


1Department of infectious Diseases, 2Institute of Photomedicine, 3Department of Pathology, Shanghai Skin Disease Hospital, Tongji University School of Medicine, and 4Shanghai Skin Disease Hospital, Clinical School of Anhui Medical University, Shanghai, China
Leprosy is a chronic infectious disease caused by Mycobacterium leprae. Massive internal migration from rural to urban areas poses new challenges for leprosy control in Shanghai, China. This retrospective epidemiological study examined new cases of leprosy diagnosed in Shanghai from 2000 to 2019, with emphasis on internal migration cases. There were 145 cases of leprosy in the study period; the majority of cases (89.0%) were internal migrants. Migrant cases had a mean of 25.4 months lag time from onset of symptoms to diagnosis, which was significantly longer than that of resident cases (mean 10.8 months, p < 0.001). Greater lag time from the first visit to diagnosis was observed in migrant cases (mean 23.2 months) compared with resident cases (mean 9.4 months, p < 0.001). A large majority of cases (91.0%) had been misdiagnosed. Internal migrant cases were responsible for most incidences of leprosy in Shanghai. They often did not receive timely diagnosis and treatment, which may have an adverse impact on the prevention of epidemic leprosy.
Key words: leprosy; internal migration; public health; epidemiology.
Accepted May 5, 2021; Epub ahead of print May 6, 2021
Acta Derm Venereol 2021; 101: adv00459.
doi: 10.2340/00015555-3821
Corr: Pingyu Zhou and Zhichun Jing, Department of Infectious Diseases, Shanghai Skin Disease Hospital, Tongji University School of Medicine, 1278 Baode Road, Shanghai 200443, China. E-mail: 743835016@qq.com; 35476451@qq.com
Internal migration of people from rural to urban areas in search of opportunities and better living is common in China. This migration may lead to an increased burden of leprosy in Shanghai urban areas. This study examines the cases of leprosy diagnosed in Shanghai, and compares the differences between indigenous cases of leprosy and cases in internal immigrants. Internal migrant cases were found to be responsible for most incidences of leprosy in Shanghai. Misdiagnosis was the main reason for delays in diagnosis of leprosy. Internal migrant cases of leprosy had a longer delay in diagnosis than resident cases.
Leprosy is a chronic infectious disease caused by Mycobacterium leprae. Leprosy mainly affects the skin and peripheral nervous system, and may lead to pronounced nerve damage and permanent disabilities, frequently causing patients to suffer discrimination and stigma (1–3).
The worldwide prevalence of leprosy has declined markedly since the implementation of multi-drug therapy (MDT) recommended by the WHO in the early 1980s (4, 5). However, leprosy remains endemic in some regions of the world. A sizeable number of cases are still appearing in the underdeveloped and developing countries of Southeast Asia, South America, Africa, and the Eastern Pacific (6). According to WHO records, more than 200,000 new cases of leprosy were reported in 2018 (7).
The incidence of leprosy in China has continued to decline during the 21st century. In 2013, the WHO no longer designated China as a country with a high prevalence of leprosy (4). In 2019, the number of new cases of leprosy in China was 464, and the new case detection rate per 100,000 people was 0.03218 (8). At present, leprosy is in a low epidemic state in China, but the distribution of leprosy is unbalanced, with new cases distributed mainly in the southwestern and south-central provinces (9). Shanghai has a low prevalence of leprosy. Early in the 1990s, the prevalence of leprosy in Shanghai was less than 1 per 100,000 people (10).
In the past two decades, migration within China (internal migration), primarily from rural to urban environments, has become very common. Most internal migrants in China are young adults who travel from rural areas to search for improved opportunities in urban centres (11). In 2018, an estimated 241 million people migrated internally (17% of the total national population). As the most economically developed city in China, Shanghai attracts millions of internal migrants annually. By the end of 2019, Shanghai’s resident population was 24.28 million, of which the registered resident population was 14.5 million and the migrant population 9.78 million. Massive internal migration from rural to urban areas poses new challenges for leprosy control in Shanghai.
The aim of this study was to describe the epidemiology of new patients with leprosy reported in Shanghai among residents and internal migrant populations between 2000 and 2019. This will help to identify challenges and provide useful information on which to base more effective leprosy eradication strategies.
A retrospective epidemiological study was performed of all new patients of leprosy reported in Shanghai from 2000 to 2019, with an emphasis on internal migrant cases of leprosy.
Data collection
Leprosy is a mandatory notifiable disease in China. All cases of leprosy in China are registered in the Leprosy Management Information System (http://218.2.99.162). New patients with a diagnosis of leprosy during the period 2000 to 2019 in Shanghai were identified from the Leprosy Management Information System. Epidemiological and clinical information were collected from these cases, including demographic data, medical history, clinical presentation, leprosy reactions, disability, and past misdiagnosis. Diagnosis and clinical classification of leprosy were performed in accordance with the WHO definition and classifications (12, 13). Internal migrants were defined as those who were living in Shanghai but without Shanghai household registration status through the Chinese hukou system.
Statistical analysis
Microsoft Excel was used to create a patient information database. Statistical analyses were performed using Statistical Product and Service Solutions (SPSS) software package ver. 21.0 (IBM Inc., Armonk, NY, USA). Quantitative and qualitative variables of patient characteristics were described as means (ranges) and numbers (percentages), respectively. Fisher’s exact test and Student’s t-test were used to compare qualitative and quantitative variables. p-values less than 0.05 were considered statistically significant.
Ethics statement
This study was approved by the Research Ethics Board of the Shanghai Skin Disease Hospital (#SSD-2020015). Written informed consent was obtained from each participant of the study. All analysed data were anonymized.
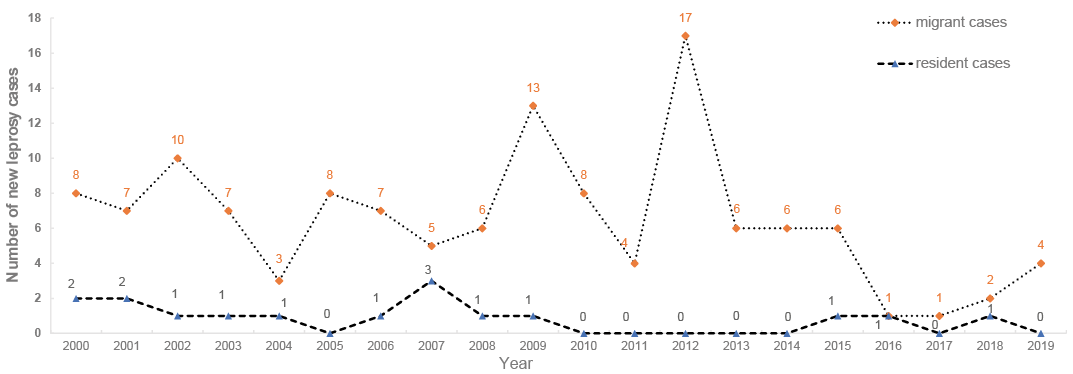
From 1 January 2000 to 31 December 2019, 145 new cases of leprosy were diagnosed in Shanghai. Sixteen (11.0%) cases were residents, and 129 (89.0%) cases were internal migrants. Fig. 1 shows the numbers and trend of new cases of leprosy reported between 2000 and 2019. New cases of leprosy among migrants were reported every year, for which the highest number of cases was 17 in 2012, followed by 13 in 2009, and 11 in 2002. The number of new cases of leprosy among residents was as high as 3 in 2013, while no new cases were found among residents in 2005, 2010 to 2014, 2017, or 2019.
Fig. 1. Trends of new cases of leprosy detected during study period (2000 to 2019) in Shanghai, in migrant and resident populations.
The numbers and geographical distribution of province of origin of all cases during the study period are shown in Table I and Fig. 2. The migrant cases had migrated from 15 different provinces. The highest number of cases of leprosy were reported in migrants from central east provinces around Shanghai, especially Anhui (22 patients; 15.3%), with a significant proportion also occurring in migrants from Jiangxi (20 patients; 13.8%), Jiangsu (18 patients; 12.4%), and Zhejiang (12 patients; 8.2%). The second most important region of origin was the southwest provinces, particularly Sichuan (18 patients; 12.4%), Guizhou (13 patients; 8.9%), and Yunnan (8 patients; 5.5%), where leprosy is still endemic in some areas. Migrants from the northern province accounted for the least cases of leprosy.
Table I. Provincial distribution of all new cases of leprosy during the study period (2000 to 2019)
Fig. 2. Province of origin of internal migration cases of leprosy in Shanghai (2000 to 2019). Size of circles represents number of internal migration cases of leprosy.
Demographic data and clinical information for the cases of leprosy are summarized in Table II. Approximately 73.6% of migrant patients and 81.2% of resident patients were male, and all patients were adults. Most of the migrant patients were between 21 and 40 years old (68.8%), and significantly younger than the resident patients (p < 0.001). Most of the patients in both groups did not recall exposure history to leprosy (91.5% of migrants and 87.5% of residents). A total of 107 migrant patients were diagnosed with multibacillary (MB) leprosy (82.9%), and 12 resident patients had MB leprosy (75%). According to the Ridley and Jopling classification, migrant patients were most likely to be classified as having borderline lepromatous leprosy (BL, 52 patients; 40.3%), lepromatous leprosy (LL, 30 patients; 23.3%), and borderline tuberculoid leprosy (BT, 28 patients; 21.7%). Resident patients were most likely to be classified as having LL (5 patients; 31.2%), borderline leprosy (BB, 4 patients; 25.0%), or BL (3 patients; 18.8%). In total, grade 2 disability (G2D) was recorded for 31 patients (21.4%). There was no significant difference between migrant and resident patients in terms of the percentage with G2D (22.5% vs 12.5%). Approximately 31% of migrant and 37.5% of resident patients experienced leprosy reactions, though this difference was not statistically significant.
Table II. Selected characteristics of new detected cases of leprosy in Shanghai between 2000 and 2019
Migrant patients had a mean of 25.4 (range 2–112) months lag time from onset of symptoms to diagnosis, which was significantly longer than that of resident patients (mean 10.8, range 1–46 months, p < 0.001). Similarly, a longer lag time from the first visit to diagnosis was observed in migrant patients (mean 23.2, range 0–92 months) compared with resident patients (mean 9.4, range 0–35 months, p < 0.001). A large majority of patients had been misdiagnosed, but there was no significant difference between migrant patients (91.5%) and resident patients (87.5%) in terms of misdiagnosis. A total of 52 patients had been misdiagnosed for more than 36 months.
During treatment, patients with PB leprosy were treated with MDT (including 600 mg rifampin and 300 mg clofazimine monthly, and 100 mg dapsone and 50 mg clofazimine daily) for 6 months, and patients with MB leprosy were treated with MDT for 12 months. The treatment completion rate was 100% in both immigrant and resident patients.
Population migration is an important factor in the transmission of infectious diseases. Infectious disease patients and carriers of pathogens can bring pathogens to new areas in migratory flows. Genomic studies show that leprosy originated in East Africa or the Near East, and spread to other parts of the world through human migration (14, 15). In recent decades, cases of leprosy imported by immigrants accounted for the majority of new cases of leprosy in some immigrant-receiving countries (16–20). A study in Spain showed that among the 168 officially registered patients with leprosy from 2003 to 2013, only 40 (24.6%) were residents of Spain, and the remaining 128 (76.2%) were immigrants (16). A report in Italy showed that between 1990 and 2009, the numbers of indigenous cases of leprosy in the country decreased (a total of 12 cases), but the incidence of imported leprosy increased significantly (a total of 159 cases) (17). Similarly, an epidemiological study of leprosy in major cities in France in 2009 and 2010 showed that only 7 (18%) out of 39 new cases of leprosy occurred in French residents (18). A study in Canada also showed that only 1 of the 184 cases of leprosy registered between 1979 and 2002 was a Canadian-born patient, and the other cases of leprosy all occurred in immigrants from 23 different countries (19).
Due to differences in socioeconomic development, developed regions in China have attracted tens of millions of internal migrants (11). These internal migrants have had a noticeable impact on epidemic leprosy in the areas receiving migrants. All new cases of leprosy reported in Beijing in 2007 were migrant cases (21). Internal migrants accounted for 38.3% of new cases of leprosy in Guangdong province in 2015 (22). In the current study, 89.0% of new cases of leprosy in Shanghai from 2000 to 2019 were internal migrants. These internal migrant cases originated mainly from 2 areas: provinces surrounding Shanghai (Anhui, Jiangsu, Jiangxi, and Zhejiang), which are close to Shanghai and easy to migrate from; and the southwestern provinces (Sichuan, Yunnan, and Guizhou), which have the highest incidence of leprosy in China (21, 23).
The proportion of MB leprosy in China is at a high level (8, 24–26), reaching 84.6% during the period 2011 to 2015 (21). In the current study, the proportion of MB leprosy in Shanghai was 82.1%, and was not significantly different between the resident leprosy population (75.0%) and the migrant leprosy population (82.9%). The current study also found that the migrant leprosy population was younger than the resident leprosy population. In China, internal migrants are mainly young people. As the main labour force in society, young people move between different areas in search of a better career and life opportunities (11). Young people tend to have a wider range of social activities, which may be conducive to the transmission of infectious diseases. Therefore, patients with MB leprosy may become a mobile source of infection for leprosy and cause public health problems. In the current study, only 13 patients (9%) admitted having a history of exposure to leprosy. Possible reasons for this are that patients with leprosy may fear discrimination and conceal their medical history, or that it is difficult for patients to recall their contact history because of the long incubation period of leprosy.
In the current study, the G2D rate in patients with leprosy reached 21.4%, which may be related to the high rate of misdiagnosis of leprosy and the long delay in diagnosis. A total of 91% of the patients with leprosy in this study had been misdiagnosed. Among these patients, the mean delay from symptom onset to diagnosis was 23.8 months, and the mean delay from first visit to diagnosis was 21.7 months, indicating that misdiagnosis was the main reason for the long delay in diagnosis of leprosy. Most of the patients with leprosy with G2D had not been properly diagnosed and treated in other hospitals for many years, which led to aggravated disability. Because the main symptom of leprosy manifested in the skin and peripheral nervous, misdiagnosis by dermatologists and neurologists was the most common. It is therefore necessary to strengthen medical staff training in the diagnosis of leprosy, especially that of staff in the departments of dermatology and neurology. For example, theoretical teaching and on-site demonstrations should be held regularly, in the form of lectures, case discussions, or short-term clinical practice classes, in order to improve the diagnostic accuracy of medical staff.
The current study also found that migrant cases of leprosy often had a longer delay in diagnosis than resident cases. This may be because local-born urban residents in Shanghai are entitled to a series of social welfare programmes (e.g. medical care) from the local government, while some migrants lack these benefits (27). In addition, socioeconomic status indicators show that migrants have lower socioeconomic status than urban residents (27, 28), suggesting that these gaps may make it more difficult for migrants to receive quality medical resources compared with urban residents, leading to a longer delay in leprosy diagnoses (29, 30). Medical staff need more professional training so that they can identify suspected cases of leprosy and provide timely referral services. Popular health education and frequent media coverage about leprosy should be provided in immigrant communities to help people understand the disease and to eliminate fear and discrimination. These measures may be helpful to improve the access of migrants to leprosy services. Future studies should investigate the specific reasons for longer delay in diagnosis of leprosy in migrant cases.
Internal immigration to Shanghai has increased annually, and has had an adverse impact on the prevention and control of epidemic leprosy. In particular, patients with leprosy are not often identified and treated in time, which may aggravate disability and transmission of the disease. Although there has been no report of second-generation cases caused by migrant leprosy patients in Shanghai, it is necessary to research the influence of migrant leprosy patients on healthy populations and to improve clinicians’ ability in order to ensure diagnosis of new leprosy patients as early as possible.
The authors thank Jiakun Chen, Jiayu Le and Renbao Zhang for their contribution to the study.
This work was supported by Supporting Project of Medical Guidance (Western Medicine) of Science and Technology Commission of Shanghai Municipality (17411970400) and National Natural Science Foundation of China (81872537).
The authors have no conflicts of interest to disclose.


 Click to show fullsize
Click to show fullsize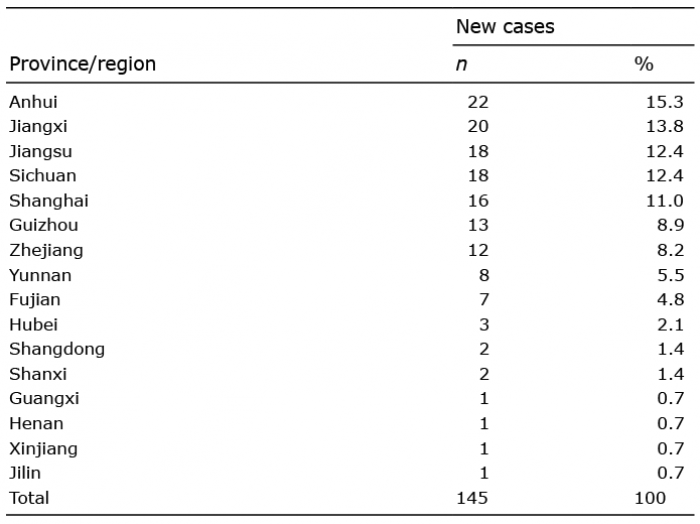 Click to show fullsize
Click to show fullsize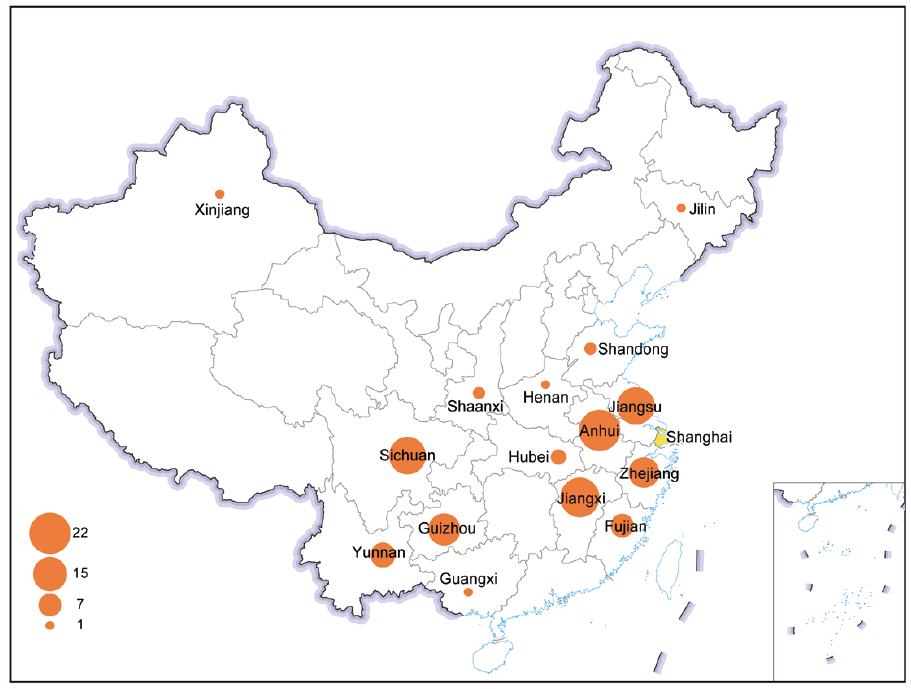 Click to show fullsize
Click to show fullsize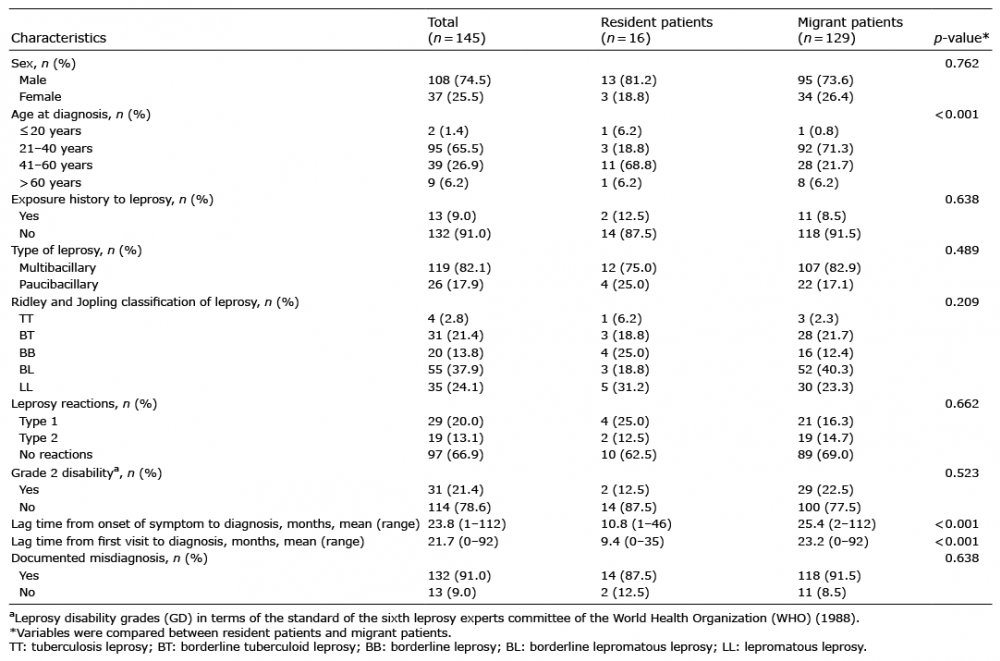 Click to show fullsize
Click to show fullsize