


1Department of Dermatology and Plastic Surgery, Akita University Graduate School of Medicine, Akita and 2Department of Dermatology, Nippon Medical School Tama Nagayama Hospital, 1-7-1 Nagayama, Tama City, 206-8512 Tokyo, Japan. E-mail: osada0130@nms.ac.jp
Accepted May 19, 2021; Epub ahead of print May 24, 2021
Acta Derm Venereol 2021; 101: adv00468.
doi: 10.2340/00015555-3835
Drug-induced hypersensitivity syndrome (DiHS)/drug reaction with eosinophilia and systemic symptoms (DRESS) is a rare, adverse drug reaction with acute skin rash, fever, lymphadenopathy, eosinophilia, and the involvement of at least one internal organ (especially the liver) (1, 2). Drug allergy and viral reactivation are implicated in the pathogenesis of this disease; DiHS and DRESS could be part of the continuum of the same disease (1), although human herpes virus-6 (HHV-6) reactivation is not included in the DRESS criteria (3). Epstein-Barr virus (EBV), cytomegalovirus (CMV), and HHV-6 are also reactivated during the course of DiHS/DRESS (1). We report here the first case of DiHS/DRESS caused by lenalidomide, a derivative of thalidomide with more potent immunomodulatory and anti-tumor activities, in which both HHV-6 and CMV were reactivated.
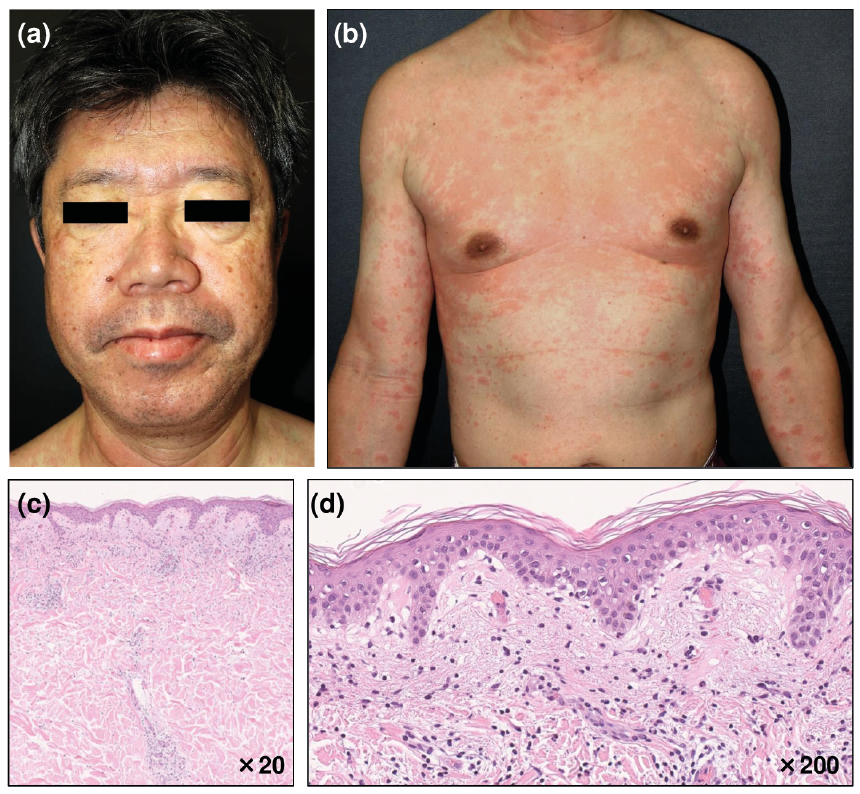
A 59-year-old man presented with a maculopapular pruritic rash on the face, trunk, upper and lower extremities associated with fever (> 38.5°C), periorbital oedema, swelling of the lower lip, and mild cervical lymphadenopathy (Fig. 1a, b). He was treated for multiple myeloma and received a combination therapy with bortezomib, lenalidomide, and dexamethasone (VRd). Despite the patient developing a rash 9 days after completing the first cycles of VRd therapy, the second cycle was continued and completed. Laboratory tests revealed leukocytosis (11,900 cells/l; normal value <9,000 cells/l), eosinophilia (2,980 cells/ µl; normal < 500/ µl), monocytosis (1,190 cells/µl; normal 90–690/µl) and atypical lymphocytes (2%). Increased serum alanine aminotransferase (61 U/l; normal 5–40 U/l), lactate dehydrogenase (342 U/l; normal 115–245 U/l), and γ-glutamyl transpeptidase (89 U/l; normal < 70 U/l), and decreased serum IgG (510 mg/dl; normal 861–1,747 mg/dl), IgM (7 mg/dl; normal 33–183 mg/dl), and IgA (15 mg/dl; normal 93–393 mg/dl) levels were also observed. Viral reactivation was detected; titres of anti-human herpes virus-6 (HHV-6) IgG (using immunofluorescence assay) and anti-cytomegalovirus (CMV) IgG (using enzyme immunoassay) increased from < 10 fold (at presentation) to ×640 fold (on day 40) and from 9.3 IU/ml (at presentation) to 17.9 IU/ml (on day 40), respectively.
Fig. 1. Clinical presentations of (a) the face and (b) the trunk at the first visit. Histopathology of a biopsy specimen. Perivascular lymphocytic infiltration in the upper dermis (c) and liquefaction degeneration at the dermoepidermal junction (d) (Haematoxylin-eosin staining; original magnifications (c: ×20, d: ×200)). Permission is given by the patient to publish these photos.
A biopsy was taken from an infiltrated erythema on the patient’s abdomen, and showed perivascular lymphocytic infiltration in the upper dermis and liquefaction degeneration at the dermoepidermal junction (Fig. 1c, d). These clinical and laboratory data fulfilled the diagnostic criteria for DiHS/DRESS (Table I) (1, 2). Monocytosis and a marked decrease in serum Ig levels confirmed an acute phase of DiHS/DRESS (1). The patient’s cutaneous manifestations and pruritus persisted after the discontinuation of lenalidomide. Administration of prednisolone (20 mg/day) improved these symptoms; it was gradually tapered and ceased in 3 weeks, without recurrence. Since thalidomide and its derivatives is critical to prevent the growth of myeloma cells, pomalidomide, another thalidomide derivative, was administered to the patient. The cutaneous pruritic manifestations reappeared after administering pomalidomide. These results indicated that thalidomide derivatives were causative agents for DiHS/DRESS in this patient. Eventually, the patient achieved complete remission with an autologous haematopoietic stem cell transplant. DiHS/DRESS is known to be caused by a limited number of drugs, and thalidomide and its derivatives represent potentially responsible drugs for this condition.
Table I. Summary of lenalidomide-induced drug-induced hypersensitivity syndrome (DiHS)/drug reaction with eosinophilia and systemic symptoms (DRESS) cases
There are 4 previous reports on DRESS caused by lenalidomide (Table I) (4–7). Since HHV-6 reactivation is not included in the DRESS criteria (2), HHV-6 reactivation was investigated in only 2 cases (excluding the current case) and found in one. Since the current case fulfilled both the DiHS and DRESS criteria, this case is the second definite DRESS with HHV-6 reactivation or typical DiHS. CMV reactivation was also detected in the current patient. A recent report has clarified that CMV DNA positivity affects the clinical course and prognosis of patients with DiHS/DRESS; CMV DNA-positive cases took a more severe and protracted course and had a higher risk of developing CMV-related complications, such as pneumonia, peritonitis, and intestinal bleeding (8). Since CMV reactivation was not investigated in other cases, its involvement in the pathogenesis of lenalidomide-DiHS/DRESS cases have to be confirmed by further studies.
As shown in Table I, all patients with DiHS/DRESS caused by lenalidomide had a medical history of hypertension, diabetes mellitus, and/or renal dysfunction, suggesting that these underlying conditions could be risk factors for lenalidomide-related-DiHS/DRESS. Alternatively, the drugs used for treating these diseases may affect the immunomodulatory activity of lenalidomide.
What is the mechanism for lenalidomide caused DiHS/DRESS? Reductions in CD56+ NK cells, CD19+ B cells and serum Ig levels and increases in CD4+CD25+Foxp3+ Tregs are observed in the acute phase of DiHS/DRESS (1). Thalidomide, lenalidomide, and pomalidomide bind to cereblon (CRBN), which activates the enzymatic activity of the CRBN E3 ubiquitin ligase complex, leading to the ubiquitination and proteasome-dependent degradation of Ikaros and Aiolos (transcription regulators of B cell development) (9, 10). Under normal conditions, Ikaros stimulates the expression of interferon regulatory factor 4 (IRF4), a key regulator of B cell development at the pre-B cell stage and plasma cell differentiation. Aiolos is required for normal plasma cell development in mice. Thus, the degradation of Ikaros and Aiolos by lenalidomide suppresses the function of B cells and myeloma growth.
Lenalidomide also affects T cell function through IL-2, which is required for the maintenance of Tregs (11). Since Ikaros normally suppresses IL-2 expression in T cells, its loss due to lenalidomide may activate T-cell mediated immune responses and increase the Treg population by the upregulation of IL-2 production.
Causative agents of DiHS/DRESS, such as anticonvulsants and sulphonamides, commonly affect B cell differentiation and inhibit immunoglobulin production, although they have different pharmacological effects. However, the molecular mechanism underlying the immunosuppressive effects of these drugs remains to be elucidated. Although the number of DiHS/DRESS cases caused by thalidomide derivatives is still limited, analysis of the cereblon–Ikaros/Aiolos-IRF4/Il-2 signalling pathway could be helpful in clarifying the mechanism of the impairment of B and T cell functions in DiHS/DRESS.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize