


1Department of Dermatology, University Hospital Münster, Münster, 2Dermatologikum Hamburg, Hamburg, and 3Department of Dermatology, Medical Faculty, Heinrich Heine University, Düsseldorf, Germany
The histopathology of psoriasis can lack classical features on certain anatomical sites. The aim of this study was to detail the histopathology and immunophenotype of psoriasis on the legs, in order to differentiate it from other inflammatory dermatoses, such as stasis dermatitis. The histopathology of psoriasis on the legs was retrospectively compared with psoriasis on the trunk and stasis dermatitis. Statistically, psoriasis on the legs was significantly less likely to show typical histological criteria of psoriasis, such as regular hyperplasia, suprapapillary thinning, and “kissing vessels”. The most valuable criteria to distinguish psoriasis on the legs from stasis dermatitis were the presence of neutrophils in the cornified layer and staggered parakeratosis. In addition, an immunohistochemical panel (Ki-67, Bcl-2alpha, S100A7, CD3, MPO, CK10, CK16) revealed that staining with Ki-67 and MPO could be diagnostically useful. Since the cornified layer contains important histopathological clues to differentiate psoriasis on the legs from stasis dermatitis, clinicians should refrain from unnecessary rubbing during disinfection before taking a biopsy.
Key words: dermatopathology; extremities; leg; psoriasis.
Accepted Apr 29, 2021; Epub ahead of print Apr 30, 2021
Acta Derm Venereol 2021; 101: adv00453.
doi: 10.2340/00015555-3817
Corr: Stephan A. Braun, Department of Dermatology, University Hospital Münster, Von-Esmarch-Straße 58, DE-48149 Münster, Germany. E-mail: stephanalexander.braun@ukmuenster.de
Diagnosis of psoriasis is usually made clinically, but in some cases clinicians take biopsies to confirm the diagnosis or to exclude differential diagnoses. Psoriasis on the lower extremities can lack classical histological criteria of psoriasis, and therefore histological diagnosis can be challenging at this specific anatomical site. This study systematically analysed the histology, including the immunohistochemistry, of psoriasis on the legs, and identified characteristic criteria for this location. The results help to improve the histological diagnostic reliability of psoriasis on the legs, and provide practical information for clinicians on what to consider when taking biopsies.
Psoriasis has a prevalence of 2–3%, and is one of the most common, chronic inflammatory skin diseases in Germany (1). Psoriasis is usually a clinical diagnosis, but, in some cases, biopsies are needed to confirm the diagnosis or to exclude differential diagnoses. These include, for example, eruptive stages of psoriasis, erythrodermic courses, pustular forms, and manifestations of psoriasis in specific anatomical locations, such as the scalp, palms and soles and the intertriginous areas. However, in cases with an unclear clinical picture, histological diagnosis can also be a challenge, thus the histological report often ends up with the same differential diagnoses.
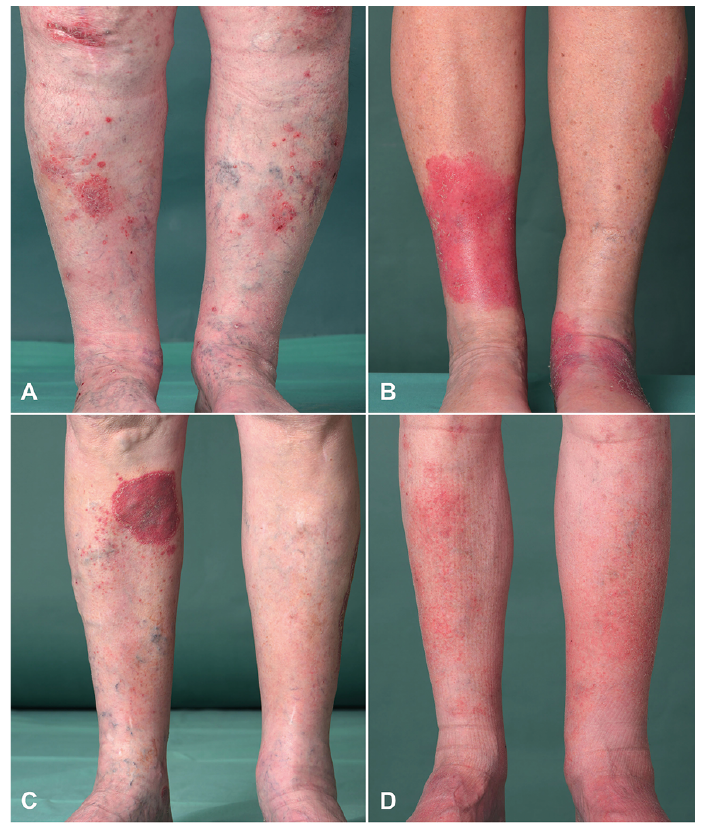
This diagnostic dilemma also occurs with psoriasis on the lower extremities. Psoriasis on the legs sometimes manifests only at this location, and presents with atypical morphology (Fig. 1), and/or appears refractory to therapy. Biopsies are therefore frequently taken to exclude other inflammatory diseases, such as chronic (nummular) eczema or stasis dermatitis. We observe that this problem occurs particularly in patients who have additional stasis due to, for example, chronic venous insufficiency (CVI).
Fig. 1. Clinical pictures of patients with (A–C) psoriasis on the lower extremities and (D) stasis dermatitis included in this study.
Although renowned dermatopathologists, such as Ackermann (2), have stated that the histology of psoriasis on the lower extremities differs from that on other anatomical sites, to date, to the best of our knowledge, there exists no systematic analysis of the histology of psoriasis on the legs. However, previous studies have shown that, by systematically examining psoriasis at a particular site, site-specific diagnostic clues could be identified (3, 4). The aim of the current study was therefore to achieve a more objective understanding of the morphological and immunophenotypical characteristics of psoriasis on the lower extremities. The results should help to improve the diagnostic reliability of psoriasis on the legs.
This study therefore: systematically analysed 39 biopsies of psoriasis on the lower extremities and compared them with 36 lesions of classical plaque-psoriasis of the trunk to identify characteristic morphological criteria of psoriasis on the legs; evaluated the influence of CVI on the histology; and looked for criteria to distinguish psoriasis on the legs from stasis dermatitis. In addition, this study evaluated a broad panel of immunohistochemical markers, including markers of myeloid (MPO), lymphoid (CD3) lineage, epidermal differentiation (CK10, CK16), proliferation and apoptosis (S100A7, Ki-67, Bcl-2alpha).
Material
Retrospectively, histopathological slides of over 200 archived biopsies of psoriasis on the lower extremities and the trunk were identified. The skin biopsies were obtained by punch biopsy during the fully developed stage of the skin eruption and were stained with haematoxylin and eosin (H&E) and periodic acid-Schiff (PAS). The diagnosis of psoriasis vulgaris was confirmed by additional clinical information (family history of psoriasis, typical psoriatic skin manifestation, psoriatic nail changes, presence of psoriatic arthritis, response to anti-psoriatic therapy), which was obtained from the clinical records and clinical pictures, which were available for all patients at the Department of Dermatology, University Hospital Münster, Germany. Biopsies that did not meet these criteria were excluded. In addition, biopsies of stasis dermatitis due to CVI were identified. The diagnosis was ensured by clinical images and the clinical record. To be included, the patients had to show the typical clinical picture of stasis dermatitis (extensive, eczematous skin lesions on the lower legs) and a CVI minimum stage I (classified according to Hach (5)) proven by ultrasound, and no documented clinical evidence for psoriasis.
Finally, 90 biopsies of 87 patients taken during the period 2011 to 2019 were enrolled in the study. Thirty-nine biopsies referred to the group “psoriasis leg (PL)”, 36 to the group “’psoriasis trunk (PT)”’, and 15 to the group “’stasis dermatitis (StD)”. In order to investigate the influence of CVI on PL, PL was divided into 2 subgroups: (i) psoriasis of the leg with clinically and sonographically documented second diagnosis of CVI minimum stage I (Hach) (PLS/ n = 15); and (ii) psoriasis of the leg without clinically documented evidence for CVI, referred to psoriasis not otherwise specified (PLNOS/ n = 24). The study was conducted in accordance with the Declaration of Helsinki and was approved by the local ethics committee (# 2019-546-f-S).
Histological analysis
A list of 64 histopathological criteria was compiled, including classical and non-classical (6) findings in psoriasis. Also, criteria of typical differential diagnoses for psoriasis on the leg, such as lichen simplex chronicus and stasis dermatitis, were added. The complete list of investigated criteria is shown in Table I.
Table I. List of analysed histopathological criteria
All 75 biopsies of psoriasis were systematically assessed for the 64 criteria on H&E-stained slides. The presence of fungi was evaluated by PAS staining. For the analysis of the biopsies of StD a reduced list of 13 key criteria was used. The presence or absence of histopathological features was documented with a semi-quantitative score: 1 = strongly present, 2 = present, 3 = weakly present, 4 = not present, 5 = not assessable. In addition, hyperplasia of the epidermis was measured quantitatively with an ocular micrometre, and the following score was defined: > 0.4 mm = strongly present, 0.4–0.2 mm = present, < 0.2 mm = weakly present. The histological evaluation was conducted by 2 experienced dermatopathologists (MF, DM). In the case of discrepancies between the 2 observers, the cases were discussed until consensus.
Immunohistochemistry
Immunohistochemistry was performed on 8 randomly selected cases of each group (PT, PL, StD). The staining was performed on 3-μm thick paraffin-embedded tissue sections. After deparaffinization and rehydrating with distilled water “Heat Induced Epitope Retrieval”’ was performed with respective buffers (Ki-67, Bcl-2alpha, S100A7: citrate buffer pH 6.1(DCS, Hamburg, Germany), CD3: EDTA buffer pH 8.0 (DCS), MPO: EDTA buffer pH 9.1 (DCS)). For CK10 no epitope retrieval was done. The following antibodies were used in respective dilutions: Ki-67 (clone Mib-1; Agilent, Santa Clara, USA; 1:50 in DCS dilution buffer); Bcl-2alpha (clone 100/D5; Agilent, Santa Clara, USA; 1:400 in DCS dilution buffer); CK10 (clone DE-K10; Agilent, Santa Clara, USA; 1:100 in DCS dilution buffer); CK16 (clone LL025; Abcam, Cambridge, UK; 1:150 in DCS dilution buffer); S100A7 (clone 47C1068; Abcam, Cambridge, UK; 1:4000 in DCS dilution buffer); MPO (polyclonal; Agilent, Santa Clara, USA; 1:20000 in Agilent dilution buffer); CD3 (polyclonal; Agilent, Santa Clara, USA; 1:500 in DCS dilution buffer). For detection, the DetectionLine PolyLink-HRP-Kit (DCS, Hamburg, Germany) was used with 3-Amino-9-ethylcarabzol (ACE) (ACE 2 Component/Chromogen Kit, DCS, Hamburg, Germany). Counterstaining was performed with haematoxylin after Mayer and slides were mounted with Aquatex (Merck, Darmstadt, Germany).
Assessment of Ki-67 and Bcl-2alpha was done by counting positive nuclei per millimetre in keratinocytes of the basal and supra-basal layer (mean of 3 measurements). Expression of CK10 and CK 16 were evaluated in 2 ways. Firstly, the distribution was scored on a 3-point scale: 0 = absent; 1 = patchy; 2 = continuous. Secondly, the positive stained area of the epidermis, which was expressed as the ratio of the total thickness of the epidermis in a rete ridge divided by the thickness of the area stained positive for CK10 or CK16, was assessed (mean of 3 measurements). S100A7 staining was analysed on a 4-point scale: 0: absent; 1: weak, only cytoplasmatic; 2: moderate, cytoplasmatic and few positive nuclei, 3: strong, cytoplasmatic and abundant nuclear positivity. MPO- and CD3-staining was evaluated in 3 epidermal layers (stratum corneum; stratum granulosum/stratum spinosum/stratum basale; subepidermal), and the presence postive stained cells was scored with a 3-point scale: 0: absent, 1: few present, 2: moderate present, 3: abundant present. Immunohistological assessment was conducted independently by 2 dermatopathologists (MF, SAB). The mean values of the 2 investigators were used for statistical analyses.
Statistical data analyses
Categorical and ordinal variables are expressed as frequency and percentage, whereas continuous variables are presented as mean ± standard deviation (SD) and range. Statistical analyses were performed with IBM SPSS Statistics, Version 26.0. (2019, Armonk, NY: IBM Corp). The χ2 test or Fisher’s exact test was used for comparison of categorical parameters of independent study groups, the Mann–Whitney U for comparison continuous and ordinal parameters of 2 independent study groups. Statistical significance was assumed at p < 0.05 (2-sided).
Demographic characteristics of the study population
A total of 90 biopsies of 87 patients were included in the study, of which 42 (46.7%) were biopsies from female patients and 48 (53.3%) from male patients. The mean age of the patients was 62 years (range 12–89 years), with an even distribution of age between the 3 groups: “psoriasis on the leg (PL)”, “psoriasis on the trunk (PT)” and “stasis dermatitis (StD)”. At 69% the male sex was slightly over-represented in the PT group. The clinical information is summarized in Table II.
Table II. Demographic and clinical characteristics of the study population
Histopathology of psoriasis on the leg shows significant differences from psoriasis on the trunk
First, the study compared cases of psoriasis on the leg (PL) with those of psoriasis on the trunk (PT) to identify histological differences depending on anatomical site. PL and PT had many epidermal changes in classical psoriasis in common: hyperkeratosis, compact cornified layer, parakeratosis, neutrophils in cornified layer, absent stratum granulosum, club-shaped rete ridges, thin rete ridges, spongiosis, intraepidermal neutrophils, basal and suprabasal mitoses. In addition, the presence of some non-classical criteria of psoriasis, such as prominent stratum granulosum, necrotic keratinocytes, vacuoles at the dermo–epidermal junction, subepidermal colloid bodies, intraepidermal erythrocytes, and other scratch-related changes showed no significant difference between leg and trunk. Pustules were identified in only 8 cases; therefore, no further statistical analysis of this criterion was performed.
The study could identify 13 statistically significant epidermal and dermal differences. The most striking and highly significant difference referred to the quantitative measurement of epidermal hyperplasia (p < 0.001). In PT epidermal hyperplasia was “strongly present” (> 0.4 mm) in 50% of examined cases, in PL only 21% of examined cases showed prominent hyperplasia and, in 28% of the cases, hyperplasia was only weakly present. In addition to quantitative differences, qualitative differences could also be identified. The hyperplasia of PL was significantly less regular compared with that of PT (46% in PL vs 69% in PT, p = 0.042). Another highly significant difference was suprapapillary thinning (p < 0.001), which was less detectable in PL (51%) compared with PT (97%). In the latter, it was missing in only one case. Also, the number of intraepidermal lymphocytes was significantly lower in cases of PL compared with PT (p = 0.04).
In the dermis deep perivascular inflammation (p = 0.003) and inflammation around sweat glands (p = 0.03) were significantly more common in PL compared with PT. In addition, highly significant increases in the number of vessels in the papillary (p = 0.003) and the reticular dermis (p < 0.001) were identified in PL. Furthermore, the capillaries in the papillary body showed significantly less close contact with the basal membrane (“kissing vessels”) (p = 0.009). Moreover, the thickness of vessels walls in the papillary dermis (p < 0.001), deep dermis (p < 0.001), and subcutis (p = 0.04) was also increased. In addition, papillary oedema (p < 0.001) was significantly less common in PL. The complete histopathological analysis of investigated criteria including statistical analysis is shown in Table III. Fig. 2 shows typical histological examples of PT and PL.
Table III. Histopathological analysis of psoriasis on the leg (PL) vs psoriasis on the trunk (PT)
Fig. 2. Histopathology of psoriasis and stasis dermatitis. (A, B) Classical criteria of psoriasis on the trunk; (C–F) representative examples of psoriasis on the legs. Particularly noteworthy is a weak hyperplasia, the lack of elongated rete ridges, and the presence of staggered parakeratosis. (G, H) Stasis dermatitis lacking staggered parakeratosis, which is highly specific for psoriasis. (Haematoxylin-eosin staining: C, E, G, H 40×; A, B, D, F 100×).
To sum up, the histopathology of PL compared with PT less often shows hyperplasia of the epidermis, and, if it does, it is more irregular and lacks typical suprapapillary thinning and “kissing vessels”. The number and thickness of dermal vessels are much more prominent in cases of PL.
Histopathology of psoriasis on the leg with vs without chronic venous insufficiency shows no significant differences
In a next step, it was evaluated whether stasis due to CVI is responsible for the identified characteristic difference in PL. Therefore, a selection of key criteria (Table IV) were compared between the 2 subgroups: PL with an additional diagnosis of CVI (PLS) (n = 15) and PL with no documented CVI (PLNOS) (n = 25). Statistical analysis found no significant differences between the 2 groups (see Table IV). An increased number of vessels in the papillary dermis was detected more frequently in PLS, but did not reach statistical significance.
Table IV. Histopathological analysis of psoriasis on the leg with vs without chronic venous insufficiency (CVI) and compared with stasis dermatitis
Histopathology of psoriasis on the leg with chronic venous insufficiency differs significantly from stasis dermatitis
In a third analysis, the study compared PLS with StD, intending to identify criteria to better discriminate the 2 inflammatory diseases. Again, this focused on a subset of key criteria (see Table IV).
In total, this study identified 6 significant differences between the 2 groups. PLS showed highly significant, more often staggered, parakeratosis (p < 0.001) and neutrophils in the cornified layer (p = 0.002). Close contact of papillary vessels with basal keratinocytes (“kissing vessels”) (p < 0.001) and thinning of the suprapapillary plates of the epidermis (p = 0.005) were also highly significantly more common in PLS compared with StD. Thick-walled vessels in the papillary dermis (p = 0.007) and papillary oedema (p = 0.005) were significantly more frequent in cases of StD. Other analysed criteria, such as epidermal hyperplasia, confluent parakeratosis, vertical streaks, fibrosis in the reticular dermis, number of vessels did not show any significant differences. The complete analysis of investigated criteria including statistical analysis is summarized in Table IV. Fig. 2 shows typical histological examples of StD.
Immunohistochemical markers show significant differences between psoriasis on the trunk and leg and between psoriasis on the leg and stasis dermatitis
Finally, it was investigated whether there are differences in the expression of typical immunohistochemical markers for psoriasis between PT and PL and PL and StD. Table V shows the list of the analysed markers. The expression ratio of cytokeratin (CK) 10 was significantly increased in PL compared with PT (p = 0.002), which means that the expression of the differentiation-marker CK10 starts later in higher epithelial layers in PL. Expression of the antimicrobial peptide psoriasin (S100A7) was significantly increased (p = 0.041). In addition, Bcl-2alpha expression was reduced in PL compared with PT (p = 0.035). No other markers showed significant differences.
Table V. Immunohistochemical analysis of psoriasis on the trunk (PT), psoriasis on the leg (PL) and stasis dermatitis (StD)
Furthermore, this study investigated whether immunohistochemical markers may be helpful to better differentiate PL from StD. Notably, several significant differences could be identified. In PL the proliferation rate of basal and suprabasal keratinocytes, measured with the proliferation marker Ki-67, was significantly higher (p = 0.010) (Fig. 3C, D). Moreover, the expression of S100A7 was increased in PL (p = 0.001) (Fig. 3E, F). Staining neutrophils with MPO confirmed our morphological results. Significantly more neutrophils could be identified in the cornified layer of patients with psoriasis compared with those with stasis dermatitis (p = 0.006) (Fig. 3G, H). A significant difference could also be identified in the expression of CK16 between the 2 groups. Expression of CK16 was decreased in StD (p = 0.015). The complete analysis is shown in Table V.
Fig. 3. Immunophenotypic differences between psoriasis on the leg (PL) and stasis dermatitis (StD). (A, C, E, G) representative case of PL and (B, D, F, H) of StD. The proliferative activity of basal, and especially suprabasal, keratinocytes, measured with Ki-67, was significantly higher in PL (C), compared with StD (D). In addition, expression of psoriasin (S100A7) was stronger in PL (E). MPO staining could be useful to unmask neutrophils within parakeratosis of PL (G), which were absent in most cases of StD (H) (staining: A, B: haematoxylin-eosin; C, D: Ki-67; E, F S100A7; G, H: MPO; original magnification: A, B 40×; C–H 100×).
As already mentioned in the introduction, histopathological diagnosis of psoriasis normally does not pose a problem when biopsies are taken from classical lesions. The characteristic histological criteria of psoriasis can be found in all common textbooks (7–11). However, when biopsies are taken from special sites, like the scalp, palms, and soles or the intertriginous area, the histology may differ significantly from the classical pattern. Although some textbooks indicate that the histology of psoriasis differs depending on the anatomical localization (11), very few studies have systematically investigated these differences. For example, there are 2 studies, which have analysed morphological characteristics of scalp psoriasis and identified helpful criteria to distinguish scalp psoriasis from seborrhoeic dermatitis (12). A few studies have focused on the distinction between palmar psoriasis and eczema (13–15). In 1974 Uehara & Ofuji (15) published a small case series of 10 patients with psoriasis palmaris and plantaris and described spongiosis with lymphocytic exocytosis as an important initial finding. In a more recent study, Park et al. (13) demonstrated that loss of the granular layer was more consistent with a diagnosis of psoriasis palmaris.
The current systematic analysis confirms that histopathology of psoriasis on the leg also differs significantly from classical psoriatic lesions. PL showed most of the classical histological features of psoriasis. However, some key features, such as regular epithelial hyperplasia, suprapapillary thinning, and “kissing vessels”, were significantly often lacking. These findings are in line with Ackerman’s comment, who stated that psoriasis on the leg is less psoriasiform (2).
Ackerman (2) also noted that the altered pattern on the leg is seen mainly in psoriatic patients with additional stasis. However, our subanalysis of PL comparing patients with and without CVI, did not detect significant differences between the 2 groups. Assuming that CVI is associated with increased stasis, one could conclude that stasis is not a decisive factor for histological differences. However, our findings should be considered with caution. Firstly, we cannot exclude that there were also patients with CVI in our PLNOS group. The classification of groups was based solely on clinical documentation. Some patients in the PLNOS group also had histological evidence of CVI, such as fibrosis of the connective tissue and increased vessel wall thickness. Secondly, the term stasis is not precisely defined. There may be other factors, such as obesity, that were not considered in the classification of the 2 subgroups and therefore could bias the result. Thus, our subanalysis is not sufficient to draw a firm conclusion. For a clearer picture of the influence of stasis on the histopathology of psoriasis on the leg, further studies with better defined groups are needed.
In addition, this study confirmed that PL also shows many overlapping histological criteria with StD, such as confluent parakeratosis, spongiosis, and proliferation of vessels with thickened walls. Due to the additional absence of classical psoriasis criteria in PL, it can become difficult to distinguish the 2 diseases histologically. In our analysis, however, we were able to identify important diagnostic clues to distinguish between the 2 diagnoses. The presence of neutrophils in the cornified layer, staggered parakeratosis, suprapapillary thinning, and “kissing vessels” were the most useful diagnostic criteria to favour the diagnosis psoriasis. Neutrophils in the cornified layer were present in 82% and staggered parakeratosis in 90% of cases of PLS in the current study, whereas both criteria were found in only 20% of cases with StD. Since neutrophils may also be increased in eczema due to superinfection, we consider staggered parakeratosis to be the most important clue for distinguishing psoriasis from eczema on the lower legs.
The current study also showed that PL differs significantly from PT in the expression of common immunohistological markers for psoriasis. An increased Ki-67 rate accompanied by a significantly decreased expression of the anti-apoptotic marker Bcl-2alpha indicated a higher proliferation rate of basal keratinocytes in PL compared with PT. In addition, expression of S100A7 was significantly increased in PL. These findings were in line with a reduced staining for the differentiation-marker CK10 in the stratum corneum in PL compared with in PT. It is notable that the higher proliferative activity and de-differentiation of keratinocytes in PL seems not to result in an increased hyperplasia. This indicates that there may be independent site-specific factors that may also influence the development of acanthosis. Notably, as it is diagnostically useful, significant differences in immunological markers between PL and StD were identified. Although we have identified significant differences for several markers (S100A7, CK16, Ki-67 and MPO in the stratum corneum), we consider that, in particular, Ki-67 could be very helpful, since it is a marker that is frequently used in routine diagnostics. The proliferation rate of basal keratinocytes in PL, measured with Ki-67, was significantly increased compared with StD. The utility of Ki-67 to differentiate psoriasis from eczematous dermatitis has been described previously (16). In particular, a high rate of positive cells in the suprabasal layers is indicative for psoriasis (16) (Fig. 3C). Therefore, in selected cases, additional immunohistochemical staining with Ki-67 could also be useful to differentiate PL from StD. Staining with MPO could be helpful to identify isolated neutrophils in the stratum corneum that are otherwise missed in H&E staining (Fig. 3G). However, the expression of the studied markers is highly dependent on the stage of the disease, the location of the biopsy and, in particular, for antimicrobial proteins, such as S100A7, on factors like superinfection and skin barrier disruption (17–19). The immunohistochemical analysis is therefore limited, particularly due to the small number of cases.
In conclusion, what do the findings add to everyday dermatological work? Histopathology can contribute to the diagnosis of psoriasis on the lower extremities, and therefore biopsies are helpful. Yet, for a valid histological statement, dermatopathologists must consider that psoriasis on the leg may have less regular hyperplasia, less suprapapillary thinning, and fewer “kissing vessels”. The absence of these criteria should not exclude the diagnosis of psoriasis. The simultaneous presence of both neutrophils in the cornified layer and staggered parakeratosis are highly specific and diagnostic for psoriasis and are the most valuable criteria to distinguish psoriasis from other inflammatory diseases on the lower extremities, in particular stasis dermatitis. In borderline cases, immunohistochemical staining especially with the widely used markers Ki-67 and MPO may add additional pieces of the diagnostic puzzle. Since the cornified layer is essential for evaluation, clinicians should be aware that when taking a biopsy on the lower leg of a scaling lesion, it is crucial to ensure that the cornified layer is not removed by unnecessary disinfection and rubbing.
The authors thank Andrea Wissel, Veronika Haase, Franziska Kottenstede, Petra Neuhaus, and Birgit Strotbaum for their excellent technical assistance and Sebastian Schmitz for the preparation of the figures.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize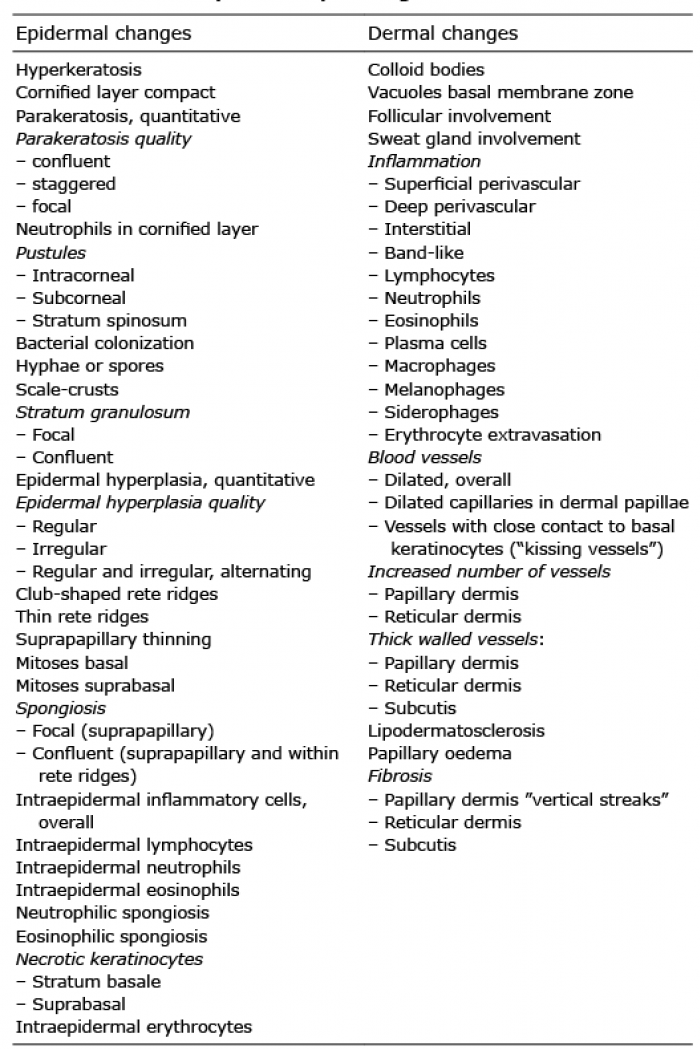 Click to show fullsize
Click to show fullsize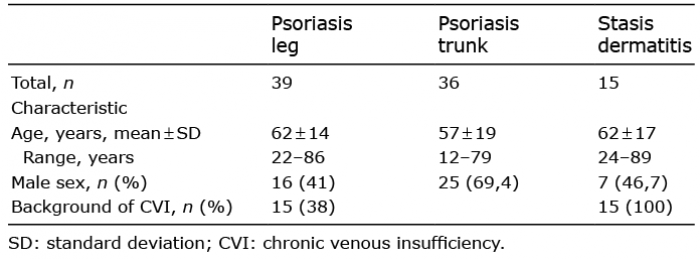 Click to show fullsize
Click to show fullsize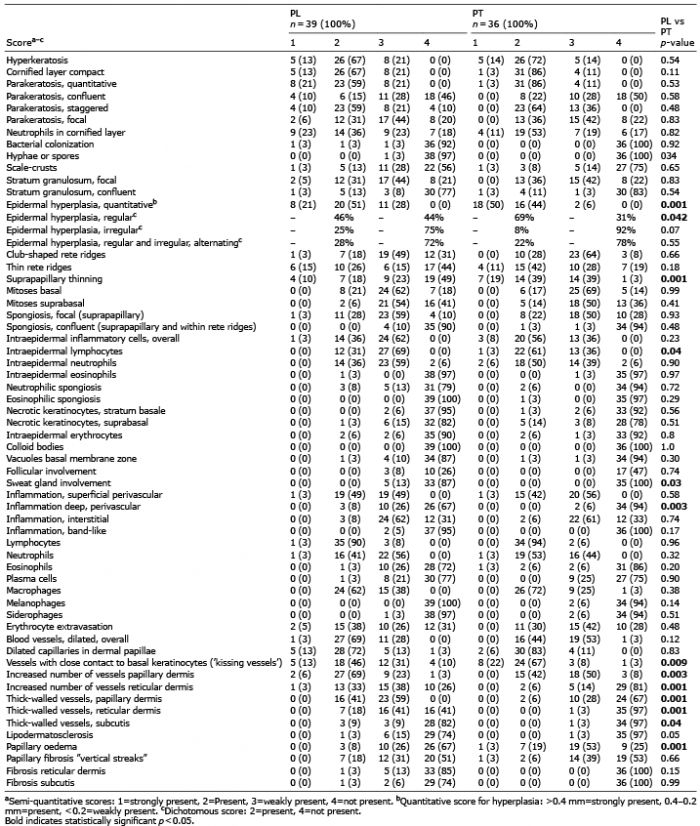 Click to show fullsize
Click to show fullsize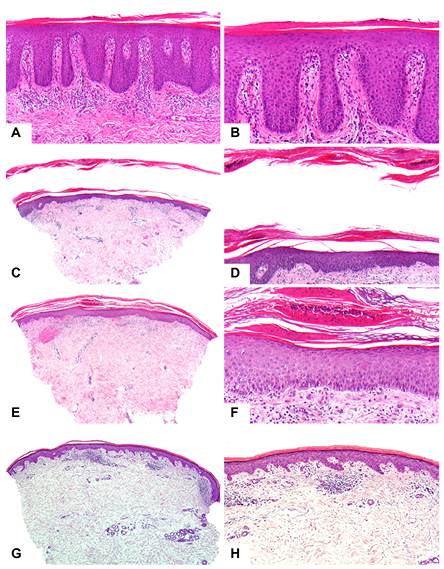 Click to show fullsize
Click to show fullsize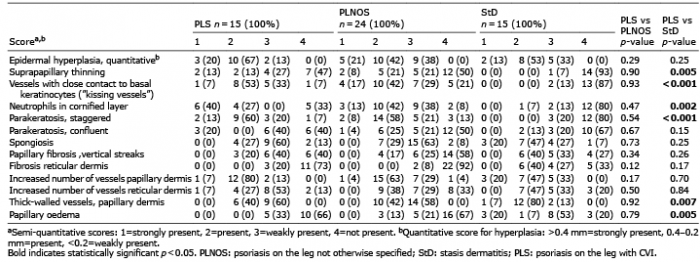 Click to show fullsize
Click to show fullsize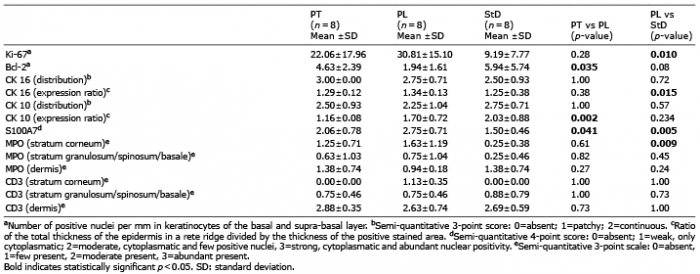 Click to show fullsize
Click to show fullsize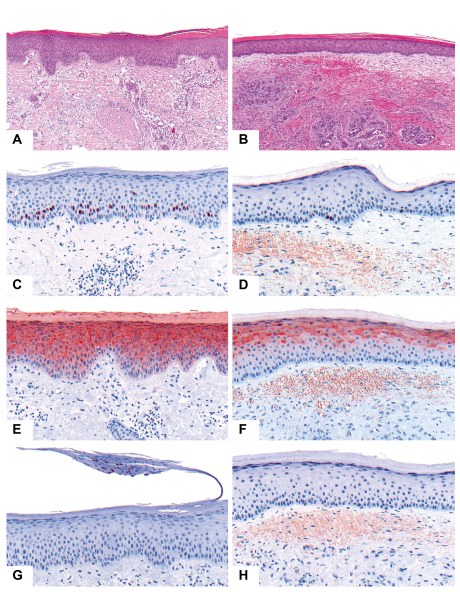 Click to show fullsize
Click to show fullsize