


Department of Dermatology, Peking Union Medical College Hospital, Chinese Academy of Medical Sciences and Peking Union Medical College, National Clinical Research Center for Skin and Immune Diseases, Beijing, 100730, PR China. *E-mail: mdonglai@sohu.com
An otherwise healthy 23-year-old man presented with multiple hyperkeratotic papules and comedo-like plugs with a linear distribution on his hands, feet and left knee since birth. The lesions had gradually increased in number and size, with occasional pruritus and pain. There was no family history of similar lesions. Physical examination revealed hyperkeratotic papules and pits with brown keratotic plugs on both hands (Fig. 1A, B), involving the wrists, palmar surfaces and most of the ventral digits, with extension onto the dorsal surface of the digits on both feet (Fig. 1C) including the plantar surfaces, several dorsal toes and medial and lateral borders, and the extensor side of the left knee. Most of the lesions presented with a linear distribution. No extracutaneous involvement was observed. Dermatoscopic examination showed several central whitish and brown cores surrounded by yellow crater-like rings (Fig. 1D).
What is your diagnosis? See next page for answer.
Fig. 1. (A) Multiple hyperkeratotic papules and pits with brown keratotic plugs on both hands, involving the wrists, palmar surfaces and most of the ventral digits, with extension onto the dorsal surface of the digits. (B) Linear hyperkeratotic papules and comedo-like plugs (close-up view). (C) Hyperkeratotic papules and punctate pits with whitish keratotic plugs on the both feet including the plantar surfaces, several dorsal toes and medial and lateral borders with a linear distribution. (D) Dermatoscopic examination showing several yellow crater-like openings with central whitish and brown keratotic plugs.
Acta Derm Venereol 2021; 101: adv00492.
Diagnosis: Porokeratotic eccrine ostial and dermal duct naevus
Histopathological examination showed hyperkeratosis, acanthosis, and parakeratotic columns overlying the dilated epidermal invaginations (Fig. 2A). The granular layers were thinner under the parakeratotic columns, and there were eccrine ostia in some invaginations (Fig. 2B). A diagnosis of porokeratotic eccrine ostial and dermal duct naevus (PEODDN) was made.
PEODDN is a rare, benign eccrine hamartoma. The pathogenesis is unclear, but recent work indicates that PEODDN may be caused by somatic genetic mosaicism based on its distribution along the Blaschko’s lines. Somatic heterozygous GJB2 mutations, including p.Gly45Glu, have been reported to be related to PEODDN (1), while similar germline mutation of GJB2 results in keratitis-ichthyosis-deafness (KID) syndrome (2, 3).
PEODDN is characterized by multiple asymptomatic or mildly pruritic, keratotic, whitish to brown papules or plaques and punctate pits with comedo-like plugs with a linear distribution. The lesions mostly involve the extremities unilaterally, but bilateral lesions and trunk involvement have also been reported (4). PEODDN usually appears at birth or in early childhood, although there are late-onset presentations (5, 6). Coexistent disorders have rarely been reported, including seizures, left hemiparesis and scoliosis, deafness and developmental delay, palmoplantar keratoderma, psoriasis, hyperthyroidism, polyneuropathy, breast hypoplasia and KID syndrome (4). Dermoscopy reveals yellow crater-like openings with central whitish and brown keratotic plugs (5). Histopathologically, hyperkeratosis, acanthosis and parakeratotic columns overlying dilated eccrine ducts and acrosyringia are pathognomonic for PEODDN. However, the absence of dermal eccrine duct abnormalities below the dilated ostia in PEODDN, as in the case described here, has been reported (7). There may be thinner granular layers beneath parakeratotic columns, and vacuolated and dyskeratotic keratinocytes within the epidermal invagination (6). Differential diagnoses include linear verrucous epidermal naevus, punctate palmoplantar keratoderma, linear and punctate porokeratosis, naevus comedonicus, verruca vulgaris and linear psoriasis, but lack of characteristic parakeratotic columns and the association with eccrine ducts and ostia helps to exclude these diseases (4, 7).
Different treatment modalities, including topical steroids, calcipotriol, retinoids, urea ointment, salicylic acid, systemic acitretin, phototherapy and cryotherapy, have showed limited success (6). Surgical excision may be considered for small and localized lesions. Carbon dioxide laser therapy and combined erbium/carbon dioxide laser seem to be efficient in some patients (4, 7). Also, in some cases, PEODDN responds to topical tazarotene, dithranol short-contact treatment and photodynamic therapy (4). Multiple treatments may be required for the recurrence of treated lesions. Regular follow-up is important due to possible progression to squamous cell carcinoma in some patients (8).
Fig. 2. (A) Skin biopsy from the left palm (haematoxylin-eosin stain, original magnification ×20). (B) Thinner granular layers and dilated eccrine ostia under the parakeratotic columns (haematoxylin-eosin stain, original magnification ×200).


 Click to show fullsize
Click to show fullsize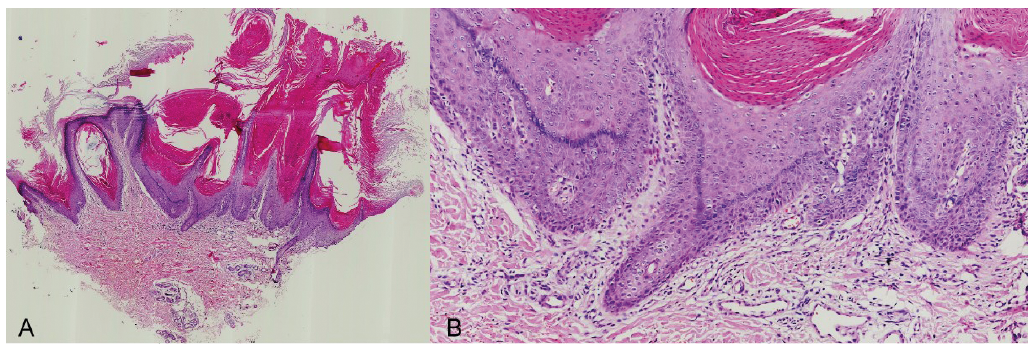 Click to show fullsize
Click to show fullsize