


1Department of Dermatology, The Jikei University School of Medicine, and 2Juntendo Itch Research Center, Institute for Environmental and Gender-Specific Medicine, Juntendo University Graduate School of Medicine, Tokyo, Japan
The aim of this study is to elucidate the relationship between 2 different types of severity-indicating parameters (i.e. between subjective and objective severity- indicating parameters in patients with atopic dermatitis. The disease severity of 55 patients with atopic dermatitis was assessed using 7 subjective parameters indicating severity, including visual analogue scale for itch, Patient-Oriented Eczema Measure, 5-D itch scale, Dermatology Life Quality Index, Eczema Area and Severity Index, body surface area, and Investigator Global Assessment, and 8 objective parameters indicating severity, including eosinophil relative count, neutrophil-to-lymphocyte ratio, lactate dehydrogenase, and thymus and activation-regulated chemokine. Five subjective parameters reflecting itch correlated significantly with eosinophil relative count, but not with neutrophil-to-lymphocyte ratio. In contrast, 2 subjective parameters, mainly reflecting the degree of inflammation and area of affected regions, correlated significantly with neutrophil-to-lymphocyte ratio. The eosinophil relative count may correlate with the degree of itch, while the neutrophil-to-lymphocyte ratio may correlate with the degree of inflammation and the area of the affected region. The eosinophil relative count and neutrophil-to-lymphocyte ratio may thus be stand-alone parameters from each other in the assessment of the severity of atopic dermatitis.
Key words: atopic dermatitis; subjective parameters; objective parameters; itch; neutrophil-to-lymphocyte ratio; eosinophil relative count.
Accepted May 26, 2021; Epub ahead of print May 27, 2021
Acta Derm Venereol 2021; 101: adv00491.
doi: 10.2340/00015555-3838
Corr: Yoshimasa Nobeyama, Department of Dermatology, The Jikei University School of Medicine, 25-8 Nishi-Shimbashi 3-chome, Minato-ku, Tokyo 105-8461, Japan. E-mail: nobederm@jikei.ac.jp
To date, the relationship between the 2 different types of severity-indicating parameters (i.e. between subjective and objective severity-indicating parameters) in patients with atopic dermatitis has not been sufficiently elucidated. This study elucidates the relationship between the subjective and objective severity-indicating parameters in atopic dermatitis. Eosinophil relative count in the peripheral blood is considered to correlate with degree of itch in patients with atopic dermatitis, while neutrophil-to-lymphocyte ratio in the peripheral blood is considered to correlate with the degree of inflammation and the area of the affected region. Eosinophil relative count and neutrophil-to-lymphocyte ratio may be stand-alone parameters from each other in the assessment of the severity of atopic dermatitis.
Atopic dermatitis (AD) is a chronic, relapsing, inflammatory skin disease characterized by eczema and itch (1, 2). For persistent AD, various new therapeutic options are being developed, e.g. interleukin (IL)-4/IL-13 inhibitors, janus kinase inhibitors, a dual janus kinase/spleen tyrosine kinase inhibitor, a histamine H4 receptor inhibitor, thymic stromal lymphopoietin/OX40 ligand pathway inhibitors, an IL-22 inhibitor, and an IL-17C inhibitor (3). To evaluate the various therapeutic options and study the course of the disease, many assessment parameters have been widely used.
Objective parameters used to indicate the severity of AD include: lactate dehydrogenase (LDH) (4), eosinophil count (5), thymus and activation-regulated chemokine (TARC) (6), and total IgE in the blood. These objective parameters provide strong levels of evidence regarding disease severity, although the level of total IgE in the blood is reported to correlate with long-term control status, not current severity (7). However, the results obtained from these objective parameters leave no margin for a subjective view.
Subjective parameters to indicate the severity of AD include: visual analogue scale (VAS) for itch (8), Patient-Oriented Eczema Measure (POEM) (9), 5-D itch scale (10), Dermatology Life Quality Index (DLQI) (11), Eczema Area and Severity Index (EASI) (12), validated Investigator Global Assessment for AD scale (IGA) (13), and body surface area (BSA) (14). These severity-indicating parameters are recorded by a patient and/or a clinician. However, even if the scores are recorded by clinicians, they are relatively subjective compared with the results of blood tests.
There are many studies evaluating subjective parameters indicating severity by comparing the results from different, or the same, subjective parameters (e.g. EASI vs IGA (15); EASI vs IGA vs Scoring Atopic Dermatitis (SCORAD) index (16); POEM vs DLQI, children’s DLQI and patients’ global severity assessments (9); VAS for itch vs numerical rating scale for itch or verbal rating scale for itch (17); 12-Item Pruritus Severity Score vs VAS for itch or DLQI (18)). Thus, the subjective parameters have been relatively sufficiently evaluated from the standpoints of content validity, construction validity and internal consistency (19, 20).
In contrast, there are few studies describing the relationship between the results obtained from objective parameters indicating severity and those obtained from subjective parameters. Stone et al. (21) suggested that total IgE level in the blood does not correlate with subjective assessment of the severity of dermatitis. Kataoka et al. (22) examined the correlation of the results from objective parameters with the results from EASI, using linear regression analysis in 96 patients with AD. They found R-values of 0.673 between TARC and EASI, 0.449 between LDH and EASI, 0.226 between eosinophil count and EASI, and 0.326 between total IgE and EASI. Jiang et al. (23) reported that the neutrophil-to-lymphocyte ratio (NLR), which is a ratio of absolute count of neutrophils to that of lymphocytes in the peripheral blood, was related to the SCORAD index in 80 patients with AD. Thus, the relationship between 2 different types of severity-indicating parameters (i.e. subjective and objective severity-indicating parameters) was evaluated separately in the current study. The aim of this study is to elucidate the correlation between objective and subjective severity-indicating parameters in patients with AD.
Patients and assessments
The ethics committee of The Jikei University School of Medicine, Tokyo, Japan, approved the study protocol (approval number #25-210), and all patients provided written informed consent prior to enrolment. For this study, 55 patients with AD were recruited (36 men, 19 women) who met the following inclusion criteria: (i) referral to The Jikei University School of Medicine, (ii) fulfilment of the diagnostic criteria for AD described by Hanifin & Rajka (24), (iii) agreement to assessment of subjective severity of AD by VAS for itch, POEM, 5-D itch scale, DLQI, EASI, IGA and BSA, and to assessment of objective severity of AD by peripheral blood tests, including LDH level, total IgE level, TARC level and differential white blood cell count, such as lymphocyte relative count (lymphocyte percentage in white blood cells), neutrophil relative count (neutrophil percentage in white blood cells), eosinophil relative count (eosinophil percentage in white blood cells), NLR and eosinophil-to-lymphocyte ratio (ELR), which is a ratio of absolute count of eosinophil to that of lymphocytes in the peripheral blood, for the administration of dupilumab. Mean age of recruited patients was 42.9 years (range 18–61 years). Exclusion criteria were: (i) administration of systemic immunosuppressants and systemic corticosteroids; (ii) treatment with phototherapy; and (iii) pregnancy and breast-feeding.
Subjective severity was scored by Japanese dermatological association-authorized dermatologists and the patients who fulfilled the above conditions. A segment score of EASI for erythema (EASI-Er) was calculated as the total sum of scores of erythema multiplied by both area score and 0.1 for head/neck, 0.3 for trunk, 0.2 for upper limbs or 0.4 for lower limbs, which are constants which reflect the relative contribution of those regions to the total body surface area. Similarly, segment scores of EASI for induration/papulation (EASI-InPa), excoriation (EASI-Ex) and lichenification (EASI-Li) were calculated as the total sum of scores of induration/papulation, excoriation and lichenification, respectively, multiplied by both area score and 0.1 for head/neck, 0.3 for trunk, 0.2 for upper limbs or 0.4 for lower limbs.
Blood examination
Differential white blood cell count was performed with an automatic blood cell count analyser (XE-5000; Sysmex, Kobe, Japan). NLR and ELR were calculated from the data obtained from differential white blood cell counts. Biochemical blood analysis was performed with an automatic analyser LABOSPECT 008α (Hitachi, Tokyo, Japan) for LDH level, automatic chemiluminescent enzyme immunity analyser AIA-CL2400 (Tosoh, Tokyo, Japan) for total IgE level, and automatic immunity analyser HISCL-5000 (Sysmex, Kobe, Japan) for TARC level.
Statistical analysis
Statistical analysis was performed using SPSS version 22 software (SPSS Japan, Tokyo, Japan). Linear regression analysis was performed to evaluate the relationships between the results obtained from subjective and objective parameters indicating disease severity. Values of p < 0.05 were considered statistically significant.
Eczema Area and Severity Index is well correlated with objective parameters
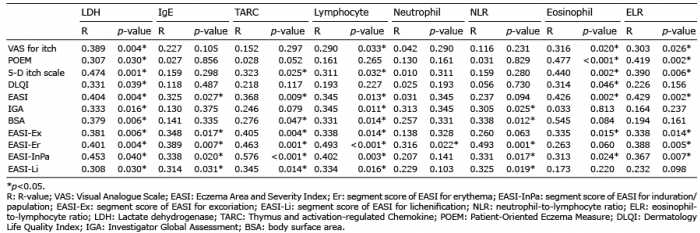
The results of VAS for itch showed significant correlation with LDH level, lymphocyte relative count, eosinophil relative count and ELR (Table I, Fig. 1, Fig. S1). Similarly, the results of POEM showed significant correlation with LDH level, eosinophil relative count and ELR. The results of 5-D itch scale showed significant correlation with LDH level, TARC level, lymphocyte relative count, eosinophil relative count and ELR. The results of DLQI showed significant correlation with LDH level and eosinophil relative count. The results of EASI showed significant correlation with LDH level, total IgE level, TARC level, lymphocyte relative count, eosinophil relative count and ELR. The results of IGA showed significant correlation with LDH level, lymphocyte relative count and NLR. The results of BSA showed significant correlation with LDH level, TARC level, lymphocyte relative count and NLR. Among the results listed above, the results of EASI were significantly correlated with the largest number of examined objective parameters indicating severity.
Table I. Correlation between severity-indicating subjective and objective parameters of atopic dermatitis
Fig. 1. Correlation between subjective and objective parameters. Grey and white squares indicate significant and non-significant correlations, respectively. Vertical axis indicates each subjective parameter indicating severity. Horizontal axis indicates each objective parameter indicating severity. Subjective parameters indicating severity of itching and those not signifying itching are grouped separately. LDH: Lactate dehydrogenase in the peripheral blood; IgE: Immunoglobulin E in the peripheral blood; TARC: Thymus and activation-regulated Chemokine in the peripheral blood; Lym: lymphocyte relative count in the peripheral blood; Neu: neutrophil relative count in the peripheral blood; NLR: neutrophil-to-lymphocyte ratio; Eo: eosinophil relative count in the peripheral blood; ELR: eosinophil-to-lymphocyte ratio; VAS: Visual Analogue Scale; POEM: Patient-Oriented Eczema Measure; DLQI: Dermatology Life Quality Index; IGA: Investigator Global Assessment; BSA: body surface area; EASI: Eczema Area and Severity Index; -Ex: segment score of Eczema Area and Severity Index for excoriation; EASI-Er: segment score of EASI for erythema; EASI-InPa: segment score of EASI for induration/ papulation; EASI-Li: segment score of EASI for lichenification.
Eosinophil relative count reflects degree of itch, while neutrophil-to-lymphocyte ratio reflects degree of inflammation and area of affected regions
LDH level showed significant correlation with the results of all examined subjective parameters indicating severity (Table I, Fig. 1, Fig. S1). Total IgE level did not show significant correlation with the results of all examined subjective parameters, except for EASI. TARC level showed significant correlation with 3 out of 7 subjective parameters. Lymphocyte relative count showed significant correlation with 5 out of 7 subjective parameters. Neutrophil relative count did not show significant correlation with any results of all 7 examined subjective parameters. NLR showed significant correlation with 2 out of 7 subjective parameters, IGA and BSA, both of which indicate degree of inflammation and area of affected regions, but not direct itching sensation. Eosinophil relative count showed significant correlation with 5 out of 7 subjective parameters, all of which, at least partly, indicate itching sensation. ELR showed significant correlation with the results of 4 out of 7 subjective parameters, at least partly responsible for itching sensation (Table I, Fig. 1, Fig. 2 and Fig. S1).
Fig. 2. Stand-alone relationship between eosinophil relative count and neutrophil-to-lymphocyte ratio (NLR). A stand-alone relationship between eosinophil relative count and NLR is simply illustrated. Patients with atopic dermatitis (AD) with higher eosinophil ratio in the blood tend to have worse symptoms, while clinicians tend to consider the conditions of patients with AD with higher NLR to be more severe.
Eczema Area and Severity Index segments to directly indicate itch correlates with eosinophil relative count and eosinophil-to-lymphocyte ratio
EASI-Ex showed significant correlation with LDH level, total IgE level, TARC level, lymphocyte relative count, eosinophil relative count and ELR, but not NLR. EASI-Er showed significant correlation with LDH level, total IgE level, TARC level, lymphocyte relative count, neutrophil relative count, NLR and ELR. EASI-InPa showed significant correlation with LDH level, total IgE level, TARC level, lymphocyte relative count, NLR, eosinophil relative count and ELR. EASI-Li showed significant correlation with LDH level, total IgE level, TARC level, lymphocyte relative count and NLR (Table I, Fig. 1, Fig. S1).
This study elucidates the relationship between the severity-indicating subjective and objective parameters in AD. The results of EASI were correlated with those of most examined objective parameters, while the results of DLQI were correlated with those of few examined objective parameters. Furthermore, interesting correlations were found between the results of some subjective and objective severity-indicating parameters.
Seven examined subjective parameters indicating severity are classified into 2 groups: one group consists of scoring systems to signify mainly itching sensation and other group consists of scoring systems to signify mainly the degree of inflammation and area of affected regions (Fig. 1). All 5 subjective parameters signifying itching sensation were at least partly significantly correlated with eosinophil relative count and/or ELR (Fig. 1, Fig. S1). None of these subjective parameters were significantly correlated with NLR. In contrast, 2 subjective severity-indicating parameters, which signify degree of inflammation and area of affected regions, were significantly correlated with NLR, but not with eosinophil relative count or ELR. Therefore, patients with AD who have higher eosinophil relative counts in the blood tend have a higher level of itching sensation, while clinicians tend to consider that the condition of patients with higher NLR is more severe (Fig. 2). This indicates a gap in the assessment of severity of AD between patients and dermatologists.
There is a lot of evidence to support that eosinophils play an important role in itching sensation in patients with AD. Previous literature suggests that eosinophils directly communicate with nerves, based on the fact that degranulated eosinophils accumulate near nerve fibres with substance P, which potentially activates human eosinophils (25), in an AD-stress mouse model (26). Some studies have demonstrated that activation of eosinophils leads to the release of IL-31 (27, 28), which is a critical cytokine in itch and nerve growth (29, 30). In addition, Cevikbas et al. (29) reported that cutaneous and intrathecal injections of IL-31 evoked robust scratching behaviour in mice. Based on these results, we hypothesized that eosinophils strongly affect the results of subjective parameters indicating the severity of AD, which signify the itching sensation, probably via the mechanisms associated with substance P and IL-31.
There is a lot of evidence to support that NLR indicates various biological significances. Alan et al. (31) reported that NLR is regarded as a useful marker for estimating inflammation in Behçet’s disease. Also, many studies show that NLR is a useful marker for predicting the prognosis of various diseases, including malignancies, peripheral vascular diseases and cardiovascular events (32–36). Based on this evidence, we hypothesized that NLR may be associated with the characteristics of the biological settings of AD, and we then opted to examine NLR as a candidate for an objective parameter indicating the severity of AD.
To confirm that: (i) the degree of itching sensation relates to eosinophil relative count and ELR; and (ii) the degree of inflammation and area of affected regions relate to NLR, this study examined each segment score of EASI. The EASI was scored separately, based on the degree of erythema, induration/papulation, excoriation (scratching) and lichenification. Each separate score was examined with the objective parameters indicating severity, including LDH level, total IgE level, TARC level, lymphocyte relative count, neutrophil relative count, NLR, eosinophil relative count and ELR. The examinations showed that: (i) NLR was not correlated with the score of EASI-Ex, an EASI segment that directly indicates itching sensation. Interestingly, the NLR was significantly correlated with the scores of EASI-Er, EASI-InPa and EASI-Li, which are considered as EASI segments that do not indicate itching sensation directly; and (ii) eosinophil relative count and ELR were correlated with EASI-Ex, but not EASI-Li (Fig. 1 and Fig. S1h–k). These facts also suggest that: (i) itching sensation is reflected in eosinophil ratio and ELR; and (ii) signs of eczema other than direct itching sensation are reliably reflected in NLR.
Among the 7 subjective parameters indicating severity examined in the current study, the results of EASI and 5-D itch scale were significantly correlated with all of TARC level, LDH level, eosinophil relative count and ELR (Fig. 1). Schmitt et al. (19) assessed the content validity, construction validity, internal consistency, interobserver reliability, test-retest reliability, sensitivity to change and acceptability (shortness of required time) of various parameters indicating AD severity, and they suggested that SCORAD, EASI and POEM fulfil such factors. In addition to these aspects, the current study potentially supports that EASI and 5-D itch scale fulfil a certain level of concurrent validity with the objective parameters indicating severity to indicate the current severity of AD (4–6).
In this study, all of the results obtained from the subjective parameters indicating severity were significantly correlated with LDH level in the peripheral blood (Fig. 1, Fig. S1). Moreover, most of the results of the subjective parameters indicating severity were correlated with lymphocyte relative count in the peripheral blood. Lymphocyte relative count was decreased when the subjective parameters indicating severity refer a severe condition of AD, in line with the previous report by Jiang et al. (23), that SCORAD score was linked to lymphocyte count in the peripheral blood. Similarly, most of the results obtained from the subjective parameters indicating severity were correlated with TARC level in the blood. Thijs et al. (37) performed a meta-analysis of 108 articles, and suggested that TARC level is the most reliable biomarker for AD, and that LDH level may be useful, but that additional research is required. The current study provides additional evidence that lymphocyte relative count and LDH level in the peripheral blood are reliable objective severity markers of AD.
Previous literature has described the relationship of total IgE levels with severities categorized by EASI scores (38), which is in line with the result of the current study that total IgE levels were correlated with EASI scores. The current study analysed the correlation further, resulting that all segment scores of EASI were correlated with total IgE levels (Fig. 1). It was found that the segment score of lichenification in EASI (EASI-Li) was correlated with total IgE levels, which is compatible with evidence that total IgE levels indicate the long-term control status of AD (7). However, the segment scores of erythema, induration/papulation and excoriation (scratching) in EASI do not seem to be compatible with total IgE level. Further study is required to elucidate the relationship between the results of scoring systems, such as EASI and total IgE level.
Limitations
Some limitations of this study should be considered. The first is the low number of examined subjective parameters indicating severity; hence, examinations of more subjective parameters indicating severity would more strongly support the results of this study. The second is a selection bias. The patients who agreed to be treated with dupilumab were included in the analyses. Scores reported by a patient could be another limiting factor, as the patients might consciously or subconsciously make themselves look as if they have a more severe condition. The third is an indirect influence of itching sensation on the scores of IGA and BSA. Although IGA and BSA were regarded as the parameters mainly indicating the degree of inflammation and area of the affected regions, these parameters may partially draw influence from the itching sensation, which potentially leads to scratching-associated eruption, such as excoriation.
Conclusion
This study suggests that eosinophil relative count and ELR correlate with the scores of scoring systems indicating itching sensation, while NLR correlates with those indicating the degree of inflammation and area of affected regions. Eosinophil relative count and NLR appear to be a stand-alone parameters from each other in the assessment of AD severity. Understanding of such characteristics of objective severity-indicating parameters may lead to more accurate evaluation for the patients with AD.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize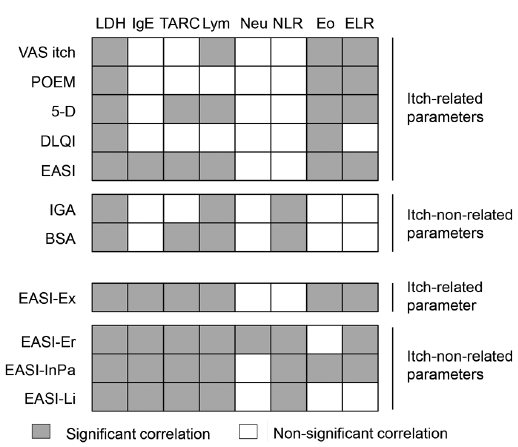 Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize