


1Department of Dermatology, Aarhus University Hospital, Aarhus, Denmark, 2Department of Pediatrics, Division of Dermatology, University of Montreal; Centre Hospitalier Universitaire Sainte-Justine, Montreal, QC, Canada, 3Department of Dermatology and Allergology, National Expertise Center for Atopic Dermatitis, University Medical Center Utrecht, Utrecht, The Netherlands, 4Clinical Medicine, Trinity College Dublin, 5National Children’s Research Centre, Our Lady’s Children’s Hospital Crumlin, Dublin, Ireland, 6Department of Dermatology, Hospital de la Santa Creu i Sant Pau, Barcelona, Spain, 7Department of Pediatrics, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea, 8Allergy and Immunology Division, Pediatric Department, Instituto da Criança, Hospital das Clínicas, Faculdade de Medicina, Universidade de São Paulo (HC-FMUSP), São Paulo, SP, Brazil, 9Regeneron Pharmaceuticals Inc., Tarrytown, NY, USA, 10Sanofi, Chilly-Mazarin, France, and 11Sanofi Genzyme, Cambridge, MA, USA. *E-mail: Gaelle.Le-Bagousse-Bego@sanofi.com
Accepted May 26, 2021; Epub ahead of print May 27, 2021
Acta Derm Venereol 2021; 101: adv00504
doi: 10.2340/00015555-3848
Before approval of dupilumab, the only approved treatment options for adolescents with uncontrolled moderate-to-severe atopic dermatitis (AD) in the USA and EU were topical agents and systemic corticosteroids (1, 2), with cyclosporine approved in several countries for patients aged ≥16 years. Most systemic treatments for adolescents with AD are used off-label (3, 4).
Dupilumab is a fully human VelocImmune®-derived monoclonal antibody that blocks the shared receptor component for interleukin (IL)-4 and IL-13, which are key and central drivers of type 2 inflammation (5, 6). Dupilumab is approved for the treatment of patients aged ≥ 6 years with moderate-to-severe AD inadequately controlled with topical prescription therapies or when those therapies are not advisable in the USA and Canada (7, 8), and in the EU for severe AD in children 6–11 years, and moderate-to-severe AD in adults and adolescents ≥ 12 years (9). It has also been approved for adolescents in several other countries, including Brazil, Russia, South Korea, and Taiwan.
In a randomised, double-blind, parallel-group, phase 3 clinical trial (LIBERTY AD; NCT03054428), dupilumab vs placebo significantly improved AD signs, symptoms, and quality of life in adolescents with uncontrolled, moderate-to-severe AD, and showed a favourable safety profile (10). We aimed to evaluate the efficacy of dupilumab monotherapy in the subgroup of patients in LIBERTY AD who had prior use of SIS.
The LIBERTY AD study design and full inclusion criteria have been reported previously (10). Briefly, included patients were adolescents (aged ≥ 12 to < 18 years) with chronic (diagnosed ≥1 year before screening), moderate-to-severe AD (per American Academy of Dermatology criteria [11]) inadequately controlled by topical treatment or for whom topical treatment was medically inadvisable (10).
A post hoc subgroup analysis was performed according to prior use or no prior use of SIS. In each subgroup, outcomes for patients included in LIBERTY AD who received the recommended label dose of dupilumab (400 mg loading dose on day 1 followed by 200 mg every 2 weeks (q2w) or 600 mg loading dose followed by 300 mg q2w, for patient body weight < 60 kg or ≥ 60 kg, respectively) were compared with those of patients who received placebo. Endpoints were: percentage change in Eczema Area and Severity Index (EASI) score from baseline to week 16; proportion of patients achieving a ≥ 6-point improvement in Children’s Dermatology Life Quality Index (CDLQI) or Patient-Oriented Eczema Measure (POEM) scores, or ≥ 4-point reduction in peak pruritus numerical rating scale (NRS) scores from baseline to week 16; and proportion of patients with an improvement in EASI score from baseline of ≥ 75% (EASI-75) or ≥ 50% (EASI-50) at week 16.
Since this was a post hoc analysis, nominal p-values were derived by Cochran–Mantel–Haenszel test for categorical variables stratified by baseline disease severity (Investigator’s Global Assessment [IGA] = 3 vs IGA = 4) and baseline body weight (< 60 vs ≥ 60 kg), and analysis of covariance (ANCOVA) for continuous variables. p ≤ 0.05 was considered significant. Statistical analyses were performed using SAS software (version 9.4, SAS Institute, Cary, NC, USA). Randomisation was not prospectively stratified by prior use of SIS.
A total of 167 patients were included in the analysis (Table SI). Patients with prior SIS use had a numerically higher extent of disease and higher mean EASI score, and were more likely to have severe AD (IGA=4).
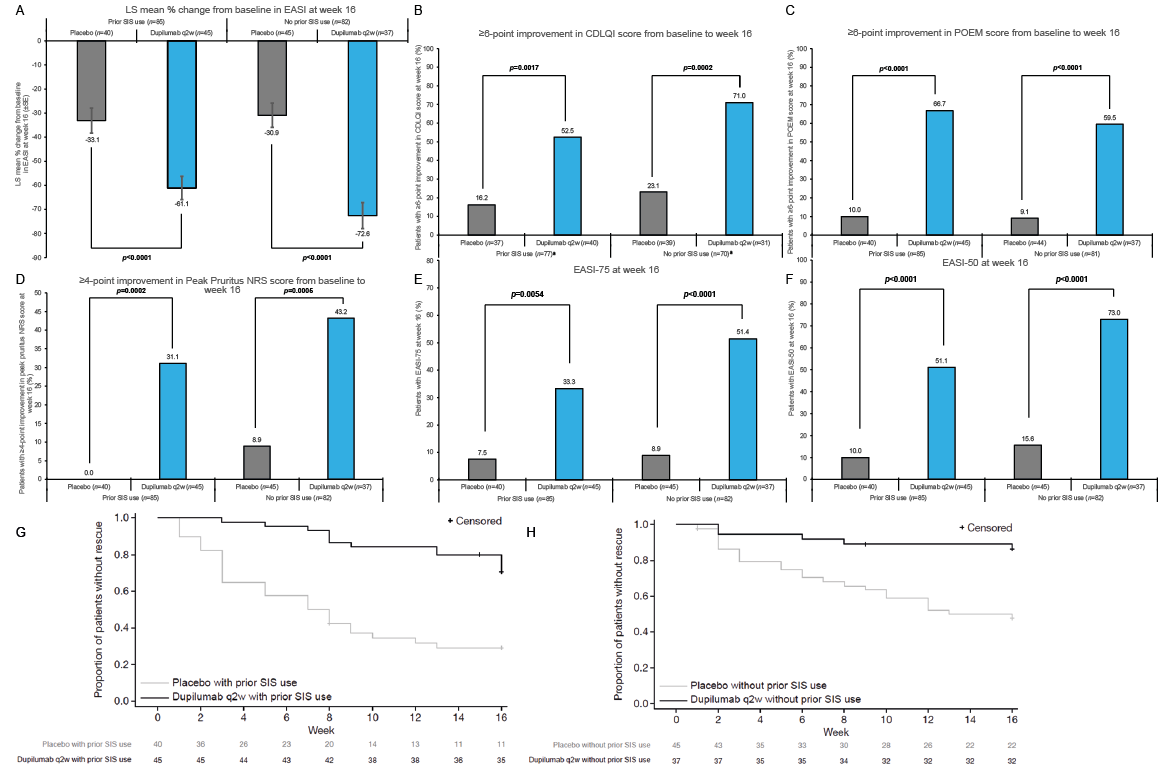
In patients with and without prior SIS use, mean percentage change in EASI score from baseline to week 16 was significantly greater for the dupilumab groups vs placebo groups (Fig. 1A), as was the proportion of patients achieving a ≥ 6-point improvement in CDLQI (Fig. 1B) or POEM (Fig. 1C) scores, or a ≥4-point improvement in peak pruritus NRS score (Fig. 1D). In addition, the proportion (%) of patients achieving EASI-75 (Fig. 1E) or EASI-50 (Fig. 1F) at week 16 was significantly greater for the dupilumab groups vs placebo groups. As mentioned earlier, patients with prior SIS use had higher disease severity at baseline compared with patients without prior SIS use. This could explain the slightly lower numerical response in both treatment and placebo arms for most endpoints in patients with prior SIS use. Nonetheless, in both the previous SIS-treated and SIS-treatment-naïve groups, a statistically significant difference vs placebo was observed.
During the study, use of rescue medication was higher among patients treated with placebo vs dupilumab q2w, both in patients with prior SIS use (70.0% vs 26.7% at week 16, respectively; Fig. 1G) and those without prior SIS use (48.9% vs 13.5% at week 16; Fig. 1H). Fig. S1 shows 2 patient cases (not necessarily representative of all patients).
In conclusion, this subgroup analysis showed that, in adolescent patients with moderate-to-severe AD, irrespective of prior SIS use, dupilumab treatment compared with placebo resulted in higher and nominally significant treatment effects across multiple efficacy endpoints.
Fig. 1. (A) Mean % change from baseline in Eczema Area and Severity Index (EASI) at week 16. Proportion of patients achieving ≥ 6-point improvement in: (B) Children’s Dermatology Life Quality Index (CDLQI) or (C) Patient-Oriented Eczema Measure (POEM) score from baseline to week 16. (D) Proportion of patients achieving ≥ 4-point improvement in peak pruritus Numerical Rating Scale (NRS) score from baseline to week 16. Proportions (%) of patients achieving (E) EASI-75 or (F) EASI-50 at week 16. Kaplan–Meier analysis of time to first rescue treatment use during the 16-week treatment period for patients with (G) and without (H) prior systemic immunosuppressant (SIS) use (dupilumab every 2 weeks (q2w) vs placebo). aAnalysed in patients with baseline CDLQI ≥6 points. EASI-75/EASI-50: improvement in EASI score from baseline of ≥75%/≥50%; IGA: Investigator’s Global Assessment; LS: least squares; SE: standard error.
Research sponsored by Sanofi and Regeneron Pharmaceuticals, Inc. Medical writing/editorial assistance provided by Yunyu Huang, PhD, of Excerpta Medica, funded by Sanofi and Regeneron Pharmaceuticals, Inc.
Conflict of interests: MD: AbbVie, Eli Lilly, LEO Pharma, Pfizer, Pierre Fabre, Regeneron Pharmaceuticals, Inc., Sanofi Genzyme – Principal Investigator, advisory board and/or consultancy. DM: AbbVie, Amgen, Eli Lilly, Janssen, LEO Pharma, Novartis, Pfizer – investigator; AbbVie, Amgen, BMS, Eli Lilly, Janssen, LEO Pharma, Novartis, Pfizer, Regeneron Pharmaceuticals, Inc., Sanofi Genzyme, UCB – Principal Investigator; AbbVie, Amgen, BMS, Novartis, Pfizer, Regeneron Pharmaceuticals, Inc., Sanofi Genzyme – speaker. MSdBW: Regeneron Pharmaceuticals, Inc., Sanofi Genzyme – Principal Investigator, advisory board, consultancy; AbbVie, Pfizer – Principal Investigator, advisory board; Eli Lilly, UCB – advisory board. ADI: AbbVie, Arena Pharmaceuticals, BenevolentAI, Chugai, Dermavant, Genentech, LEO Pharma, Lilly, Menlo Therapeutics, Novartis, Pfizer, Regeneron Pharmaceuticals, Inc., Sanofi, UCB – consultancy. EB: AbbVie, Boehringer Ingelheim, Dermira, Eli Lilly, LEO Pharma, Pfizer, Novartis – investigator; Almirall, Galderma, Novartis, Pfizer, Pierre Fabre, Regeneron Pharmaceuticals, Inc., Sanofi Genzyme – consultancy. KA: No conflict of interests to declare. APC: AbbVie, Aché, Nutricia, Sanofi – consultancy. AB, JC: Regeneron Pharmaceuticals, Inc. – employees, hold stock and/or stock options in the company. GBLB, ABR: Sanofi – employees, hold stock and/or stock options in the company.


 Click to show fullsize
Click to show fullsize