


1Family Medicine and Primary Care, Lee Kong Chian School of Medicine, Nanyang Technological University Singapore, 2National Healthcare Group Polyclinics, 3National Skin Centre, 4Skin Research Institute of Singapore, and 5Dermatology and Skin Biology, Lee Kong Chian School of Medicine, Nanyang Technological University Singapore, Singapore
Most teledermatology studies focus on patients’ satisfaction; fewer focus on the experiences of healthcare professionals. This qualitative study explored healthcare professionals’ perceptions of teledermatology used for linking public primary care clinics with the specialist dermatology centre in Singapore. Semi-structured in-depth interviews were conducted with 25 family physicians and dermatologists. Six themes were identified: satisfaction with the service; perceived patient benefits; rationale for introducing teledermatology; educational impact; challenges of virtual consultations; and desirable service refinements for the future. Family physicians and dermatologists were positive about the service, but highlighted a need to streamline referral processes and improve the quality of transmitted images. Reduced need for referral to the specialist centre could be achieved by expanding the polyclinic’s pharmacopoeia and treatment modalities. This study highlights the benefits of telemedicine for patient, professionals, and healthcare organizations, and these are reassuring given the widespread and rapid introduction of telemedicine through necessity during the COVID-19 pandemic.
Key words: qualitative research; telemedicine; dermatology; teledermatology; healthcare professionals’ experience.
Accepted May 26, 2021; Epub ahead of print May 27, 2021
Acta Derm Venereol 2021; 101: adv00540.
doi: 10.2340/00015555-3847
Corr: Helen Elizabeth Smith, Lee Kong Chian School of Medicine, Nanyang Technological University, 11 Mandalay Road, Singapore 308232. E-mail: h.e.smith@ntu.edu.sg
Few teledermatology studies report the experiences of healthcare professionals. In this study 25 family physicians and dermatologists were interviewed regarding their experiences of providing teledermatology service that enabled patients in primary care clinics to link with a specialist dermatology centre. Many benefits were identified, including: service satisfaction, patient benefits, educational opportunities, and future service refinements. Areas for improvement were also identified, including the referral processes, the quality of transmitted images, and the treatment available at the primary care clinics. This study highlights the benefits of telemedicine, which are reassuring findings as telemedicine becomes more widely used due to the COVID-19 pandemic.
In the 2013 Global Burden of Disease study (1), skin diseases were amongst the top 20 reasons for loss of disability-adjusted life years. Primary care consultations for skin problems are very common; a study from the Netherlands estimated that they accounted for 13% of primary care consultations (2), and a UK study suggested it may be as great as 24% (3). Whilst many skin problems can be dealt with in a community setting, when there is diagnostic uncertainty or lack of skill or equipment for the investigation and treatment, referral to a specialist dermatology service is appropriate.
In the 1990s, when teledermatology was developing, it was envisaged it would be used in rural areas where access to specialist dermatological care was limited (4). With advancements in technology, the use of teledermatology has become much more widespread. There are 3 modes of teledermatology consultation: “store-and- forward”, live videoconferencing, or a combination of both. The store-and-forward teledermatology consultation involves sending digital images of the skin condition for later expert review. In contrast, live video-conferencing consultations are synchronous, with patient-clinician interaction in real-time. Currently, the store-and-forward mode is more widely used; it has a strong evidence base, and requires less sophisticated equipment (5).
Teledermatology has been reported to be useful in different patient populations globally (6). One study from Singapore described how nurses and nursing aides took photographs of nursing home residents’ skin problems and uploaded these for a dermatologist to evaluate. The referral process was onerous, taking, on average, 86 min of nursing home staffs’ time, but only 11 min were needed for the dermatologist to review the case and provide advice. Staff satisfaction with the service was assessed using an online questionnaire, which initially highlighted concerns about computer skills and reimbursement (7).
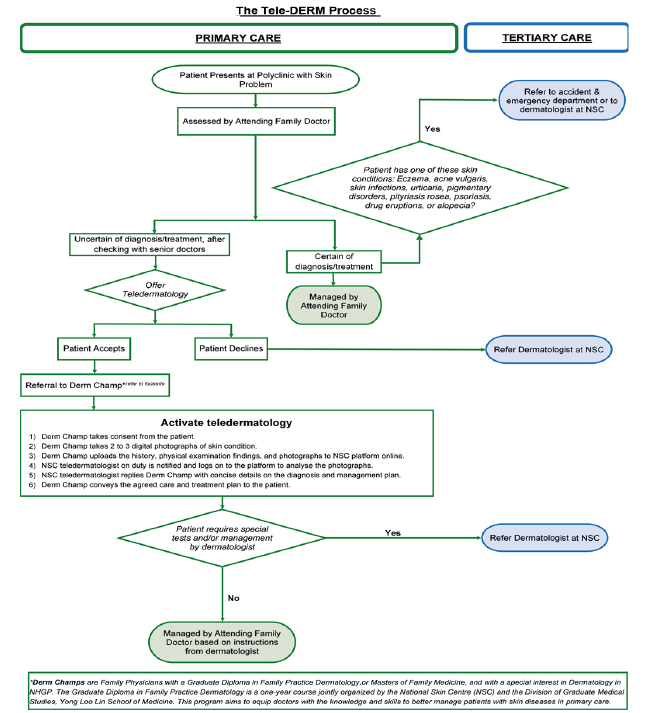
In 2016 the National Healthcare Group introduced a teledermatology service between its polyclinics (i.e. public primary healthcare centres/clinics) and the National Skin Centre (a tertiary healthcare institution). Using “store-and-forward teledermatology”, the medical history and digital photographs of patient’s skin complaints are sent by a polyclinic doctor to a dermatologist through a secure web portal (8) (Fig. 1). This study reports the experiences of the family physicians and specialist medical practitioners using this service, in order to understand their experiences and any difficulties encountered.
Fig. 1. The teledermatology referral and management process between public primary healthcare clinics and specialist dermatology centre. NSC: National Skin Centre.
Participants
Family physicians (n = 15) and dermatologists (n = 10) involved in the delivery of the teledermatology service were interviewed. Eligible doctors willing to be interviewed shared their contact details with the research team and a mutually convenient time was arranged for an interview.
Semi-structured interview
Face-to-face semi-structured interviews were conducted in March–July 2019 by an experienced qualitative researcher. The topic guide (Appendix S1) explored doctors’ experiences of teledermatology, and refinements needed to improve the patient and professional experience. One interviewee preferred not to be audio-recorded, so contemporaneous notes were taken. All interviews were in English.
Data analysis
Digital audio recordings were transcribed verbatim, de-identified, and entered into NVivo (9). Data analysis followed Burnard’s structured approach (10) to thematic content analysis. Two researchers (AC, TSH) independently coded the interviews, before discussing the themes and revising the coding structure with a senior member of the research team (HES). Each of the themes is illustrated with quotes with the interviewee’s identifier in brackets; letters relate to the institution (specialist centre (SC) or public primary care centre (PC)) and the number is the subject. Findings are reported in accordance with the Consolidated Criteria for Reporting Qualitative Research (COREQ) (11).
A total of 25 doctors were interviewed: 15 from primary care and 10 from the specialist centre, ages ranged from 30 to 49 years (mode 35 years). Amongst the specialists, 4 were consultant dermatologists and 6 associate consultants; in the polyclinics 7 were associate consultant/senior family physicians and 8 family physicians. The doctors had used the teledermatology service for 3–4 years.
Themes from interviews
Six themes were identified: satisfaction with teledermatology service, perceived benefits for patients, rationale for teledermatology, educational impact, challenge of virtual consultations, and service refinements for the future.
Satisfaction with teledermatology service. Both family medicine doctors and dermatologists were positive and supported the introduction of the teledermatology service, perceiving it to have benefits for patients, for themselves, and for their respective institutions.
“I think it’s a good service…it brings specialist care closer to the population, and also helps us streamline the care of our service…it also allows dialogue between a dermatologist and primary physicians who see a large majority of the patients…” (SC04)
Primary care doctors did not recall any instances where patients who were invited to attend a teledermatology consult had refused. Patients generally appeared satisfied with their virtual consultation with a dermatologist, but there were occasions when, on completion of the teledermatology consultation, the patient insisted on proceeding to an in-person consultation with a dermatologist.
“Some patients they want to see the specialist. Even with a condition that you think is treatable at the polyclinic. I think even with the photos…shown to the specialist they insist on going to the specialist. Some patients just feel that specialists provide better care with more understanding and are more knowledgeable on the condition. And some patients say that photos do not tell the whole picture as well because my photos are still only 2D. It’s not 3D and there are only certain views that you can see on the photos.” (PC02)
The aspect of teledermatology that caused most concern for the primary care clinicians was that, ultimately, a referral to the skin centre may still be needed because of difficulty making a diagnosis from the history and photographs alone, the need for tests or treatments only available at the specialist centre, or a failure to respond to the proposed management plan. Family doctors sometimes reflected whether bypassing the virtual consultation and opting for a conventional referral may be a better use of their time:
“…whether it’s appropriate. I mean we should have just referred earlier instead of having to go through the whole process [teledermatology consultation], wasting resources both from outside and from the Skin Centre [NSC] side. And at the end of the day the patient still goes to see the dermatologist.” (PC02)
Perceived benefits for patients. Doctors recognized that teledermatology offered their patients convenience, saving them money and time travelling to the specialist centre for consultations:
“The extra cost involved to see the specialist is avoided, the time for them to go so long distance is avoided…This is here [at the polyclinic], they are living nearby, so they are getting it right away…I think it’s much more better, when they have any issues they can immediately come and see us [family physician], rather than go hospital...” (PC01)
The immediate availability of an expert opinion also reduced anxiety and enabled effective management to begin promptly, enhancing the quality of care.
“…[the teledermatology service] also reduces anxiety, …..sometimes when we [family physicians] refer a patient to the National Skin Centre, I’d say it can take a few weeks to months… So having a condition whereby you do not receive treatment in time, or whereby you have an undetermined diagnosis can be potentially, make patients a bit more worried, while waiting….so having their condition better clarified in the beginning, I think that will help them with their management of the condition.” (PC11)
“I think it benefits the patients in a sense that it, allows prompt access to specialist input.” (SC04)
The healthcare professionals perceived that the key benefits of teledermatology for patients were the assurance of having their skin problem diagnosed and getting a management plan devised by a dermatologist.
“…the condition has been viewed, reviewed by a specialist…So they [the patients] feel more affirmed that it is the correct diagnosis…and it’s faster.” (PC12)
In general, the healthcare professionals opined that the teledermatology service had improved the quality of care by reducing the time taken for the patient to get a diagnosis, getting the appropriate treatment quicker, and enabling family physicians to provide holistic care.
“…some of the patients have benefited. They don’t have to travel all the way [to the NSC] because once the condition is being treated, it’s reviewed by us [family physician] and it’s under control. Then the patient is happy and their treatment is continued here. Since these patients also see us for other chronic conditions, like high blood pressure, diabetes…So there is this a continuity of care as well.” (PC02)
“So I guess it’s just that it saves their [patients] time if it’s unnecessary to visit the specialists, and they get to be treated early…Rather than waiting for the appointment for the treatment, the specialist will suggest to us [family physician] what are the treatments so that we can give it to the patient. So that we give them early treatment, rather than just wait for months to be treated.” (PC15)
“…if they [patients] can get access to a dermatology consultation, so then creams, some moisturisers that we suggest, or certain treatment options can help immediately. Because, I mean the earliest they can come in [to the NSC] is probably the day after, or the day after that, or they may not be free for a couple more days. So, then you reduce the unnecessary delay, if any.” (SC21)
Rationale for teledermatology. There were similarities and differences in the way primary care physicians and the specialists described the rationale for introducing teledermatology. Both parties discussed the potential impact on availability of specialist input (“faster access”, “reducing delay”), reduction in the number of cases referred for specialist care, and reduction on the skin centre workload. A difference was that the dermatologists spoke specifically about reducing the number of “inappropriate”, “unwarranted” or “unnecessary” referrals made to them, as illustrated in this quote:
“ ‘…cause sometimes we do get maybe referrals which can be managed in the primary care setting. So I think one of the ideas is to try to see if we can reach out more to the, you know, community maybe and we reduce the unnecessary referrals to create space for the more warranted ones.” (SC42)
The specialists also saw teledermatology as way of harmonizing the management of skin problems, across healthcare settings, and for them to better understand the case-mix of skin problems in the community, as illustrated in this quote:
“Teledermatology would help to cut down this, sort of, discordance [family physician’s vs dermatologist’s assessment], that’s the first thing. Second thing it is also a way of providing a more... holistic, sort of, community-based dermatologic service because we [dermatologists] are not based in the community.” (SC07)
Educational impact. For family physicians, a key benefit of teledermatology was the opportunity to reinforce and improve their diagnosis and management skills for common skin conditions.
“…when the specialists reply, we do learn from the cases… Some of them, we actually have some idea on how they’re managed, so, it kind of boosts our confidence, reinforces what we know. So, we have more confident in dealing with similar cases in future.” (PC05)
The impact of this deeper knowledge is reflected in the reducing frequency with which they use telemedicine:
“…now I think that even the Tele-DERM [consultations] have reduced, because I think we [family physicians] can manage skin problems of patients at the polyclinic better.” (PC15)
Within the polyclinic the educational benefits cascaded beyond those doctors actively engaged in telemedicine; examples were cited of recently acquired knowledge informing advice given to colleagues, educational events and post-graduate training:
“…we can kind of help the other colleagues in the clinic and then cut down the referrals to dermatologists” (NGP05)
“And this is a learning for us, as it is also learning to our juniors.” (PC22)
The dermatologists observed amongst polyclinic staff an increasing depth of knowledge and enhanced confidence. Their interaction with primary care also stimulated dermatologists to reflect on their own practice, for example:
“I think from their [family physician] point of view, I can see how it might be beneficial for them, because I think some of them, they, get the diagnosis right. So maybe they are looking for some more information that the diagnosis is correct. ‘Cause, there is no issue with their diagnosis, it’s just to confirm…For me [dermatologist], it makes me think about what the different diagnoses are.” (SC39)
Challenges of a virtual consultation. Dermatologists described how photographic image quality can impact the validity of their diagnosis and advice. Whilst the photographs are accompanied by a clinical history, the images are the major source of information.
“…sometimes limited by the photos that are taken …the photographs used in the teledermatology consultation are just a snapshot of the area. I can’t possibly examine the whole patient, and sometimes the photos are a bit grainy…but they’re small weaknesses.” (SC39)
As well as technical difficulties the dermatologists described the challenges of “virtual consultations”, requiring diagnostic decisions to be made with fewer clues and without the opportunity to palpate:
“…if you see this person, and then you see the healthcare giver scratching herself, then you say, could it be an infestation or a lice thing. But when you have a 2D picture and it comes to you, you would lack additional information. If the ah mah [elderly lady] comes in and she smells of medicated oil…you thought maybe, it’s an irritant problem, but you can’t smell that, on top of the touching and feeling. So those kind of multi-sensory …are gone.” (SC42)
“Difficult to diagnose and give treatment plan. This is because the quality of the photograph is not good, the tactile information is missing, and the dermoscope not available for use.” (SC43)
This challenge of advising without a face-to-face consultation was recognized by the primary care doctors, who had benefited from direct patient contact:
“It’s a suboptimal thing because they [dermatologist] are seeing only images, the photos. So that’s a disadvantage...Not seeing the patient as a whole.” (PC22)
Service refinements for the future. Suggestions were frequently shared about how to “streamline” or “simplify” the administrative referral processes, making them less onerous and less disruptive to workflow, for example:
“….if the consent form was online, or we didn’t have to physically print it out and sign it, and they keep it, sometimes it’s just the hassle of doing it as well.” (PC02)
Other suggestions related to changes in telehealth technology:
“The ideal way I could think of, is that there is a secure platform on our phone that I can just open up. Use the platform to assess my camera, take a photo, type the history into the phone, send straight-away and get an answer.” (PC13)
The polyclinic doctors spoke about the need for additional resources to maximize the impact of telemedicine. Their suggestions included expanding the polyclinic’s pharmacopoeia to include all medications recommended by the dermatologist; currently a patient might need to travel to the specialist centre’s pharmacy to collect their prescription, somewhat negating the benefits of not travelling for a consultation. Referral is also still necessary for simple treatments, such as cryotherapy for viral warts:
“…if we could expand our medication, formula, treatment. And then, as I said, if we do it, we could treat the viral warts with the cryotherapy. Then I think that would definitely benefit our telederm [teledermatology] service as well.” (PC02)
In the setting and context of this study, the types of skin conditions that the teledermatology leads refer for teledermatology to seek further advice on diagnosis and management include localized rashes of mild to moderate severity. Examples include, but are not limited to, localized dermatitis, mild-to-moderate acne vulgaris, and localized undifferentiated rashes. The referring primary care physicians and the specialist dermatologists were generally positive about the asynchronous telemedicine service between primary and secondary care. They valued how teledermatology provided patients with specialist care in a timely manner whilst remaining with their primary care provider. The healthcare professionals felt that the teledermatology service was acceptable and valued by patients, with savings of time and money compared with the traditional referral for a face-to-face specialist consultation. The resultant reduction in referrals to the specialist centre was mentioned by primary care doctors and dermatologists. However, the former discussed reducing total referrals, whereas the specialists understood the rationale to be the reduction in those referrals that did not need specialist assessment, i.e. inappropriate referrals. The potential diagnostic challenges of virtual consultation were discussed, but no actual adverse events were described. Doctors recognized that teledermatology benefited professionals as well as patients; for generalists improving their knowledge of skin disorders, and for specialists developing a better understanding of the dermatology case-mix in primary care.
The positive contribution that telemedicine can make to the dermatological education of primary care professionals was recognized by everyone. It has been estimated that, globally, less than 1 in 10 primary care consultations are for skin-related complaints, and yet it is estimated that formal teaching time for dermatology in undergraduate medical and nursing curricula may be as little as 0.24–0.3% (12). Achieving change in curricula can be difficult, and is not helped when recommendations for inclusion of new topics rarely address what can be dispensed with in order to accommodate additional material. The use of non-traditional methods of teaching, such as undergraduate and junior doctor observation of telemedicine consultation, could avoid the overcrowding of the formal didactic curriculum.
In the current study, the educational benefits of teledermatology for the dermatologists were commented on, but less often than those for primary care. In the literature, there is ambivalence towards telemedicine in the training of dermatologists. There are concerns that teledermatology impacts negatively on the case-mix available for training junior doctors because cases are sent directly to the specialist, bypassing the opportunity for review by junior staff (13). In contrast, others advocate the use of teledermatology to assess the competencies of dermatology residents (14). With the growth in telemedicine, training in telemedicine consultation needs to become an integral part of education in communication skills (15).
Based on the data from the current study, the following points could be considered when designing future teledermatology infrastructure. Firstly, incorporating a safe application that doctors can use to take photographs of the skin problem. As the cameras of mobile phones are capable of taking relatively clear photos, allowing doctors to use their mobile phones instead of a camera that is shared by several doctors is more convenient and time-saving. Secondly, specialist centres could have a teledermatology clinic that solely manages teledermatology referrals from the primary care clinics. This will reduce the waiting time for both the family physician and the patient to get a diagnosis. This will also avoid causing a backlog of patients that the specialist has to manage if the specialist has to run their own clinic.
One of our study’s strengths is that it sought the perceptions of both the referring physicians (primary care) and the receiving physicians (dermatologists). Often, studies focus on the perspectives of 1 or other group, rather than assessing the collaborative service delivered. There may be some selection bias, as not all the doctors using teledermatology agreed to be interviewed; it may be that satisfaction with the service encouraged participation, or, conversely, the opportunity to comment on its shortcomings. Another weakness is the inclusion in the sample of only doctors. This study did not capture the perceptions of other members of the team, including managers, nurses, and pharmacists, who contribute to both the development and maintenance of this service. Another limitation is that the spectrum of skin conditions that are referred for teledermatology in Singapore may not be similar to that in other countries.
Understanding the difficulties healthcare professionals encounter with telemedicine is essential, as they are the active promotors of the service, and, without their buy-in, it is difficult to sustain the service. In general, they were satisfied with the telemedicine service, but highlighted a need to streamline the referral processes and improve the quality of the transmitted images. A further reduction in specialist centre referrals could be achieved by expanding the availability of teledermatology. This study, conducted prior to the COVID-19 pandemic, documents a positive implementation experience. The pandemic has seen the rapid introduction of many telemedicine services locally, to meet the need to provide care within the home, to reduce travel, to protect providers and patients, and to facilitate social distancing. Already there have been 2 publications regarding telemedicine initiatives locally (paediatric eating disorders, renal dialysis) (16, 17) and the Ministry of Health is changing the regulatory framework and providing on-line training (18). The Ministry proposes that “Telemedicine is set to become a key feature of Singapore’s healthcare landscape”, suggesting that the COVID-19 pandemic is a catalyst for practice redesign, with in-person healthcare moving to be the second, rather than the first option, for patient care (19, 20).
The authors would like to thank the staff at the polyclinics and specialist centre that helped us with the recruitment of patients.
This study was funded by a research grant (CPHCRI1.1#001) under the Centre for Primary Health Care Research and Innovation, a partnership between the Lee Kong Chian School of Medicine, Nanyang Technological University Singapore and the National Healthcare Group Singapore.
This study was approved by the National Healthcare Group Domain Specific Review Board (Ethics 2018/01112).
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
The authors have no conflicts of interests to declare.


 Click to show fullsize
Click to show fullsize