


1Department of Dermatology, Radboud University Medical Center and 2Radboud University, Nijmegen, The Netherlands
#Both authors contributed equally as first authors.
Dose reduction of biologics for psoriasis could contribute to lower drug exposure. This study evaluated a one-step, tightly controlled, biologic dose reduction strategy in a prospective daily practice cohort. In patients with psoriasis with low disease activity using adalimumab, etanercept or ustekinumab for at least 6 months, the dosing interval was prolonged with 33%. Patients could return to their normal dosing interval in case of disease flare. Of 108 eligible patients, 80 started dose reduction and were analysed. In total, 36/80 patients (45.0%) discontinued dose reduction after 19 months (95% confidence interval 14.9–23.1 months). Of 67 patients with 1-year follow-up, 45 (67.2%) still used the lower dose after 1 year. No serious adverse events related to dose reduction occurred. Cumulative dose and costs decreased by 22.7% during 1 year. In conclusion, a one-step tightly controlled dose reduction strategy for adalimumab, etanercept and ustekinumab has considerable potential to safely decrease biologic dosages in patients with psoriasis in daily practice.
Key words: psoriasis; biologics; dose reduction; daily practice.
Accepted Apr 26, 2021; Epub ahead of print Apr 27, 2021
Acta Derm Venereol 2021; 101: adv00463.
doi: 10.2340/00015555-3815
Corr: Lara S. van der Schoot, Department of Dermatology, Radboud University Medical Center, René Descartesdreef 1, PO Box 9101, NL-6500 HB Nijmegen, The Netherlands. E-mail: lara.vanderschoot@radboudumc.nl
Biologics are effective medications for psoriasis. Dose reduction of biologics for psoriasis could contribute to more personalized treatment. This study evaluated a one-step biologic dose reduction strategy in daily practice. The dose was reduced in 80 psoriasis patients with adequate disease control using adalimumab, etanercept or ustekinumab for at least 6 months. Patients could return to their normal dose in case of disease flare. After 1 year, 67% of patients were still on a lower dose. Cumulative dose and costs decreased. Therefore, a one-step tightly controlled dose reduction strategy for adalimumab, etanercept and ustekinumab has considerable potential to decrease biologic dosages.
Biologics are effective therapies for moderate-to-severe psoriasis. However, treatment with biologics is often based on general guidelines and standard dosing regimens. This may not always suit the individual patient. Dose reduction (DR) of biologics in psoriasis could contribute to more personalized treatment. High costs and long-term safety concerns associated with biologics make DR desirable for implementation in daily practice.
In a recent pragmatic randomized controlled trial (RCT) we investigated a tightly controlled DR strategy in patients with psoriasis with stable low disease activity: the CONDOR study (1). Although non-inferiority regarding disease activity was not demonstrated, DR of adalimumab, etanercept, and ustekinumab was possible in 53% of patients, without safety concerns. Other studies also showed that DR of adalimumab, etanercept and ustekinumab is possible in patients with low disease activity (2–5), but success rates differ based on success definition, DR strategy and study design.
For further implementation of such a strategy, it is essential to study the gains and investments needed in daily practice. Therefore, the aim of this study was to prospectively evaluate a one-step tightly controlled DR strategy in daily practice. This strategy, based on the CONDOR study, was incorporated in clinical practice. The strategy is guided by disease activity and patients’ reported quality of life (QoL). Instead of 2 DR steps in CONDOR, we started conservatively with only one step, leading to 67% of the original dose. The use of this adapted, one-step tightly controlled DR strategy in daily practice was evaluated regarding time investment, practicability, patients’ experiences, success rate, patient and treatment characteristics, safety and cost reduction.
Design and participants
This prospective, clinical evaluation was conducted at the department of dermatology of Radboudumc, an academic hospital in the Netherlands, between February 2018 and February 2020. The tightly controlled DR strategy of the CONDOR study was adapted and evaluated in clinical practice in our hospital after retrieving first trial results (1). In CONDOR, eligible patients had Psoriasis Area and Severity Index (PASI) scores ≤ 5 at 2 subsequent visits in the past 6 months and Dermatology Life Quality Index (DLQI) scores ≤ 5 at inclusion. In our daily practice strategy, patients were asked to participate in case of low disease activity for at least 6 months according to the treating physician, with PASI and DLQI scores ≤ 5 at start of DR. Participation on patients’ request despite PASI or DLQI > 5 or treatment < 6 months was allowed after approval from their treating physicians. In accordance with the trial, adult patients with plaque psoriasis as primary indication for biologic use, should use adalimumab, etanercept or ustekinumab at the registered dose (40 mg every other week, 50 mg per week, 45 mg or 90 mg every 12 weeks, respectively) for at least 6 months before starting DR. In case of psoriatic arthritis (PsA), patients should have adequately controlled joint inflammation. The treating rheumatologist was consulted for approval of DR in case of doubt. The use of concomitant anti-psoriatic drugs was permitted.
Instead of 2 DR steps, DR was started conservatively with only one step. The interval was prolonged, leading to 67% of the original dose. In case of a disease flare (i.e. PASI and/or DLQI score > 5), patients were advised to return to the (previous) effective or authorized dose of their biologic. Patients could also return to the (previous) effective dose at their own request.
All patients at our outpatient clinic for biological treatment were screened by a dedicated nurse, to determine whether they were possible candidates for DR. In case of a negative first screening result, patients were screened again before every subsequent visit. Possible eligible patients were asked to participate by their treating physician (i.e. shared decision-making). Patients’ motivations for participating in the strategy and for not participating were collected.
Outpatient visits took place every 3–6 months with monitoring of disease activity by PASI and DLQI, according to usual practice. Extra visits could be scheduled at patients’ request. Patients were also asked to complete the Skindex-29 questionnaire, a dermatology-specific quality of life questionnaire (6–8). During follow-up, patients were asked about their experiences with the DR strategy, as well as their reasons for discontinuation of DR. Patients were stimulated to contact their physician in case of disease worsening. When patients were not able to visit the clinic, a telephone contact was made. Safety monitoring was carried out according to existing guidelines for clinical practice, and serious adverse events (SAEs) possibly related to DR were collected.
All data were anonymized and collected using a web-based data management system, CASTOR (9). All patients have been included in the prospective BioCAPTURE registry, as described elsewhere (10), and therefore provided written informed consent to use their clinical data for scientific purposes.
Outcomes
The aim of this study was to evaluate the use of the adapted DR strategy in daily practice. Therefore, the numbers of patients eligible for DR were analysed. Patients’ opinions and experiences were assessed, including reasons for participating and for not participating, and reasons for stopping DR. The success of the DR strategy was measured by the proportion of patients using a lower biologic dose up to 1 year, and the proportion of patients who stopped DR including time until stop. Regarding safety, SAEs possibly related to DR were assessed. Furthermore, disease activity (PASI scores) and patient-reported quality of life (DLQI and Skindex-29 scores) during 1 year of DR were evaluated. Cumulative reduced biologic doses and costs were compared with the normal doses. Other indirect costs, such as other medical costs or visit costs, were not included. Biologic costs were based on actual Dutch prices during the study (11).
Statistical analysis
Data were extracted from the database and imported into SPSS Statistics 25 (IBM, Armonk, NY, USA) for analysis. Patients who stopped DR ≤ 1 month and patients who were included < 3 months before data lock were excluded from analyses. Follow-up ended when patients discontinued DR or at the moment of data lock, whichever came first. Depending on the type of variable and its distribution, descriptive statistics are presented as percentages with absolute numbers, means with 95% confidence intervals (95% CI) or medians and interquartile ranges (IQR). In order to analyse outcomes for different time-points, visit data were centred into the nearest 3-monthly time-points (i.e. visit months) with a window of ± 6 weeks.
Screening results of patients possibly eligible for DR were summarized, and the number needed to screen (NNS) of all patients from the biologic outpatient clinic to detect one patient who started DR was calculated. Baseline characteristics of participating patients were summarized, as well as patients’ motivations for participation or refusing participation, patients’ experiences regarding DR, proportion of patients on a lower dose, proportion of patients who stopped DR (for the total cohort and per biologic), and reasons for stopping DR. The time until stop of DR was presented graphically by a Kaplan–Meier curve and patients were censored when follow-up ended. Median survival time was calculated for the total group and per biologic. Based on PASI and DLQI scores at the moment of DR discontinuation, the total number of patients who stopped due to a disease flare (i.e. PASI and/or DLQI > 5) was calculated. Of patients with PASI > 5, further PASI course for the next 6 months was checked in their patient records. The proportion of patients who discontinued DR despite low PASI and/or DLQI scores was also calculated. SAEs possibly related to DR (e.g. psoriasis exacerbation requiring hospitalization) were counted.
For subanalyses of outcomes after 1 year, a subcohort of patients with sufficient follow-up was defined, including patients who started the DR strategy ≥ 1 year ago. For this subcohort, the proportion of patients who were still on a lower dose after 1 year was calculated. PASI, DLQI and Skindex-29 were analysed in 2 ways. First, data of continuing patients only were analysed (“as treated” analysis), and second, “intention to treat” (ITT) analysis with imputation of missing values using last observation carried forward (LOCF) was performed on the total group. The LOCF method carries forward the last available outcome, which leads to more conservative estimations (12). The dose used in the first year of the DR strategy was calculated for the subcohort of patients who started DR ≥ 1 year ago. In case patients discontinued DR, their used dose during the rest of the year was substituted. The mean reduction in the biologic dose compared with the normal dose per label, and corresponding cost reduction, were calculated.
Participants
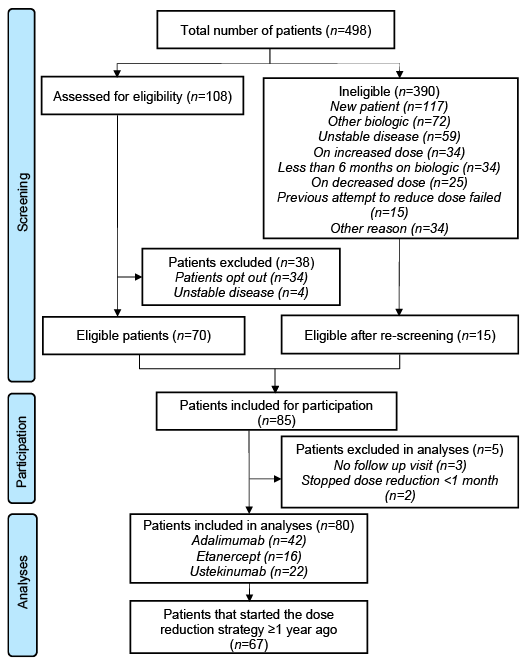
In total 498 patients visiting our outpatient clinic for biological treatment were screened between February 2018 and February 2020. The screening results are shown in Fig. 1. In total, 390 out of 498 patients did not qualify for DR, for the reasons stated in Fig. 1. This resulted in a group of 108 patients eligible for DR. After re-screening of 390 ineligible patients, 15 patients were included because they achieved stable disease activity, used normal doses again, reached 6 months treatment duration or because of other reasons. In total, 85 out of 498 (total clinic population) started with DR, resulting in a NNS for one patient on DR of 5.9. Five patients were excluded from analysis (see Fig. 1). The total follow-up duration ranged from 49 to 670 days (mean 365 days). A subcohort of 67 patients who started the DR strategy ≥ 1 year ago was defined for subanalyses. The time investment of the dedicated nurse was approximately 1 h per 16 patients. Baseline characteristics of the participating patients are shown in Table I. Overall, baseline PASI and DLQI scores were low. However, 3 patients started DR at their own request with DLQI scores > 5. One patient insisted on starting DR despite PASI > 5, but had a limited affected body surface area (2.3%) and a DLQI score of 0 and was therefore allowed to start DR.
Fig. 1. Screening results and eligible patients. Patients with psoriasis who visited the outpatient clinic for biological treatment were screened between February 2018 and February 2020. Only patients with stable, low disease activity for at least 6 months and using adalimumab, etanercept or ustekinumab at the normal, registered dose could participate.
Table I. Baseline characteristics of participating patients
Patients’ opinions and experiences
Patients’ reported motivations for participating are shown in Table II. The most important reason for starting DR was “minimizing medication use”. Of all patients who did not want to participate, the most frequently reported reason was “fear of psoriasis flares”. During follow-up, a random sample of 55 participants were asked about their experiences. Of this sample, 36 patients (65.5%) were positive or satisfied regarding DR, 13 patients (23.6%) were slightly positive/moderately satisfied, and 6 patients did not respond. No participants were dissatisfied.
Table II. Reasons for participating (n = 80)
Dose reduction characteristics
Of all patients who started DR (n = 80), regardless of their follow-up duration, 44 (55%) continued and 36 (45%) discontinued DR. DR was stopped by 19/42 (45.2%) adalimumab patients, 7/16 (43.8%) etanercept patients and 10/22 (45.6%) ustekinumab patients. The number of patients who discontinued DR per visit month is shown in Table III. In total, 7/36 discontinuing patients had PASI and/or DLQI scores > 5, whereas 22/36 patients discontinued DR despite low PASI and/or DLQI scores. Two patients stopped DR due to an increase in joint complaints, with one patient already having PsA. Rheumatological examination of the other patient did not reveal PsA. During follow-up, a total of 8 patients temporarily showed a PASI > 5, of which 4 patients continued DR at their own request and regained PASI < 5 within 6 months. Of 4 patients with PASI > 5 who discontinued DR, 3 patients regained PASI < 5 within 6 months. One patient with baseline PASI > 5 discontinued DR at 6 months (PASI > 5). All patients with high baseline DLQIs (n = 3) discontinued DR at month 3, with one patient having PASI > 5. The median time until stop was 19 months (95% CI 14.9–23.1) as presented in a Kaplan–Meier curve (Fig. 2). Reasons for stopping DR were reduced effectiveness experienced by the patient (n = 18; 50%), reduced effectiveness experienced by both physician and patient (n = 9; 25%), joint complaints (n = 2; 5.6%), or another reason/missing (n = 7; 19.4%). No serious adverse events (SAEs) related to DR were reported. There were no changes in concomitant immunosuppressant use.
Table III. Numbers of patients who discontinued dose reduction (DR) per visit month
Fig. 2. Kaplan–Meier survival curves for time until stop of dose reduction (DR). (a) Time until stop of DR for all biologics (n = 80). Median time until stop was 19 months (95% CI 14.9–23.1 months). (b) Time until stop of DR split per biologic. Data include 42 patients on adalimumab (ADA) (n = 19 stopped DR), 16 on etanercept (ETA) (n = 7 stopped DR) and 22 on ustekinumab (USTE) (n = 10 stopped DR). Median time until stop was 9 months (95% CI 14.7–23.3 months) for adalimumab, and 19 months (95% CI 12.0–26.0 months) for ustekinumab. For etanercept, the median time until stop of DR could not be calculated, as > 50% was still active in the survival curve at end of analysis.
From the subcohort of patients who started DR ≥ 1 year ago (n = 67), 45 patients (67.2%) were still on a lower dose after 1 year. Twenty-seven out of 37 (72.9%) adalimumab patients, 8/14 etanercept patients (57.1%) and 10/16 (62.5%) ustekinumab patients were on a lower dose after 1 year.
Disease activity and quality of life
PASI, DLQI and Skindex-29 during 1 year were analysed in 2 ways (as treated and ITT with LOCF) as shown in Fig. 3. Analyses were performed within the subcohort of patients who started DR ≥ 1 year ago (n = 67). During 1 year of DR, PASI scores were low (median [IQR], 1.6 [0.2–2.5] at baseline, 1.7 [0.5–3.0] at month 6 and 1.9 [0.8–2.8] at month 12 in as treated analyses) with a maximum range of 0–6.9. Median DLQI scores (as treated) were 0 [0–1] at baseline, 0 [0–1.5] at month 6 and 0.5 [0–2] at month 12. For Skindex-29, median scores (as treated) were 5.2 [0.9–16.4] at baseline, 5.2 [0.9–13.8] at month 6 and 6.9 [0.9–14.7] at month 12. Both median DLQI and Skindex scores correspond with minimal impact of psoriasis on patients’ QoL (13, 14). ITT analysis with LOCF gave a more conservative estimate of PASI, DLQI and Skindex-29, with slightly higher scores after month 6 compared with the as treated analysis.
Fig. 3. Psoriasis Area and Severity Index (PASI), Dermatology Life Quality Index (DLQI) and Skindex-29 scores by analysis method. Total number of patients n = 67. Data are presented as medians with interquartile range (IQR). Range of total possible scores: PASI 0–72, DLQI 0–30, Skindex-29 0–100. Number of missing observations per visit month for the as treated analyses (n): PASI 3 (month 0), 3 (month 3), 1 (month 6), 2 (month 9), 1 (month 12); DLQI 1 (month 0), 3 (month 3), 1 (month 6), 0 (month 9), 3 (month 12); Skindex-29 8 (month 0), 2 (month 3), 2 (month 6), 0 (month 9), 1 (month 12).
Biologic doses and costs
The cumulative dose during 1 year of the DR strategy was calculated for the subcohort of patients who started DR ≥ 1 year ago (n = 67). In total, a 22.7% reduction in biologic dose and costs was achieved after 1 year compared with the per label dose, resulting in absolute cost savings of €159,228.16. Mean dose per patient per biologic, cost savings and the corresponding percentage reduction are shown in Fig. 4.
Fig. 4. Mean doses per patient and percentage reduction in normal dose and costs after 1 year of dose reduction (DR) strategy. Data are presented for the subcohort of patients who started DR ≥ 1 year ago (n = 67). Cost savings are presented as mean per patient and were based on actual local prices per injection on 1 April 2020: adalimumab (ADA) €390.87; etanercept (ETA) €181.92; ustekinumab (USTE) 45 mg €1,410.13; ustekinumab 90 mg €2,820.27.
This prospective evaluation shows that a one-step tightly controlled DR strategy of adalimumab, etanercept and ustekinumab for patients with psoriasis is possible in daily practice. Of 108 patients with low disease activity, 85 started DR. The most important reason among patients for starting DR was “minimizing medication use”, whereas for not participating this was “fear of psoriasis flares”. After 1 year, 67% of patients were still on a lower dose. QoL and disease activity remained stable, and no SAEs related to DR occurred. Of patients with temporary PASI > 5, disease remission was regained in the vast majority of patients. Consequently, direct medication costs were reduced substantially by 22.7%.
The DR strategy described here was based on a RCT on tightly controlled DR of adalimumab, etanercept and ustekinumab in patients with psoriasis (CONDOR) (1). In the current study this strategy was adapted in order to make it more applicable for daily use. Inclusion criteria were less strict, the approach was more patient driven and the current study used only one step of DR (33% decrease of the normal dose) instead of 2 steps (50% decrease of the normal dose). The reason for this adaptation was that, in our early experience with the CONDOR study, the majority of patients successfully achieved this first step of DR. Furthermore, one step is more practical. It might be easier to convince patients to decrease their biologic dose by only 33%. In this clinical evaluation, a similar proportion of patients used a lower biologic dose after 1 year compared with the trial: 67% vs 68% in the trial. The mean cumulative dose used in 1 year was less reduced than in CONDOR, which can be explained by the adapted strategy. With the final results of CONDOR we now know that 34% of patients achieved the second step of DR to 50% of the original dose (1). Therefore, if one-step DR is successful, a further decrease should be discussed with the patient.
In line with these results, previous studies indicated that DR of biologics for psoriasis is possible. In these studies, patients could also reduce their dose after approximately 6 months and in case of low disease activity, but success rates ranged from 22% to 90% depending on the definition of success and the study design (2–5). The current evaluation differs from previous studies, as it prospectively evaluated a modified, tightly controlled strategy from a recently conducted RCT (1). We believe that tight control is needed in order to safely determine the lowest effective dose. Moreover, this study elucidates the investments needed to perform DR on a standard basis in clinical practice. A dedicated nurse was provided to support physicians and patients. This made it possible to collect data and it improved applicability of the strategy. The nurse screened all patients visiting our biologic outpatient clinic, with a time investment of 1 h per 16 patients. Of all 498 visiting patients, 85 eventually started DR, resulting in a number needed to screen of 5.9 patients. Of 498 patients however, most patients were not eligible, as they did not use a biologic yet, had unstable disease, or used another biologic. Patients needed to be screened several times, as disease activity could become stable over time. This requires time investment. Installing a dedicated nurse or physician could contribute to the success of a new strategy, as coaching of patients is needed. Of the patients who stopped DR, 66% had a PASI and/or DLQI ≤ 5, and reduced effectiveness experienced by the patient, while not experienced by the physician, contributed the most among reasons for stopping DR. It was possible for patients to stop DR on their request due to several reasons, such as fear of disease flare. On the other hand, one patient wanted to start DR with a PASI > 5. Four patients continued DR despite PASI > 5. Personalizing treatment goals and coaching of patients therefore seems important when considering DR.
Currently, the possibility of DR is mentioned in only a few published national guidelines (15, 16). No clear protocols are available yet. A tightly controlled strategy, guided by disease activity and QoL, seems safe for daily use and allows evaluation of the success of the strategy. In the current strategy we used a PASI and/or DLQI score ≤ 5 as target for starting and continuing DR. It can be questioned whether this is the correct target, as in the field of psoriasis different treatment targets were defined in recent years. For example, the National Psoriasis Foundation defined their therapeutic goal as a body surface area of 1% or less (17), while a Spanish group recommended a PASI 90 or Physicians’ Global Assessment (PGA) ≤ 1, with a DLQI ≤ 1, and prolonged remission without loss of response and worsening of comorbidities (18). In Belgium, the target was multidimensional, including multiple criteria, such as disease activity, itch, DLQI, daily functioning and safety (19). Mahil et al. (20) recently stated that PASI ≤ 2 and PGA clear/almost clear are relevant for treat to target strategies. In our opinion however, not only disease activity, but also QoL, should be taken into account, as it might differ among patients as to which PASI scores are acceptable (21). Therefore a low DLQI was a prerequisite, apart from PASI. Moreover, PASI is difficult to assess at lower score levels (22). Some patients with higher PASIs may still have limited disease activity and DLQI may be informative in this context.
A limitation of this evaluation is the study length in the context of long-term gains and risks of DR. However, in the current evaluation no safety issues related to DR occurred. Furthermore, 7/8 patients with PASI > 5 during the analysis period regained PASI < 5 within 6 months. Only 2 patients discontinued DR due to an increase in joint complaints, with one patient having PsA. The outcomes of DR regarding other inflammatory comorbidities were not assessed, although, according to clinical practice, DR was reconsidered in case of worsening of such comorbidities. Studying the effect of DR on comorbidities specifically is for future research. In line with the current results, previous studies did not report safety issues related to DR, despite follow-up might not have been long enough for assessing all adverse outcomes (23). The long-term extension results of our previous RCT showed a temporary, small increase in PASI scores, which decreased again after 18 months (24). No patients who failed on DR needed to switch treatment within 24 months of follow-up, as treatment responses were regained by re-installing the normal dose. Impact on QoL remained low and there were no safety signals, including symptoms related to anti-drug antibody formation (24). Another study found no difference in development of anti-drug antibodies of ustekinumab between patients on a reduced dose vs the normal dose (4). It should be emphasized that, by striving for tight control, timely dose adjustments can lead to re-achievement of adequate treatment responses, hence limiting long-term safety risks. Still, more long-term data regarding DR is needed in order to provide insight into longer term risks and benefits.
A further limitation of the current study is that it did not analyse the use of topical steroids or other health-related costs. Consequently, indirect costs related to DR could not be calculated. In our previous RCT, more patients in the DR group used topical steroids compared with the usual care group, and healthcare usage was higher (1, 25). However, the DR strategy resulted in substantial cost savings, with a minimal reduction in quality-adjusted life years.
In our opinion, this clinical evaluation shows that a pragmatic, one-step DR strategy of adalimumab, etanercept and ustekinumab for psoriasis is possible in daily practice. Seventy-eight percent of eligible patients started DR. Two-thirds of patients who started DR at least 1 year ago were still on a lower dose after 1 year, without safety concerns. Although it requires some time investment, the study showed that even a one-step DR strategy has considerable potential to lower cumulative biologic doses with lowering of healthcare costs, without deterioration of psoriasis. More daily practice studies with longer follow-up of patients could contribute to accumulation of evidence regarding biologic DR.
This study is co-funded by Dutch Healthcare Insurance Company VGZ.
Conflict of interest. SA reported grants from Janssen Pharmaceuticals, Abbvie, Celgene and Novartis and congress fee from Celgene. LSvdS carries out clinical trials for Janssen and Novartis. LJvV carries out clinical trials for AbbVie, Celgene, Janssen and Novartis. JMPAvdR carries out clinical trials for AbbVie, Celgene and Janssen; has received speaking fees/attended advisory boards from AbbVie, BMS, Almirall and Janssen and has received reimbursement for attending a symposium from Celgene and AbbVie. EMGJdJ has received research grants for the independent research fund of the Department of Dermatology of Radboud University Medical Center Nijmegen, the Netherlands from AbbVie, Pfizer, Novartis, Janssen Pharmaceuticals and Leo Pharma and has acted as consultant and/or paid speaker for and/or participated in research sponsored by companies that manufacture drugs used for the treatment of psoriasis including AbbVie, Janssen Pharmaceutica, Novartis, Lily, Celgene, Leo Pharma, UCB and Almirall. None of the above-mentioned funding is personal, but goes to the independent Research Fund of the Department of Dermatology of Radboud University Medical Center Nijmegen (Radboudumc), The Netherlands. The other authors have no conflict of interests to declare.


 Click to show fullsize
Click to show fullsize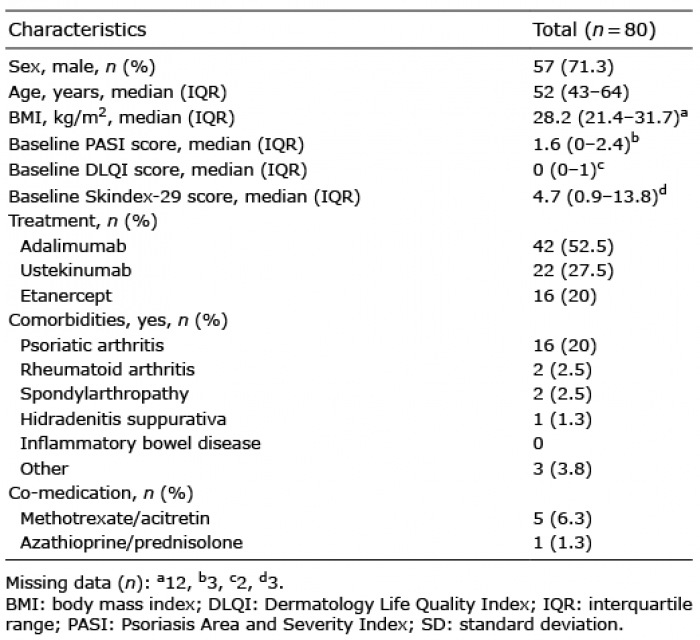 Click to show fullsize
Click to show fullsize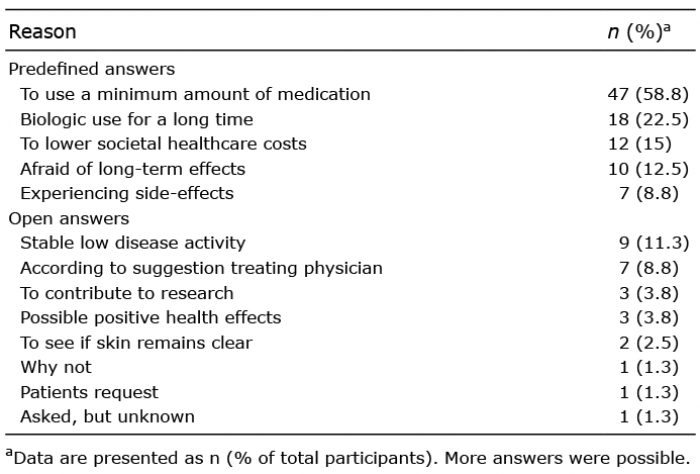 Click to show fullsize
Click to show fullsize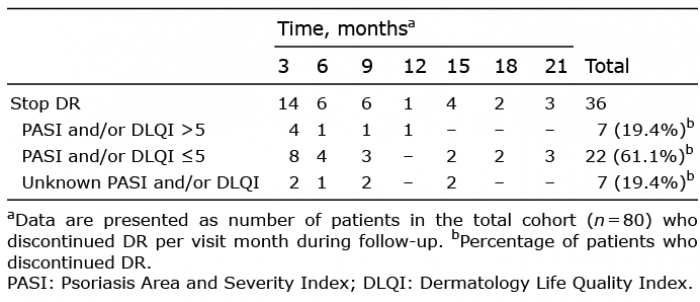 Click to show fullsize
Click to show fullsize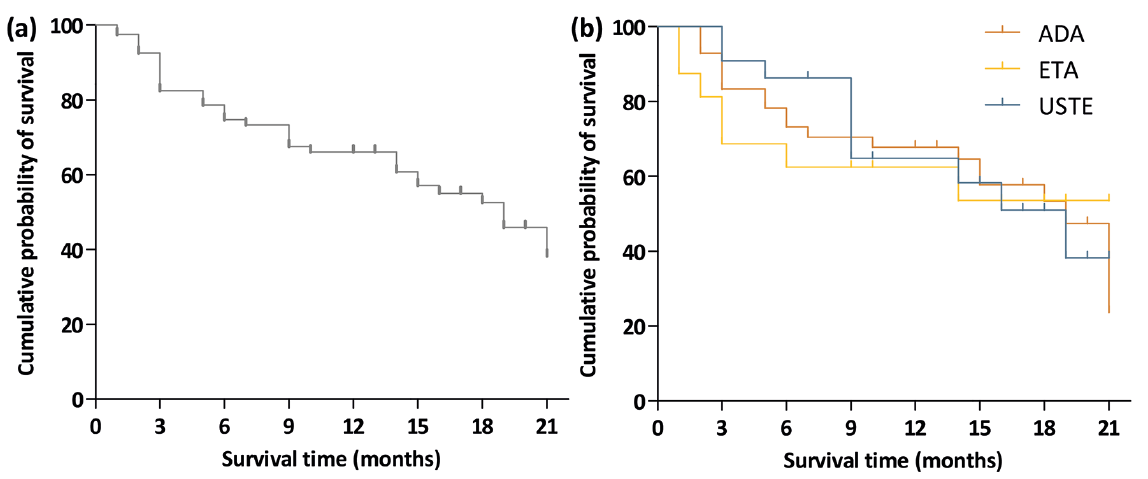 Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize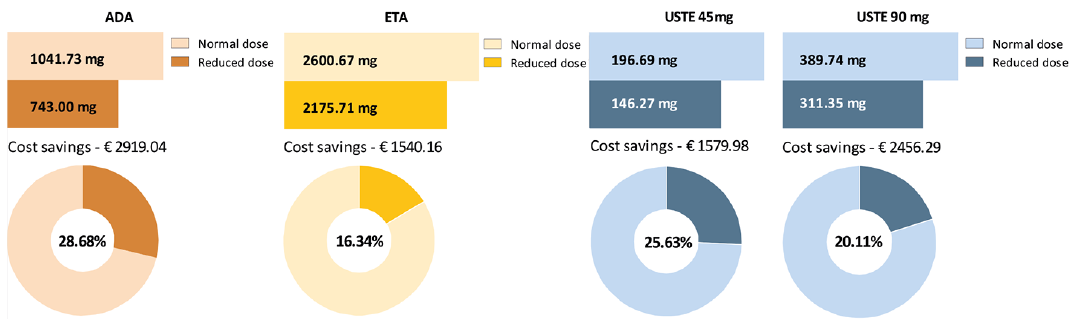 Click to show fullsize
Click to show fullsize