PASI correlation, none of the parameters investigated reached significance. This was also true after elimination of irrelevant parameters using a stepwise backward approach in the final model (data not shown). For further analyses see Appendix S1.
Table III. Prediction of individual Spearman’s correlation coefficients between Psoriasis Area and Severity Index (PASI) and neutrophil-to-lymphocyte ratio (NLR) under treatment, according to baseline patient characteristics
Sensitivity, specificity and positive-predictive value of Psoriasis Area and Severity Index as a proxy for clinically relevant C-reactive protein and neutrophil-to-lymphocyte ratio cut-offs
CRP values of equal or more than 3 mg/l and NLR values of equal or more than 2.15 were reported to be independent cardiovascular risk factors and were therefore used as cut-offs (18, 19). Overall, 66% and 57% of CRP and NLR values, respectively, were below the stated cut-offs. ROC curves were calculated for both classifiers to identify PASI thresholds with optimal sensitivity and specificity for low cardiovascular risk CRP and NLR levels (Fig. S1). The best threshold according to the Youden Index to predict CRP and NLR values below the stated cut-offs was a PASI below 2.75 for both classifiers. Table IV compares the sensitivity, specificity, and PPV of a PASI of 0, a PASI of 2.75, a PASI 100 response, and a PASI 75 response to predict CRP values, NLR values and both values below the stated cut-offs. There was minimal variation in the study population for PASI 0 and PASI 2.75, on the one hand, and PASI 100 and PAS I75 response, on the other hand, since baseline PASI was not available for all patients (Table I). Overall, the statistical performance of the absolute and relative PASI thresholds was similar in the present long-term setting. Sensitivity, specificity and PPV were better for CRP compared with NLR. While PASI 0 and PASI 100 had high specificities for NLR and CRP below the stated cut-offs of approximately 90% and a PPV for CRP approximately 85%, the sensitivities were low. PASI 2.75 and PASI 75, on the other hand, had moderate sensitivities and specificities for both parameters of approximately 50–60%, while the PPV for CRP below the cut-off was somewhat lower, at 76%. Table V shows that the performances of PASI 100 and PASI 75 were slightly better overall in patients without psoriasis arthritis, in particular concerning predictions of the NLR cut-off. Again, the performance of PASI 0 and PASI 2.75 were comparable (Table SII). Table SIII shows that the performance of PASI 0 and 2.75 cut-offs for low cardiovascular risk CRP and NLR depended on the treatment duration. Overall, sensitivity was lower and specificity higher early during treatment.
Table IV. Statistical performance of selected Psoriasis Area and Severity Index (PASI) thresholds to predict low cardiovascular risk C-reactive protein (CRP) and neutrophil-to-lymphocyte ratio (NLR)
Table V. Statistical performance of selected Psoriasis Area and Severity Index (PASI) thresholds to predict low cardiovascular risk C-reactive protein (CRP) and neutrophil-to-lymphocyte ratio (NLR) in patients with and without psoriasis arthritis
This paper presents a thorough statistical analysis of PASI and biomarkers of systemic inflammation under biologic treatment with the TNF-α antagonists adalimumab and etanercept, and the IL12/23 antagonist ustekinumab.
First, the data show weak-to-moderate, yet significant, correlations between biomarkers of systemic inflammation and PASI under biologic treatment. NLR and CRP, in particular, were associated with PASI independent of each other and of treatment duration as potential confounding factors.
Even though good evidence exists for a reduction in CRP under biologic treatment (20, 21) and for a correlation of PASI and CRP in untreated patients (9, 22), less data are available on the correlation of CRP and PASI under biologic treatment (9). The results of the current study are in line with a study of 152 patients with psoriasis treated with adalimumab, who demonstrated a correlation between CRP and Physician Global Assessment at week 16 (23), and with a study of 42 patients with psoriasis, approximately half of whom received biologic treatment, where only the responding patients showed a positive correlation between PASI and CRP (24). Conversely, a study of 43 patients with psoriasis, 13 of whom received biologic treatment, did not find a statistically significant correlation between PASI and CRP 3 and 6 months after initiation of systemic treatment, possibly due to a small sample size (25). None of these studies investigated the correlation of PASI and CRP on an individual patient level.
Increased NLR was reported previously in patients with psoriasis compared with healthy controls; however, insufficient data were available to conclude that NLR correlates with PASI (26). The current results are generally in line with a study of 236 Japanese patients with psoriasis, which showed a reduction of NLR under biologic treatment that was more pronounced in patients with a PASI 75 response after 3–4 months (27). However, the direct association between PASI and biomarkers of systemic inflammation was not assessed. Zhang et al. (28) reported that NLR decreased in patients with psoriasis treated with biologics in unblinded clinical trials. However, this latter study was limited to 3 months follow-up and included only 35 patients with psoriasis. Possibly due to sample size limitations, their study was unable to detect a correlation between NLR and PASI. Therefore, the current data are an important addition to the available body of evidence.
Secondly, and importantly, the current study assessed whether PASI values under biologic treatment allow predictions of values of concomitant biomarkers of inflammation on an individual patient level. To the best of our knowledge, this is the first study to report a systematic investigation of this matter.
The main findings of the current study were: first, a PASI decrease indicated an NLR decrease and a CRP decrease or stable low margin CRP in ≥ 80%. Secondly, the correlation of PASI with CRP and NLR varied considerably on an individual patient level. Thirdly, overall, the sensitivity, specificity and PPV of a PASI of 0 and a PASI of 2.75 (i.e. the PASI threshold with the optimal Youden Index) for low cardiovascular risk CRP were 24%, 92%, 85%, and 62%, 61%, 76%, respectively. Fourthly, the specificity of PASI for low cardiovascular risk CRP and NLR was better, and the sensitivity worse early during treatment. And fifthly, the statistical performance of absolute and relative PASI thresholds was similar, and overall worse for low cardiovascular risk NLR and if psoriasis arthritis was present.
Practically speaking, overall, a patient with a PASI of 0 had an 85% chance of having a concomitant low cardiovascular risk level CRP value (compared with a 76% chance for a patient with a PASI of less than 2.75 and a 55% chance for a patient with a PASI of more than 2.75). Given the sensitivities of 24% and 62%, 76% and 38% of patients with low cardiovascular risk level CRP values had a PASI above 0 and 2.75, respectively. More recently, a discussion about early, aggressive treatment of psoriasis to reduce systemic inflammation and prevent systemic co-morbidity has evolved (8). With this in mind, the current data cautiously suggest that that complete clearance of skin lesions (i.e. PASI of 0) may not be the optimal indicator of low systemic inflammation. While PASI allowed robust low-order estimates, it was not well-suited for more precise predictions of systemic inflammation in individual patients. Further research is needed to evaluate, and possibly define, a minimal set of biomarkers of inflammation as valid additional treatment goals per se.
Study limitations, power and generalizability
As confounding factors are inherent to a retrospective study design, they could not be completely controlled for. Also, cardiovascular endpoints were not directly investigated, but biomarkers were used as a proxy for systemic disease. This approach is, however, supported by a variety of studies, notably concerning systemic inflammation in the field of cardiovascular medicine, indicating that biomarkers are well-suited to identify at-risk populations (29, 30). Conventional CRP values, which are broadly available, and not high sensitivity CRP, were used. Our laboratory reports these values left-censored at 2 mg/l. Since non-parametric testing and nominal transformation was used, left-censoring is not expected to affect statistical results. The correlation between PASI and CRP might, however, differ for high-sensitivity CRP, which is left-censored at lower values of 0.3–0.5 mg/l, with a threshold for cardiovascular risk at ≥ 2 mg/l according to the American Heart Association (31). The current study focused on 2 older classes of biologics, which have been available on the market for a long time. Therefore, long-term data were readily available. Furthermore, probably due to their long presence on the market, some of the more convincing data on a reduction in mortality under biologic treatment in psoriasis involve TNF-α antagonists (8). However, the effects of biologic treatment on mortality are a controversial issue and several lines of evidence also point to beneficial effects of IL 12/23 blockade and newer generation biologics including IL-17 antagonists (32, 33). Therefore, further research is needed to re-examine the current findings in newer generation biologics.
The strengths of this study are its real-world setting, the availability of PASI and biomarker values at a high temporal resolution, its approach to assess PASI and biomarker correlations in a first explorative step without a priori assumptions, and the long observation period. The sex, age, and PASI of the current study population are comparable to registry data reported for psoriasis patients under systemic treatment in Germany (34). The power to detect a Spearman’s correlation coefficient of at least 0.21, corresponding to a weak-to-moderate correlation according to Cohen (17), was more than 80% for all parameters investigated in the initial correlation analysis presented in Table I (see Methods).
In conclusion, this study expands the available evidence by confirming an independent, weak-to-moderate correlation of PASI with CRP and NLR under biologic treatment. Secondly, and importantly, the study also investigated the value of PASI as a proxy for systemic inflammation on an individual patient level. We conclude that PASI allows robust low-order estimates of systemic inflammation, but is not an adequate substitute for laboratory biomarkers for more precise assessments. Thus, further research is needed to evaluate, and possibly define, a minimal set of biomarkers of inflammation as valid additional treatment goals per se.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize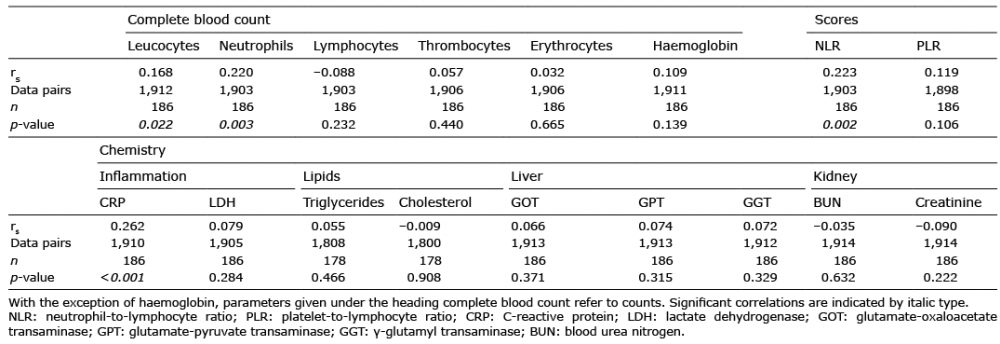 Click to show fullsize
Click to show fullsize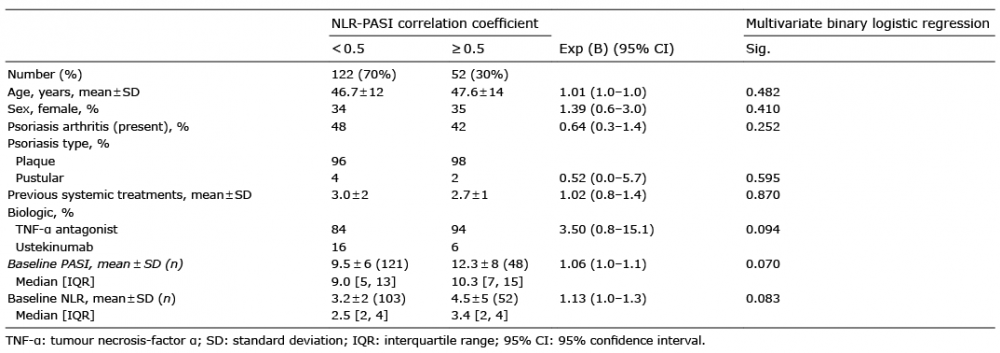 Click to show fullsize
Click to show fullsize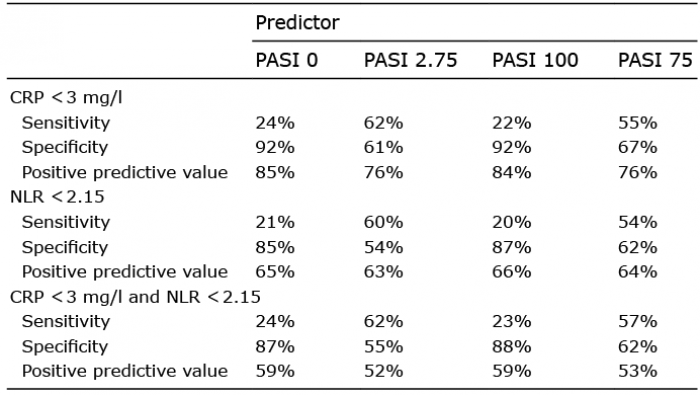 Click to show fullsize
Click to show fullsize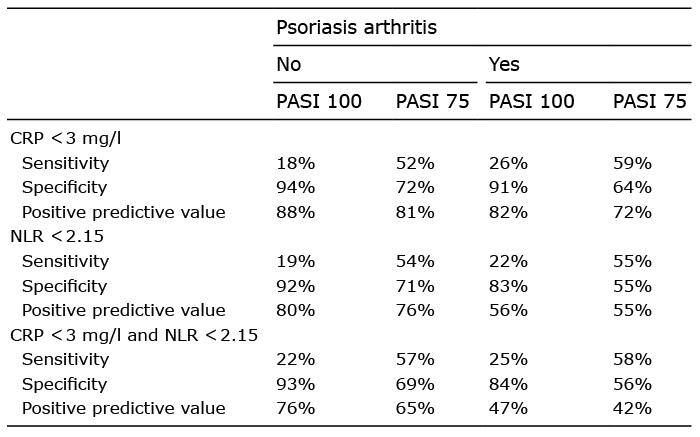 Click to show fullsize
Click to show fullsize